天津医药 ›› 2025, Vol. 53 ›› Issue (11): 1158-1164.doi: 10.11958/20252455
吴梦琳( ), 马芳, 杨亚菲
), 马芳, 杨亚菲
收稿日期:2025-07-10
修回日期:2025-08-13
出版日期:2025-11-15
发布日期:2025-11-19
作者简介:吴梦琳(1995),女,医师,主要从事浅表及血管方向超声方面研究。E-mail:基金资助:
WU Menglin(), MA Fang, YANG Yafei
Received:2025-07-10
Revised:2025-08-13
Published:2025-11-15
Online:2025-11-19
吴梦琳, 马芳, 杨亚菲. 超声AI联合BRAF V600E基因检测对甲状腺结节良恶性与侵袭性的诊断效能[J]. 天津医药, 2025, 53(11): 1158-1164.
WU Menglin, MA Fang, YANG Yafei. Diagnostic efficacy of ultrasonic artificial intelligence combined with BRAF V600E gene testing in differentiating benign-malignant and invasive thyroid nodules[J]. Tianjin Medical Journal, 2025, 53(11): 1158-1164.
摘要:
目的 探讨超声人工智能(AI)与苏氨酸特异性激酶(BRAF)V600E基因的联合检测在甲状腺结节良恶性与侵袭性评估中的应用价值。方法 选取甲状腺恶性结节(恶性组)、甲状腺良性结节(良性组)患者各150例,根据恶性组的病理诊断是否涉及包膜、血管、神经侵犯或淋巴结转移分为侵袭组(66例)和未侵袭组(84例)。收集各组一般临床特征、超声AI指标及BRAF V600E基因检测结果。统计超声AI、BRAF V600E基因检测与甲状腺结节术后病理诊断的差异。受试者工作特征(ROC)曲线及Delong检验评估超声AI、BRAF V600E基因单项及联合检测的诊断效能。结果 恶性组结节最大直径>1 cm、实性结构、极低回声/低回声、微钙化、边界模糊、形态不规则、纵横比>1、内部/混合血流分布、Ⅲ—Ⅴ级血流丰富度的比例均大于良性组。侵袭组结节最大直径>1 cm、实性结构、极低回声/低回声、微钙化、边界模糊、形态不规则、内部/混合血流分布、Ⅲ—Ⅴ级血流丰富度的比例均大于未侵袭组(P<0.05)。超声AI诊断甲状腺恶性结节的敏感度为90.00%,特异度为80.67%;超声AI诊断甲状腺恶性结节合并侵袭性的敏感度为84.85%,特异度为83.33%。BRAF V600E基因诊断甲状腺恶性结节的敏感度为72.67%,特异度为90.00%;BRAF V600E基因诊断甲状腺恶性结节合并侵袭性的敏感度为74.24%,特异度为88.10%。受试者工作特征(ROC)曲线显示,超声AI、BRAF V600E基因单项及联合检测诊断甲状腺恶性结节的AUC(95%CI)分别为0.853(0.807~0.900)、0.813(0.762~0.864)、0.941(0.917~0.966),且联合检测的AUC大于超声AI、BRAF V600E基因单项检测(P<0.05);超声AI、BRAF V600E基因单项及联合检测诊断甲状腺恶性结节合并侵袭性的AUC(95%CI)分别为0.841(0.773~0.909)、0.812(0.737~0.886)、0.924(0.880~0.967),且联合检测的AUC大于超声AI、BRAF V600E基因单项检测(P<0.05)。结论 超声AI与BRAF V600E基因的联合检测显著优化了甲状腺结节良恶性与侵袭性的诊断效能。
中图分类号:
| 组别 | n | 性别(男/女) | 年龄/岁 | 辐射接触史 |
|---|---|---|---|---|
| 良性组 | 150 | 52/98 | 46.00(36.00,59.00) | 2(1.33) |
| 恶性组 | 150 | 57/93 | 49.00(39.00,60.00) | 7(4.67) |
| χ2或Z | 0.360 | 1.278 | 1.833 | |
| 组别 | 碘暴露史 | 甲状腺疾病史 | 甲状腺疾病家族史 | |
| 良性组 | 3(2.00) | 23(15.33) | 18(12.00) | |
| 恶性组 | 9(6.00) | 32(21.33) | 21(14.00) | |
| χ2 | 3.125 | 1.803 | 0.265 | |
表1 良性组与恶性组一般临床特征比较
Tab.1 Comparison of general clinical characteristics between the benign group and the malignant group
| 组别 | n | 性别(男/女) | 年龄/岁 | 辐射接触史 |
|---|---|---|---|---|
| 良性组 | 150 | 52/98 | 46.00(36.00,59.00) | 2(1.33) |
| 恶性组 | 150 | 57/93 | 49.00(39.00,60.00) | 7(4.67) |
| χ2或Z | 0.360 | 1.278 | 1.833 | |
| 组别 | 碘暴露史 | 甲状腺疾病史 | 甲状腺疾病家族史 | |
| 良性组 | 3(2.00) | 23(15.33) | 18(12.00) | |
| 恶性组 | 9(6.00) | 32(21.33) | 21(14.00) | |
| χ2 | 3.125 | 1.803 | 0.265 | |
| 组别 | n | 性别(男/女) | 年龄/岁 | 辐射接触史 |
