天津医药 ›› 2024, Vol. 52 ›› Issue (9): 917-923.doi: 10.11958/20240171
高攀( ), 谢冰歆, 周赞东, 刘彤△()
), 谢冰歆, 周赞东, 刘彤△()
收稿日期:2024-02-02
修回日期:2024-04-16
出版日期:2024-09-15
发布日期:2024-09-06
通讯作者:
△E-mail:作者简介:高攀(1998),女,硕士在读,主要从事慢性肾脏病和心房颤动相关机制方面研究。E-mail:基金资助:
GAO Pan(), XIE Bingxin, ZHOU Zandong, LIU Tong△()
Received:2024-02-02
Revised:2024-04-16
Published:2024-09-15
Online:2024-09-06
Contact:
△E-mail:高攀, 谢冰歆, 周赞东, 刘彤. 慢性肾脏病循环中FGF23对心房纤维化的促进作用[J]. 天津医药, 2024, 52(9): 917-923.
GAO Pan, XIE Bingxin, ZHOU Zandong, LIU Tong. Promoting effect of circulating FGF23 on atrial fibrosis in chronic kidney disease[J]. Tianjin Medical Journal, 2024, 52(9): 917-923.
摘要:
目的 探究慢性肾脏疾病(CKD)循环中成纤维细胞生长因子(FGF)23通过与心房组织成纤维细胞生长因子受体(FGFR)4结合促进心房纤维化的可能机制。方法 选择健康雄性SD大鼠22只,随机数字表法抽取14只行5/6肾切除手术并且喂养15周建立CKD模型,剩余8只作为假手术(Sham)组。观察2组体质量、血压、肾功能、超声心动图、心外膜电标测以及病理指标。酶联免疫吸附试验测定2组大鼠循环中的FGF23水平,左心房组织转录组测序寻找差异表达基因。大鼠心房成纤维细胞分为对照组、FGFR抑制剂组、转化生长因子-β(TGF-β)组及TGF-β+FGFR抑制剂组,采用Western blot法检测α-平滑肌肌动蛋白(α-SMA)、胶原蛋白Ⅰ(ColⅠ)以及磷酸化蛋白激酶B(p-AKT)蛋白的表达。结果 CKD组大鼠收缩压、肌酐以及血尿素氮水平升高。心脏电生理检查显示CKD可促进心房颤动及房室传导阻滞的发生。心脏超声提示CKD组左心房内径明显增大,病理染色显示CKD组左心房发生明显纤维化,心外膜电标测提示CKD组大鼠左心房电传导速度明显减慢并且传导异质性明显增加。CKD大鼠循环中的FGF23水平明显增加。Western blot检测发现CKD组大鼠FGFR4表达上调。阻断心房成纤维细胞FGF23/FGFR4信号通路后,纤维化相关蛋白α-SMA、ColⅠ及p-AKT/AKT降低。结论 CKD可能通过诱导心房结构重构及电重构促进房颤的发生,循环中增加的FGF23可能通过与心房组织中FGFR4结合启动下游AKT通路,进而促进心房纤维化。
中图分类号:
| 组别 | 体质量/g | Cr/ (μmol/L) | BUN/ (mmol/L) | 收缩压/ mmHg | |||
|---|---|---|---|---|---|---|---|