|---|---|---|---|---|
| 未侵袭组 | 84 | 27/57 | 47.50(38.25,58.75) | 2(2.38) |
| 侵袭组 | 66 | 30/36 | 50.50(39.00,61.00) | 5(7.58) |
| χ2或Z | 2.780 | 0.922 | 1.226 | |
| 组别 | 碘暴露史 | 甲状腺疾病史 | 甲状腺疾病家族史 | |
| 未侵袭组 | 3(3.57) | 14(16.67) | 11(13.10) | |
| 侵袭组 | 6(9.09) | 18(27.27) | 10(15.15) | |
| χ2 | 1.138 | 2.477 | 0.130 | |
表2 未侵袭组与侵袭组一般临床特征比较
Tab.2 Comparison of general clinical characteristics between the non-invasive group and the invasive group
| 组别 | n | 性别(男/女) | 年龄/岁 | 辐射接触史 |
|---|---|---|---|---|
| 未侵袭组 | 84 | 27/57 | 47.50(38.25,58.75) | 2(2.38) |
| 侵袭组 | 66 | 30/36 | 50.50(39.00,61.00) | 5(7.58) |
| χ2或Z | 2.780 | 0.922 | 1.226 | |
| 组别 | 碘暴露史 | 甲状腺疾病史 | 甲状腺疾病家族史 | |
| 未侵袭组 | 3(3.57) | 14(16.67) | 11(13.10) | |
| 侵袭组 | 6(9.09) | 18(27.27) | 10(15.15) | |
| χ2 | 1.138 | 2.477 | 0.130 | |
| 组别 | 结节数量 | 结节位置 | 最大直径 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单发 | 多发 | 左叶 | 右叶 | 峡部 | 混合 | ≤1 cm | >1 cm | ||||||||||
| 良性组 | 90(60.00) | 60(40.00) | 60(40.00) | 58(38.67) | 8(5.33) | 24(16.00) | 97(64.67) | 53(35.33) | |||||||||
| 恶性组 | 102(68.00) | 48(32.00) | 54(36.00) | 63(42.00) | 15(10.00) | 18(12.00) | 51(40.00) | 99(66.00) | |||||||||
| χ2 | 2.083 | 3.510 | 28.218** | ||||||||||||||
| 组别 | 结节结构 | 回声类型 | 钙化类型 | 边界 | |||||||||||||
| 囊性 | 实性 | 无回声 | 极低回声/ 低回声 | 等回声/ 高回声 | 混合回声 | 无 | 微钙化 | 粗钙化 | 清晰 | 模糊 | |||||||
| 良性组 | 105(70.00) | 45(30.00) | 24(16.00) | 45(30.00) | 72(48.00) | 9(6.00) | 90(60.00) | 14(9.33) | 46(30.67) | 120(80.00) | 30(20.00) | ||||||
| 恶性组 | 7(4.67) | 143(95.33) | 3(2.00) | 126(84.00) | 15(10.00) | 6(4.00) | 32(21.33) | 103(68.67) | 15(10.00) | 33(22.00) | 117(78.00) | ||||||
| χ2 | 136.835** | 92.647** | 111.029** | 100.960** | |||||||||||||
| 组别 | 形态 | 纵横比 | 血流分布 | 血流丰富度 | |||||||||||||
| 规则 | 不规则 | ≤1 | >1 | 周边 | 内部/混合 | Ⅰ—Ⅱ级 | Ⅲ—Ⅴ级 | ||||||||||
| 良性组 | 103(68.67) | 47(31.33) | 134(89.33) | 16(10.67) | 82(54.67) | 68(45.33) | 115(76.67) | 35(23.33) | |||||||||
| 恶性组 | 50(33.33) | 100(66.67) | 49(32.67) | 101(67.33) | 20(13.33) | 130(86.67) | 53(35.33) | 97(64.67) | |||||||||
| χ2 | 37.468** | 101.233** | 57.100** | 52.002** | |||||||||||||
表3 甲状腺结节良性组与恶性组的超声AI特征比较 [n=150,例(%)]
Tab.3 Comparison of ultrasound AI features between the two groups
| 组别 | 结节数量 | 结节位置 | 最大直径 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单发 | 多发 | 左叶 | 右叶 | 峡部 | 混合 | ≤1 cm | >1 cm | ||||||||||
| 良性组 | 90(60.00) | 60(40.00) | 60(40.00) | 58(38.67) | 8(5.33) | 24(16.00) | 97(64.67) | 53(35.33) | |||||||||
| 恶性组 | 102(68.00) | 48(32.00) | 54(36.00) | 63(42.00) | 15(10.00) | 18(12.00) | 51(40.00) | 99(66.00) | |||||||||
| χ2 | 2.083 | 3.510 | 28.218** | ||||||||||||||
| 组别 | 结节结构 | 回声类型 | 钙化类型 | 边界 | |||||||||||||
| 囊性 | 实性 | 无回声 | 极低回声/ 低回声 | 等回声/ 高回声 | 混合回声 | 无 | 微钙化 | 粗钙化 | 清晰 | 模糊 | |||||||
| 良性组 | 105(70.00) | 45(30.00) | 24(16.00) | 45(30.00) | 72(48.00) | 9(6.00) | 90(60.00) | 14(9.33) | 46(30.67) | 120(80.00) | 30(20.00) | ||||||
| 恶性组 | 7(4.67) | 143(95.33) | 3(2.00) | 126(84.00) | 15(10.00) | 6(4.00) | 32(21.33) | 103(68.67) | 15(10.00) | 33(22.00) | 117(78.00) | ||||||
| χ2 | 136.835** | 92.647** | 111.029** | 100.960** | |||||||||||||
| 组别 | 形态 | 纵横比 | 血流分布 | 血流丰富度 | |||||||||||||
| 规则 | 不规则 | ≤1 | >1 | 周边 | 内部/混合 | Ⅰ—Ⅱ级 | Ⅲ—Ⅴ级 | ||||||||||
| 良性组 | 103(68.67) | 47(31.33) | 134(89.33) | 16(10.67) | 82(54.67) | 68(45.33) | 115(76.67) | 35(23.33) | |||||||||
| 恶性组 | 50(33.33) | 100(66.67) | 49(32.67) | 101(67.33) | 20(13.33) | 130(86.67) | 53(35.33) | 97(64.67) | |||||||||
| χ2 | 37.468** | 101.233** | 57.100** | 52.002** | |||||||||||||
| 组别 | n | 结节数量 | 结节位置 | 最大直径 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单发 | 多发 | 左叶 | 右叶 | 峡部 | 混合 | ≤1 cm | >1 cm | |||||||||||||||||
| 未侵袭组 | 84 | 62(73.81) | 22(26.19) | 32(38.10) | 33(39.29) | 7(8.33) | 12(14.29) | 35(41.67) | 49(58.33) | |||||||||||||||
| 侵袭组 | 66 | 40(60.61) | 26(39.39) | 22(33.33) | 30(45.45) | 8(12.12) | 6(9.09) | 16(24.24) | 50(75.76) | |||||||||||||||
| χ2 | 2.961 | 1.929 | 5.001* | |||||||||||||||||||||
| 组别 | 结节结构 | 回声类型 | 钙化类型 | 边界 | ||||||||||||||||||||
| 囊性 | 实性 | 无回声 | 极低回声/低回声 | 等回声/ 高回声 | 混合回声 | 无 | 微钙化 | 粗钙化 | 清晰 | 模糊 | ||||||||||||||
| 未侵袭组 | 7(8.33) | 77(91.67) | 3(3.57) | 64(76.19) | 13(15.48) | 4(4.76) | 26(30.95) | 45(53.57) | 13(15.48) | 29(34.52) | 55(65.48) | |||||||||||||
| 侵袭组 | 0 | 66(100.00) | 0 | 62(93.94) | 2(3.03) | 2(3.03) | 6(9.09) | 58(87.88) | 2(3.03) | 4(6.06) | 62(93.94) | |||||||||||||
| χ2 | 4.048* | 11.719** | 20.340** | 17.449** | ||||||||||||||||||||
| 组别 | 形态 | 纵横比 | 血流分布 | 血流丰富度 | ||||||||||||||||||||
| 规则 | 不规则 | ≤1 | >1 | 周边 | 内部/混合 | Ⅰ—Ⅱ级 | Ⅲ—Ⅴ级 | |||||||||||||||||
| 未侵袭组 | 38(45.24) | 46(54.76) | 29(34.52) | 55(65.48) | 16(19.05) | 68(80.95) | 45(53.57) | 39(46.43) | ||||||||||||||||
| 侵袭组 | 12(18.18) | 54(81.82) | 20(30.30) | 46(69.70) | 4(6.06) | 62(93.94) | 8(12.12) | 58(87.88) | ||||||||||||||||
| χ2 | 12.175** | 0.299 | 5.395* | 27.792** | ||||||||||||||||||||
表4 甲状腺结节未侵袭组与侵袭性组的超声AI特征比较 [例(%)]
Tab.4 Comparison of ultrasound AI characteristics between the non-invasive group and the invasive group of thyroid nodules