| SHAM组 | 485.60±38.28 | 23.57±8.18 | 168.09±8.66 | 114.17±4.78 | |||
| CKD组 | 502.80±28.88 | 58.05±13.57 | 245.09±19.83 | 126.17±6.11 | |||
| t | 0.802 | 4.866** | 7.955** | 3.460** | |||
| 组别 | 平均动脉压/ mmHg | 舒张压/ mmHg | 心脏质量/胫骨 长度/(mg/cm) | ||||
| SHAM组 | 100.73±2.31 | 93.94±3.28 | 31.20±4.04 | ||||
| CKD组 | 103.42±8.86 | 93.68±9.86 | 44.41±4.46 | ||||
| t | 0.657 | 0.057 | 4.907** | ||||
表1 2组大鼠的生化指标及基本特征比较(n=5,$\bar{x}±s$)
Tab.1 Comparison of biochemical indicators and baseline characteristics between the two groups of rats
| 组别 | 体质量/g | Cr/ (μmol/L) | BUN/ (mmol/L) | 收缩压/ mmHg | |||
|---|---|---|---|---|---|---|---|
| SHAM组 | 485.60±38.28 | 23.57±8.18 | 168.09±8.66 | 114.17±4.78 | |||
| CKD组 | 502.80±28.88 | 58.05±13.57 | 245.09±19.83 | 126.17±6.11 | |||
| t | 0.802 | 4.866** | 7.955** | 3.460** | |||
| 组别 | 平均动脉压/ mmHg | 舒张压/ mmHg | 心脏质量/胫骨 长度/(mg/cm) | ||||
| SHAM组 | 100.73±2.31 | 93.94±3.28 | 31.20±4.04 | ||||
| CKD组 | 103.42±8.86 | 93.68±9.86 | 44.41±4.46 | ||||
| t | 0.657 | 0.057 | 4.907** | ||||
| 组别 | QT间期/ms | 窦房结恢复时间/ms | 房颤持续时间/s |
|---|---|---|---|
| Sham组 | 41.60±8.29 | 170.00±8.72 | 1.16±2.59 |
| CKD组 | 86.80±10.73 | 206.40±25.63 | 10.02±6.56 |
| t | 7.451** | 3.007* | 2.807* |
表2 2组大鼠电生理学参数比较(n=5,$\bar{x}±s$)
Tab.2 Comparison of electrophysiologic parameters between two groups of rats
| 组别 | QT间期/ms | 窦房结恢复时间/ms | 房颤持续时间/s |
|---|---|---|---|