| 组别 | n | 结节数量 | 结节位置 | 最大直径 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单发 | 多发 | 左叶 | 右叶 | 峡部 | 混合 | ≤1 cm | >1 cm | |||||||||||||||||
| 未侵袭组 | 84 | 62(73.81) | 22(26.19) | 32(38.10) | 33(39.29) | 7(8.33) | 12(14.29) | 35(41.67) | 49(58.33) | |||||||||||||||
| 侵袭组 | 66 | 40(60.61) | 26(39.39) | 22(33.33) | 30(45.45) | 8(12.12) | 6(9.09) | 16(24.24) | 50(75.76) | |||||||||||||||
| χ2 | 2.961 | 1.929 | 5.001* | |||||||||||||||||||||
| 组别 | 结节结构 | 回声类型 | 钙化类型 | 边界 | ||||||||||||||||||||
| 囊性 | 实性 | 无回声 | 极低回声/低回声 | 等回声/ 高回声 | 混合回声 | 无 | 微钙化 | 粗钙化 | 清晰 | 模糊 | ||||||||||||||
| 未侵袭组 | 7(8.33) | 77(91.67) | 3(3.57) | 64(76.19) | 13(15.48) | 4(4.76) | 26(30.95) | 45(53.57) | 13(15.48) | 29(34.52) | 55(65.48) | |||||||||||||
| 侵袭组 | 0 | 66(100.00) | 0 | 62(93.94) | 2(3.03) | 2(3.03) | 6(9.09) | 58(87.88) | 2(3.03) | 4(6.06) | 62(93.94) | |||||||||||||
| χ2 | 4.048* | 11.719** | 20.340** | 17.449** | ||||||||||||||||||||
| 组别 | 形态 | 纵横比 | 血流分布 | 血流丰富度 | ||||||||||||||||||||
| 规则 | 不规则 | ≤1 | >1 | 周边 | 内部/混合 | Ⅰ—Ⅱ级 | Ⅲ—Ⅴ级 | |||||||||||||||||
| 未侵袭组 | 38(45.24) | 46(54.76) | 29(34.52) | 55(65.48) | 16(19.05) | 68(80.95) | 45(53.57) | 39(46.43) | ||||||||||||||||
| 侵袭组 | 12(18.18) | 54(81.82) | 20(30.30) | 46(69.70) | 4(6.06) | 62(93.94) | 8(12.12) | 58(87.88) | ||||||||||||||||
| χ2 | 12.175** | 0.299 | 5.395* | 27.792** | ||||||||||||||||||||
| 超声AI | 术后病理 | 术后病理 | ||||
|---|---|---|---|---|---|---|
| 恶性 | 良性 | 合计 | 侵袭 | 未侵袭 | 合计 | |
| ≥0.5 | 135 | 29 | 164 | 56 | 14 | 70 |
| <0.5 | 15 | 121 | 136 | 10 | 70 | 80 |
| 合计 | 150 | 150 | 300 | 66 | 84 | 150 |
表5 超声AI诊断与甲状腺结节术后病理情况比较 (例)
Tab.5 Comparion of ultrasound AI diagnosis and postoperative pathological conditions of thyroid nodules
| 超声AI | 术后病理 | 术后病理 | ||||
|---|---|---|---|---|---|---|
| 恶性 | 良性 | 合计 | 侵袭 | 未侵袭 | 合计 | |
| ≥0.5 | 135 | 29 | 164 | 56 | 14 | 70 |
| <0.5 | 15 | 121 | 136 | 10 | 70 | 80 |
| 合计 | 150 | 150 | 300 | 66 | 84 | 150 |
| BRAF V600E | 术后病理 | 术后病理 | ||||
|---|---|---|---|---|---|---|
| 恶性 | 良性 | 合计 | 侵袭 | 未侵袭 | 合计 | |
| 阳性 | 109 | 15 | 124 | 49 | 10 | 59 |
| 阴性 | 41 | 135 | 176 | 17 | 74 | 72 |
| 合计 | 150 | 150 | 300 | 66 | 84 | 150 |
表6 BRAF V600E基因诊断与甲状腺结节的术后病理情况比较 (例)
Tab.6 Comparison of BRAF V600E gene diagnosis and postoperative pathological conditions of thyroid nodules
| BRAF V600E | 术后病理 | 术后病理 | ||||
|---|---|---|---|---|---|---|
| 恶性 | 良性 | 合计 | 侵袭 | 未侵袭 | 合计 | |
| 阳性 | 109 | 15 | 124 | 49 | 10 | 59 |
| 阴性 | 41 | 135 | 176 | 17 | 74 | 72 |
| 合计 | 150 | 150 | 300 | 66 | 84 | 150 |