| Sham组 | 41.60±8.29 | 170.00±8.72 | 1.16±2.59 |
| CKD组 | 86.80±10.73 | 206.40±25.63 | 10.02±6.56 |
| t | 7.451** | 3.007* | 2.807* |
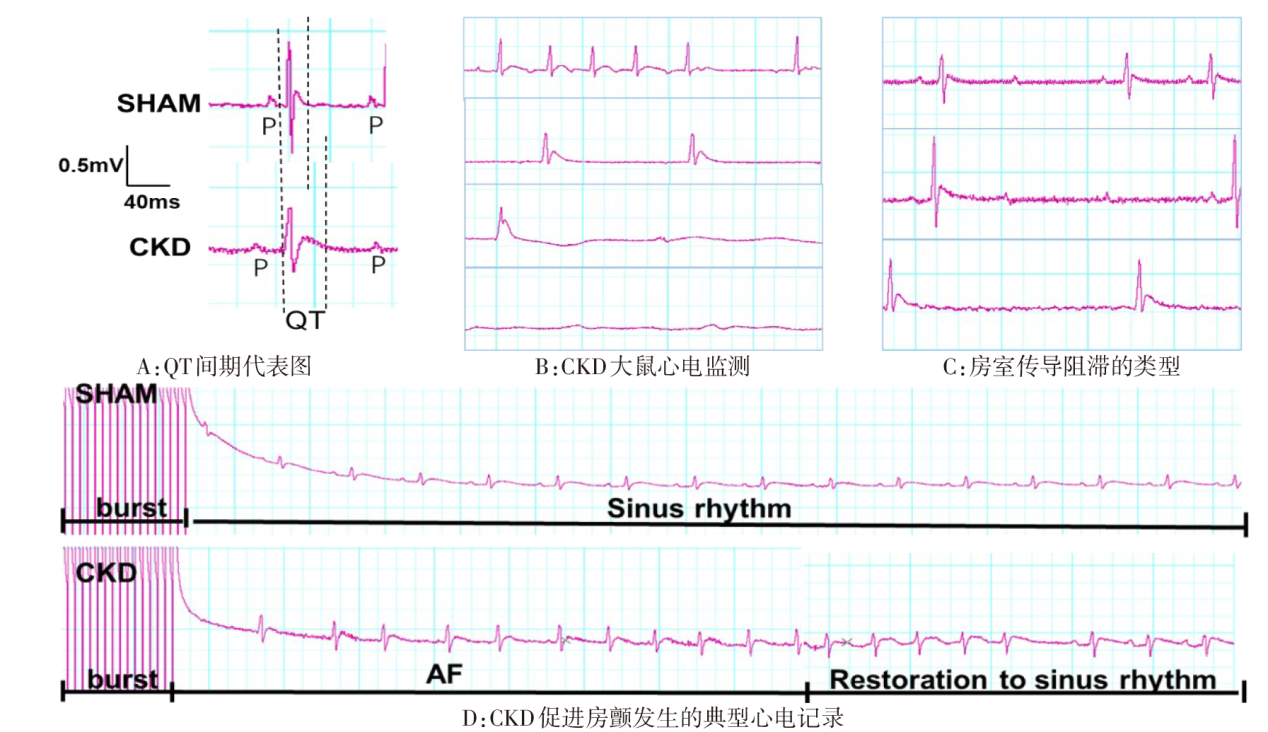
图1 2组大鼠电生理检查心电图
Fig.1 Electrophysiological study of electrocardiograms in two groups of rats
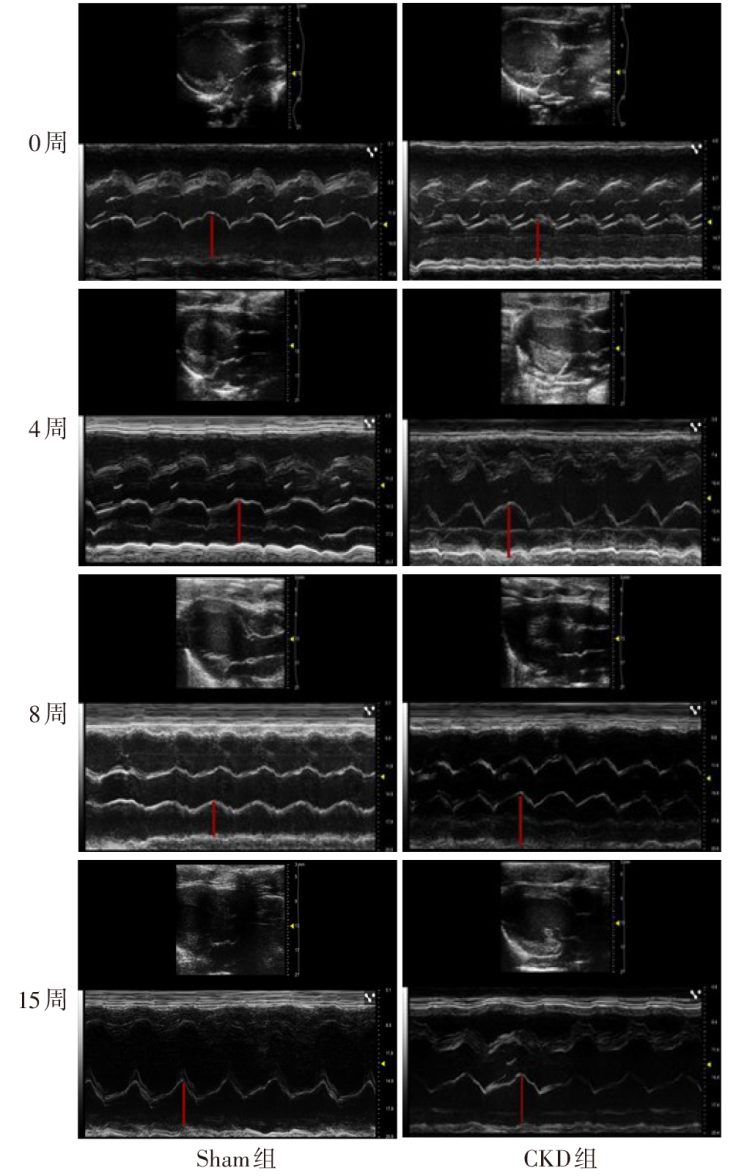
图2 2组大鼠不同时间段LAD变化情况
Fig.2 Changes in LAD at various time intervals in two groups of rats
| 组别 | 0周 | 4周 | 8周 | 15周 |
|---|---|---|---|---|
| SHAM组 | 3.96±0.12 | 3.95±0.36 | 3.96±0.34 | 4.00±0.40 |
| CKD组 | 3.98±0.35 | 4.63±0.16 | 4.67±0.38 | 4.81±0.10 |
| t | 0.131 | 3.909** | 3.128* | 4.381** |
表3 2组大鼠不同时间段LAD比较(n=5,mm,$\bar{x}±s$)
Tab.3 Comparison of LAD in different time periods between two groups of rats
| 组别 | 0周 | 4周 | 8周 | 15周 |
|---|---|---|---|---|
| SHAM组 | 3.96±0.12 | 3.95±0.36 | 3.96±0.34 | 4.00±0.40 |
| CKD组 | 3.98±0.35 | 4.63±0.16 | 4.67±0.38 | 4.81±0.10 |
| t | 0.131 | 3.909** | 3.128* | 4.381** |
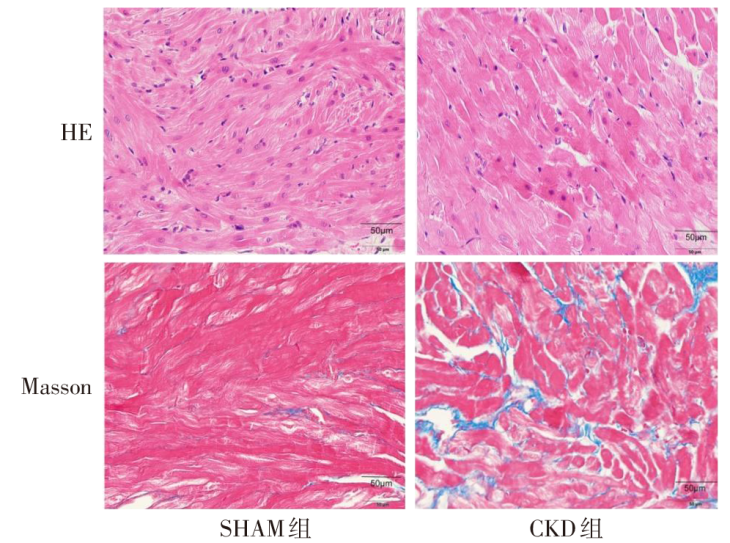
图3 2组大鼠左心房组织病理学变化(HE染色、Masson染色,×400)
Fig.3 Pathological changes in left atrial tissue of rats in both groups (HE staining, Masson staining, ×400)
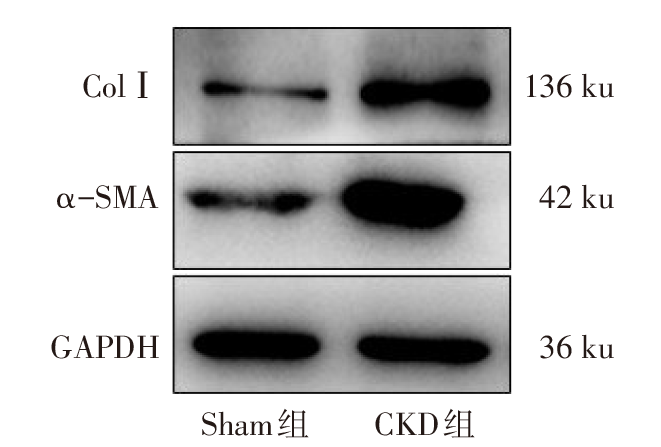
图4 Western blot检测2组大鼠左心房组织中α-SMA、Col Ⅰ蛋白表达
Fig.4 The expression levels of α-SMA and Col Ⅰ protein in left atrium of rats from two groups detected by Western blot assay
| 组别 | 组织胶原容积分数 | α-SMA | ColⅠ | 左心房传导速度/(mm/ms) | 绝对不均一性/(ms/mm) | 不均匀性指数 |
|---|---|---|---|---|---|---|
| Sham组 | 2.29±0.67 | 0.26±0.07 | 0.44±0.26 | 0.82±0.18 | 3.82±1.39 | 1.20±0.45 |
| CKD组 | 5.12±1.20 | 1.14±0.59 | 1.58±0.58 | 0.39±0.09 | 7.16±2.87 | 3.28±1.22 |
| t | 4.634** | 3.322* | 4.020** | 4.780** | 2.343* | 3.578** |
表4 2组大鼠心房结构重构及电重构参数比较(n=5,$\bar{x}±s$)
Tab.4 Comparison of structural remodeling as well as electrical remodeling parameters of atria between two groups of rats
| 组别 | 组织胶原容积分数 | α-SMA | ColⅠ | 左心房传导速度/(mm/ms) | 绝对不均一性/(ms/mm) | 不均匀性指数 |
|---|---|---|---|---|---|---|
| Sham组 | 2.29±0.67 | 0.26±0.07 | 0.44±0.26 | 0.82±0.18 | 3.82±1.39 | 1.20±0.45 |
| CKD组 | 5.12±1.20 | 1.14±0.59 | 1.58±0.58 | 0.39±0.09 | 7.16±2.87 | 3.28±1.22 |
| t | 4.634** | 3.322* | 4.020** | 4.780** | 2.343* | 3.578** |
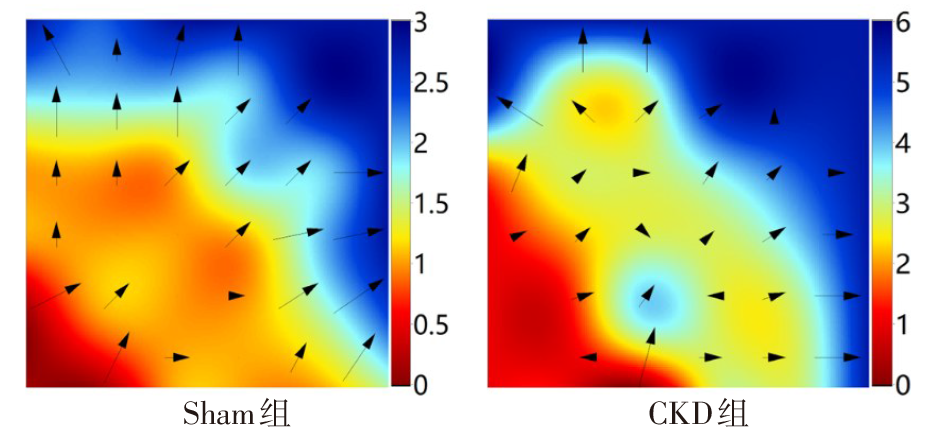
图5 2组大鼠左心房心外膜电标测典型图
Fig.5 Typical diagram of left atrial epicardial electrical markers in two groups
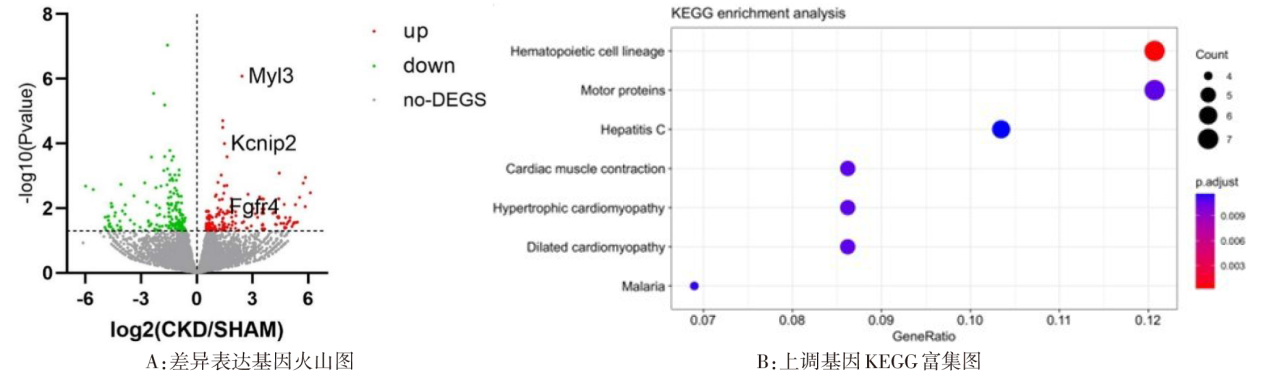
图6 差异表达基因生物信息分析结果
Fig.6 Results of bioinformatic analysis of differentially expressed genes
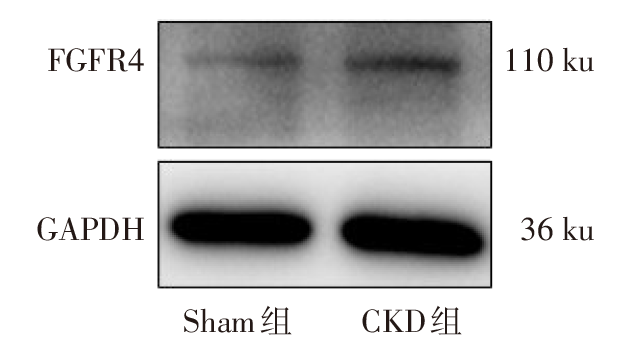
图7 Western blot检测2组大鼠左心房组织中FGFR4蛋白表达
Fig.7 The expression of FGFR4 protein in left atrium of rats from two groups detected by Western blot assay
| 组别 | FGF23/(ng/L) | FGFR4 |
|---|---|---|
| Sham组 | 2 771.53±1 393.28 | 0.30±0.27 |
| CKD组 | 8 452.75±1 377.41 | 0.97±0.37 |
| t | 6.484** | 3.239* |
表5 2组大鼠循环FGF23水平及心房FGFR4蛋白表达比较(n=5,$\bar{x}±s$)