| 指标 | AUC | 95%CI | 约登指数 |
|---|---|---|---|
| 超声AI | 0.853 | 0.807~0.900 | 0.707 |
| BRAF V600E基因 | 0.813 | 0.762~0.864 | 0.627 |
| 联合检测 | 0.941 | 0.917~0.966 | 0.727 |
表7 超声AI联合BRAF V600E基因检测对甲状腺恶性结节的诊断效能
Tab.7 Diagnostic efficacy of combined AI ultrasound and BRAF V600E testing for malignant thyroid nodules
| 指标 | AUC | 95%CI | 约登指数 |
|---|---|---|---|
| 超声AI | 0.853 | 0.807~0.900 | 0.707 |
| BRAF V600E基因 | 0.813 | 0.762~0.864 | 0.627 |
| 联合检测 | 0.941 | 0.917~0.966 | 0.727 |
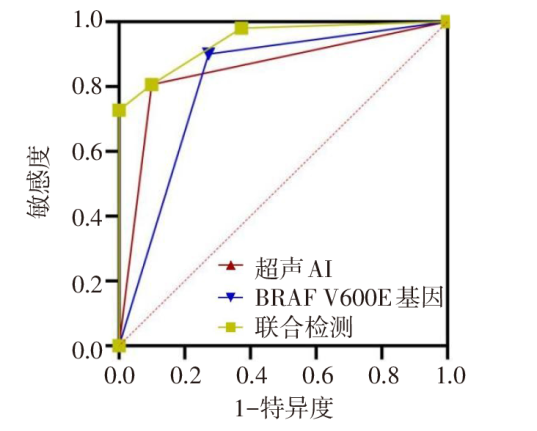
图1 超声AI联合BRAF V600E基因检测诊断甲状腺恶性结节的ROC曲线
Fig.1 ROC curve of combined AI ultrasound and BRAF V600E testing for predicting malignant thyroid nodules
| 指标 | AUC | 95%CI | 约登指数 |
|---|---|---|---|
| 超声AI | 0.841 | 0.773~0.909 | 0.681 |
| BRAF V600E基因 | 0.812 | 0.737~0.886 | 0.623 |
| 联合检测 | 0.924 | 0.880~0.967 | 0.774 |
表8 超声AI联合BRAF V600E基因检测对甲状腺恶性结节合并侵袭性的诊断效能
Tab.8 Diagnostic efficacy of combined AI ultrasound and BRAF V600E testing for invasive malignant thyroid nodules
| 指标 | AUC | 95%CI | 约登指数 |
|---|---|---|---|
| 超声AI | 0.841 | 0.773~0.909 | 0.681 |
| BRAF V600E基因 | 0.812 | 0.737~0.886 | 0.623 |
| 联合检测 | 0.924 | 0.880~0.967 | 0.774 |
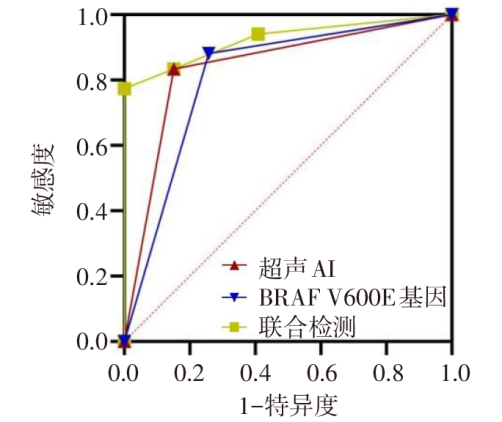
图2 超声AI联合BRAF V600E基因检测诊断甲状腺恶性结节合并侵袭性的ROC曲线
Fig.2 ROC curve of combined AI ultrasound and BRAF V600E testing for predicting invasive malignant thyroid nodules
| [1] | 中国医师协会外科医师分会甲状腺外科专家工作组, 中国研究型医院学会甲状腺疾病专业委员会, 等. 超声引导下甲状腺结节和颈部淋巴结细针穿刺活检中国专家共识及操作指南(2025版)[J]. 中国实用外科杂志, 2025, 45(1):34-41. |
| Expert Working Group of Thyroid Association,College of Surgeons, Chinese Medical Doctor Association, Chinese Research Hospital Association Thyroid Disease Committee, et al. Chinese experts consensus and operational guidelines on ultrasound guided fine-needle aspiration biopsy of thyroid nodule and cervical lymph node(2025 edition)[J]. Chinese Journal of Practical Surgery, 2025, 45(1):34-41. doi:10.19538/j.cjps.issn1005-2208.2025.01.05. | |
| [2] | 杨桃, 全艳, 张加孟, 等. 甲状腺结节细针穿刺细胞学联合BRAF基因检测在甲状腺良恶性肿瘤鉴别诊断中的应用价值[J]. 天津医药, 2025, 53(9):972-976. |
| YANG T, QUAN Y, ZHANG J M, et al. Application value of thyroid nodule fine needle aspiration cytology combined with BRAF gene detection in the differential diagnosis of benign and malignant thyroid tumors[J]. Tianjin Med J, 2025, 53(9):972-976. doi:10.11958/20241258. | |
| [3] | 蔡文卿, 崔灿, 刘洁, 等. BRAFV600E基因突变检测在细针穿刺细胞学良性甲状腺结节中的应用价值[J]. 中国普通外科杂志, 2024, 33(11):1786-1793. |
| CAI W Q, CUI C, LIU J, et al. The application value of BRAFV600Egene mutation testing in fine-needle aspiration biopsy diagnosed benign thyroid nodules[J]. China Journal of General Surgery, 2024, 33(11):1786-1793. doi:10.7659/j.issn.1005-6947.2024.11.005. | |
| [4] | 刘凌晓, 董怡. 人工智能技术在甲状腺结节诊断及预测淋巴结转移中的应用[J]. 介入放射学杂志, 2021, 30(4):4. |
| LIU L X, DONG Y. Application of artificial inteligenee technology in diagnosing thyroid nodules and predicting lymphnode metastasis[J]. J Intervent Radiol, 2021, 30(4):4. doi:10.3969/j.issn.1008-794X.2021.04.001. | |
| [5] | MENDES J M, ELSHEIKH T M, DI MARCO J, et al. Are there specific cytologic features that can predict BRAFV600E mutational status of papillary thyroid carcinoma in fine-needle aspiration specimens?[J]. Diagn Cytopathol. 2024, 52(6):295-302. doi:10.1002/dc.25290. |
| [6] | DURANTE C, HEGEDüS L, CZARNIECKA A, et al. 2023 European Thyroid Association Clinical Practice Guidelines for thyroid nodule management[J]. Eur Thyroid J, 2023, 12(5):e230067. doi:10.1530/ETJ-23-0067. |
| [7] | 刘江云, 李利霞, 刘新羽. 超声AI、弹性应变率及TSH检测在甲状腺结节良恶性鉴别中的应用研究[J]. 临床和实验医学杂志, 2024, 23(22):2438-2442. |
| LIU J Y, LI L X, LIU X Y. Application of ultrasonic AI,elastic strain rate and TSH detection in differential diagnosis of benign and malignant thyroid nodules[J]. Journal of Clinical and Experimental Medicine, 2024, 23(22):2438-2442. doi:10.3969/j.issn.1671-4695.2024.22.023. | |
| [8] | 中华医学超声杂志(电子版)编辑委员会浅表器官学组. 甲状腺结节超声诊断规范[J]. 中华医学超声杂志(电子版), 2017, 14(4):241-244. |
| Editorial Board of Chinese Journal of Medical Ultrasound(Electronic Edition),Superficial Organ Subgroup. Standardization for thyroid nodule ultrasound diagnosis[J]. Chin J Med Ultrasotmd(Electronic Edition), 2017, 14(4):241-244. doi:10.3877/cma.j.issn.1672-6448.2017.04.001. | |
| [9] | 广东省医学教育协会甲状腺专业委员会, 广东省基层医药学会细胞病理与分子诊断专业委员会. 甲状腺癌基因检测与临床应用广东专家共识(2020版)[J]. 中华普通外科学文献(电子版), 2020, 14(3):161-168. |
| Guangdong Medical Education Association Thyroid Specialized Committee, Guangdong Primary Healthcare Association Cellular Pathology and Molecular Diagnosis Specialized Committee. Guangdong expert consensus on gene testing and clinical application in thyroid cancer(Version 2020)[J]. Chin Arch Gen Surg(Electronic Edition), 2020, 14(3):161-168. doi:10.3877/cma.j.issn.1674-0793.2020.03.001. | |
| [10] | 杨蕊菲, 刘葆婧, 武曼, 等. 血浆ctDNA中HOXA7、SOX17甲基化联合影像学指标在肺癌早诊中的应用研究[J]. 重庆医科大学学报, 2025, 50(3):403-408. |
| YANG R F, LIU B J, WU M, et al. Application of radiological indicators combined with the methylation of HOXA7 and SOX17 in plasma circulating tumor DNA in the early diagnosis of lung cancer[J]. Journal of Chongqing Medical University, 2025, 50(3):403-408. doi:10.13406/j.cnki.cyxb.003715. | |