Tab.5 Comparison of circulating FGF23 levels and atrial FGFR4 protein expression between two groups of rats
| 组别 | FGF23/(ng/L) | FGFR4 |
|---|---|---|
| Sham组 | 2 771.53±1 393.28 | 0.30±0.27 |
| CKD组 | 8 452.75±1 377.41 | 0.97±0.37 |
| t | 6.484** | 3.239* |
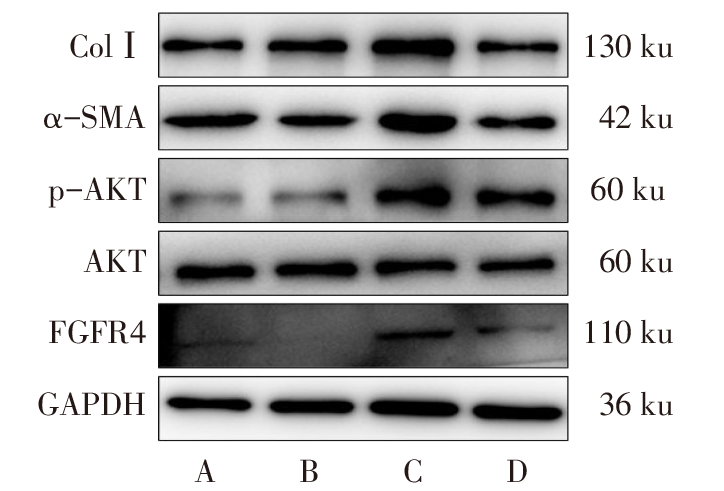
图8 Western blot检测各组细胞中ColⅠ、α-SMA、p-AKT、FGFR4蛋白表达 A:对照组;B:FGFR抑制剂组;C:TGF-β组;D:TGF-β+FGFR抑制剂组。
Fig.8 Western blot analysis of Col I, α-SMA, p-AKT, AKT and FGFR4 protein expression in each cell group
| 组别 | ColⅠ | α-SMA | FGFR4 | p-AKT/AKT |
|---|---|---|---|---|
| 对照组 | 0.46±0.10 | 0.36±0.18 | 0.41±0.08 | 0.79±0.27 |
| FGFR抑制剂组 | 0.44±0.13 | 0.41±0.16 | 0.27±0.20 | 0.60±0.28 |
| TGF-β组 | 0.97±0.11ab | 1.22±0.08ab | 1.19±0.39ab | 2.90±0.94ab |
| TGF-β+FGFR抑制剂组 | 0.58±0.25c | 0.72±0.08c | 0.43±0.16c | 0.34±0.20c |
| F | 22.585** | 37.142** | 12.359** | 20.705** |
表6 4组细胞中α-SMA、ColⅠ、FGFR4、p-AKT的蛋白表达水平比较(n=4,$\bar{x}±s$)
Tab.6 Comparison of protein levels of α-SMA, Col I, FGFR4 and p-AKT between four groups of cells
| 组别 | ColⅠ | α-SMA | FGFR4 | p-AKT/AKT |
|---|---|---|---|---|
| 对照组 | 0.46±0.10 | 0.36±0.18 | 0.41±0.08 | 0.79±0.27 |
| FGFR抑制剂组 | 0.44±0.13 | 0.41±0.16 | 0.27±0.20 | 0.60±0.28 |
| TGF-β组 | 0.97±0.11ab | 1.22±0.08ab | 1.19±0.39ab | 2.90±0.94ab |
| TGF-β+FGFR抑制剂组 | 0.58±0.25c | 0.72±0.08c | 0.43±0.16c | 0.34±0.20c |
| F | 22.585** | 37.142** | 12.359** | 20.705** |
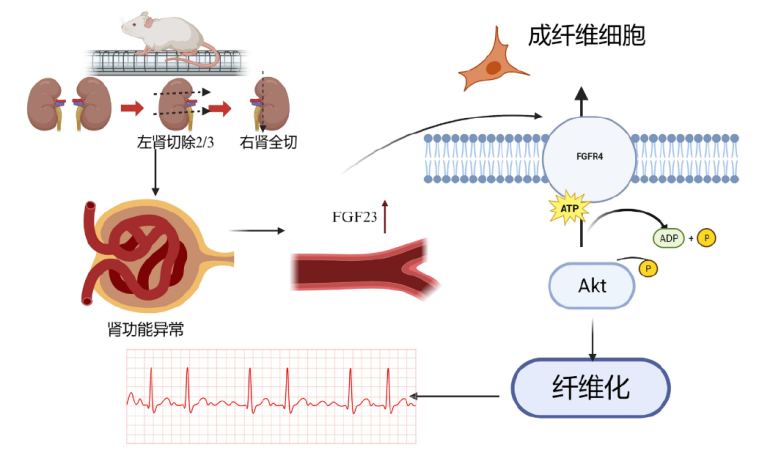