| [11] | 李晓宇, 刘利平, 辛雨薇, 等. 人工智能软件联合超声造影鉴别诊断甲状腺良、恶性结节[J]. 中国医学影像学杂志, 2023, 31(3):226-230. |
| LI X Y, LIU L P, XIN Y W, et al. Diagnosis of artificial intelligence software combined with contrast-enhanced ultrasound in differentiating benign from malignant thyroid nodules[J]. Chinese Journal of Medical Imaging, 2023, 31(3):226-230. doi:10.3969/j.issn.1005-5185.2023.03.007. | |
| [12] | 张萌, 金壮, 赵蕙琳, 等. 多模态超声联合临床特征建立对甲状腺结节良恶性诊断的预测模型[J]. 中国医学影像学杂志, 2024, 32(1):14-20. |
| ZHANG M, JIN Z, ZHAO H L, et al. Establishment of a predictive model for the diagnosis of benign and malignant thyroid nodulesvia multimodal ultrasound combined with thyroid hormone[J]. Chinese Journal of Medical Imaging, 2024, 32(1):14-20. doi:10.3969/j.issn.1005-5185.2024.01.003. | |
| [13] | FU J, LIN J, DAI Z, et al. Hypoxia-associated autophagy flux dysregulation in human cancers[J]. Cancer Lett, 2024, 590(5):216823. doi:10.1016/j.canlet.2024.216823. |
| [14] | 赵玲, 马步云. 甲状腺髓样癌和甲状腺乳头状癌的超声特征研究[J]. 现代肿瘤医学, 2023, 31(16):3010-3014. |
| ZHAO L, MA B Y. Ultrasonographic features study of medullary thyroid carcinoma and papillaithyroid carcinoma[J]. Modern Oncology, 2023, 31(16):3010-3014. doi:10.3969/j.issn.1672-4992.2023.16.011. | |
| [15] | 侯婷婷, 夏燕妮, 张红伟. C-TIRADS联合cfDNA鉴别诊断甲状腺结节价值及临床效用评价[J]. 河北医药, 2023, 45(18):2736-2740. |
| HOU T T, XIA Y N, ZHANG H W. Evaluation of the value and clinical application of the Chinese thyroid imaging reports and data systems combined with circulating free DNA detection in the differential diagnosis of thyroid nodules[J]. Hebei Medical Journal, 2023, 45(18):2736-2740. doi:10.3969/j.issn.1002-7386.2023.18.003. | |
| [16] | 周芳, 张刚, 李欢, 等. 甲状腺乳头状癌超声图像特征及BRAF V600E突变与颈部淋巴结转移的关系[J]. 临床超声医学杂志, 2023, 25(4):289-293. |
| ZHOU F, ZHANG G, LI H, et al. Correlation of ultrasonographic characteristics,BRAF V600E gene mutation and cervical lymph node metastasis in papillary thyroid carcinoma[J]. J Clin Ultrasound in Med, 2023, 25(4):289-293. doi:10.3969/j.issn.1008-6978.2023.04.011. | |
| [17] | VIMALRAJ S. A concise review of VEGF,PDGF,FGF,Notch,angiopoietin,and HGF signalling in tumor angiogenesis with a focus on alternative approaches and future directions[J]. Int J Biol Macromol, 2022, 221(11):1428-1438. doi:10.1016/j.ijbiomac.2022.09.129. |
| [18] | ZOU M, AL-YAHYA S, AL-ALWAN M, et al. β-catenin attenuation leads to up-regulation of activating NKG2D ligands and tumor regression in BrafV600E-driven thyroid cancer cells[J]. Front Immunol, 2023, 14(7):1171816. doi:10.3389/fimmu.2023.1171816. |
| [19] | 常晨, 房国栋, 雷建园, 等. 免疫组化检测BRAF V600E突变在甲状腺乳头状癌中的应用[J]. 国际遗传学杂志, 2022, 45(6):441-447. |
| CHANG C, FANG G D, LEI J Y, et al. Immunohistochemical detection of BRAF V600E mutation in papillary thyroid cancer[J]. International Journal of Genetics, 2022, 45(6):441-447. doi:10.3760/cma.j.cn231536-20220801-00072. | |
| [20] | 吴宪吉, 肖思齐, 沈珂羽, 等. BRAF V600E突变与甲状腺乳头状癌临床病理特征关系的研究进展[J]. 中国实验诊断学, 2024, 28(2):219-223. |
| WU X J, XIAO S Q, SHEN K Y, et al. Research progress on the relationship between BRAF V600E mutation and clinicopathological features of papillary thyroid carcinoma[J]. Chinese Journal of Laboratory Diagnosis, 2024, 28(2):219-223. doi:10.3969/j.issn.1007-4287.2024.02.021. | |
| [21] | 赵思童, 胡晓东, 许怀瑾, 等. 桥本甲状腺炎超声与病理学诊断的一致性分析[J]. 解放军医学杂志, 2023, 48(5):530-536. |
| ZHAO S T, HU X D, XU H J, et al. Analysis of consistency between ultrasound and pathological diagnosis of Hashimoto thyroiditis[J]. Med J Chin PLA, 2023, 48(5):530-536. doi:10.11855/j.issn.0577-7402.2023.05.0530. |
| [1] | 朱梦雅, 霍莹, 郭志鹏, 刘洋, 刘刚. 单纯经超声引导的房间隔缺损封堵术安全性及有效性研究[J]. 天津医药, 2026, 54(3): 309-313. |
| [2] | 杨桃, 全艳, 张加孟, 谢清耘, 黄麟洲. 甲状腺结节细针穿刺细胞学联合BRAF基因检测在甲状腺良恶性肿瘤鉴别诊断中的应用价值[J]. 天津医药, 2025, 53(9): 972-975. |
| [3] | 刘志远, 杨声飞, 钱释然, 邓忆莲, 黎东伟, 李君久. 胸乳入路腔镜甲状腺术后早期低钙血症的危险因素分析及预测模型构建[J]. 天津医药, 2025, 53(8): 826-830. |
| [4] | 赵志刚, 刘辉, 刘红梅. 重症乙型流感病毒性肺炎合并侵袭性肺曲霉菌病的影响因素分析[J]. 天津医药, 2025, 53(7): 736-740. |
| [5] | 王明扬, 李丽, 李玲玲, 吴钺. 能谱CT定量分析在甲状腺恶性结节诊断及颈部淋巴结转移评估中的应用[J]. 天津医药, 2025, 53(6): 654-658. |
| [6] | 麦湘湘, 李柠肖, 游咏. 超声测量的咬肌增厚率对帕金森病患者发生吞咽困难的诊断价值[J]. 天津医药, 2025, 53(6): 659-664. |
| [7] | 施君, 杨贵岚, 杨晓丽. 子宫螺旋动脉超声联合血清CTRP6、sTWEAK对早发型子痫前期的诊断价值[J]. 天津医药, 2025, 53(5): 514-518. |
| [8] | 冯华, 王魁, 徐文俊, 李能, 张恒喜. 床旁超声造影联合气水交替注射法在重症鼻肠管留置患者中的应用效果[J]. 天津医药, 2025, 53(5): 542-546. |
| [9] | 李娜, 贺英, 滕飞, 贺文姝, 郭彩凤, 钟娜, 吴琼, 李军. 超声BI-RADS分类联合血清FGFR1、GDF3在乳腺肿块良恶性鉴别诊断中的应用价值[J]. 天津医药, 2025, 53(3): 247-251. |
| [10] | 李佳蓉, 朱晓敏, 赵晓赟. 人工智能在气道管理方面的研究进展[J]. 天津医药, 2025, 53(10): 1098-1104. |
| [11] | 徐杨, 袁宇, 高金妹. 超声检查对骨折患者下肢深静脉漂浮血栓脱落的诊断意义[J]. 天津医药, 2024, 52(5): 548-551. |
| [12] | 刘桂莹, 刘立志, 杨宗梅. 胎盘生长因子与晚发型子痫前期患者超声血流参数的关系及对妊娠结局的影响[J]. 天津医药, 2024, 52(10): 1069-1074. |
| [13] | 王众, 赵静雯, 王天驰, 唐缨. 超声影像组学在肾炎组织学分型中的应用价值[J]. 天津医药, 2024, 52(10): 1100-1105. |
| [14] | 王天驰, 王众, 牛宁宁, 唐缨. 超声影像组学对移植肾实质性病变鉴别诊断的价值[J]. 天津医药, 2023, 51(6): 653-657. |
| [15] | 刘伟亮, 陆海永, 郑英娟, 李朝喜, 温德惠. C-TIRADS及超微血管成像技术评估桥本甲状腺炎合并甲状腺结节性质的价值[J]. 天津医药, 2023, 51(5): 535-539. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||