图9 FGF23/FGFR4下游通路图 5/6肾切除所致的肾功能异常会使循环中的FGF23增多,FGF23可与成纤维细胞中的FGFR4受体结合启动下游AKT通路促进纤维化,进而促进房颤的发生。
Fig.9 FGF23/FGFR4 downstream pathway illustration
| [1] | 高翔, 梅长林. 慢性肾脏病早期筛查、诊断及防治指南(2022年版)[J]. 中华肾脏病杂志, 2022, 38(5):453-464. |
| GAO X, MEI C L. Interpretation of guideline for early screening,diagnosis,prevention and treatment of chronic kidney disease(2022 edition)[J]. Chinese Journal of Practical Internal Medicine, 2022, 38(5):453-464. doi:10.19538/j.nk2022090108. | |
| [2] | GREGG L P, HEDAYATI S S. Management of traditional cardiovascular risk factors in CKD:what are the data?[J]. Am J Kidney Dis, 2018, 72(5):728-744. doi:10.1053/j.ajkd.2017.12.007. |
| [3] | BANSAL N, FAN D, HSU C Y, et al. Incident atrial fibrillation and risk of end-stage renal disease in adults with chronic kidney disease[J]. Circulation, 2013, 127(5):569-574. doi:10.1161/CIRCULATIONAHA.112.123992. |
| [4] | LIPPI G, SANCHIS-GOMAR F, CERVELLIN G. Global epidemiology of atrial fibrillation:an increasing epidemic and public health challenge[J]. Int J Stroke, 2021, 16(2):217-221. doi:10.1177/1747493019897870. |
| [5] | SOLIMAN E Z, PRINEAS R J, GO A S, et al. Chronic kidney disease and prevalent atrial fibrillation:the Chronic Renal Insufficiency Cohort (CRIC)[J]. Am Heart J, 2010, 159(6):1102-1107. doi:10.1016/j.ahj.2010.03.027. |
| [6] | GUO Y, GAO J, YE P, et al. Comparison of atrial fibrillation in CKD and non-CKD populations:a cross-sectional analysis from the Kailuan study[J]. Int J Cardiol, 2019, 277:125-129. doi:10.1016/j.ijcard.2018.11.098. |
| [7] | DING W Y, GUPTA D, WONG C F, et al. Pathophysiology of atrial fibrillation and chronic kidney disease[J]. Cardiovasc Res, 2021, 117(4):1046-1059. doi:10.1093/cvr/cvaa258. |
| [8] | JANKOWSKI J, FLOEGE J, FLISER D, et al. Cardiovascular disease in chronic kidney disease:pathophysiological insights and therapeutic options[J]. Circulation, 2021, 143(11):1157-1172. doi:10.1161/CIRCULATIONAHA.120.050686. |
| [9] | KOVESDY C P. Epidemiology of chronic kidney disease: an update 2022[J]. Kidney Int Suppl (2011), 2022, 12(1):7-11. doi:10.1016/j.kisu.2021.11.003. |
| [10] | MATHEW J S, SACHS M C, KATZ R, et al. Fibroblast growth factor-23 and incident atrial fibrillation:the Multi-Ethnic Study of Atherosclerosis (MESA) and the Cardiovascular Health Study (CHS)[J]. Circulation, 2014, 130(4):298-307. doi:10.1161/CIRCULATIONAHA.113.005499. |
| [11] | FAUL C, AMARAL A P, OSKOUEI B, et al. FGF23 induces left ventricular hypertrophy[J]. J Clin Invest, 2011, 121(11):4393-4408. doi:10.1172/JCI46122. |
| [12] | DONG Q, LI S, WANG W, et al. FGF23 regulates atrial fibrosis in atrial fibrillation by mediating the STAT3 and SMAD3 pathways[J]. J Cell Physiol, 2019, 234(11):19502-19510. doi:10.1002/jcp.28548. |
| [13] | YAO C, VELEVA T, SCOTT L J R, et al. Enhanced cardiomyocyte NLRP3 inflammasome signaling promotes atrial fibrillation[J]. Circulation, 2018, 138(20):2227-2242. doi:10.1161/CIRCULATIONAHA.118.035202. |
| [14] | HEALEY J S, BARANCHUK A, CRYSTAL E, et al. Prevention of atrial fibrillation with angiotensin-converting enzyme inhibitors and angiotensin receptor blockers:a Meta-analysis[J]. J Am Coll Cardiol, 2005, 45(11):1832-1839. doi:10.1016/j.jacc.2004.11.070. |
| [15] | LANDRAY M J, WHEELER D C, LIP G Y, et al. Inflammation,endothelial dysfunction,and platelet activation in patients with chronic kidney disease:the chronic renal impairment in Birmingham (CRIB) study[J]. Am J Kidney Dis, 2004, 43(2):244-253. doi:10.1053/j.ajkd.2003.10.037. |
| [16] | SONG J, NAVARRO-GARCIA J A, WU J, et al. Chronic kidney disease promotes atrial fibrillation via inflammasome pathway activation[J]. J Clin Invest, 2023, 133(19):e167517. doi:10.1172/JCI167517. |
| [17] | QIU H, JI C, WU H, et al. Chronic kidney disease-induced atrial structural remodeling and atrial fibrillation: more studies on the pathological mechanism are encouraged[J]. Naunyn Schmiedebergs Arch Pharmacol, 2018, 391(7):671-673. doi:10.1007/s00210-018-1494-4. |
| [18] | AOKI K, TESHIMA Y, KONDO H, et al. Role of indoxyl sulfate as a predisposing factor for atrial fibrillation in renal dysfunction[J]. J Am Heart Assoc, 2015, 4(10):e002023. doi:10.1161/JAHA.115.002023. |
| [19] | HEIJMAN J, VOIGT N, GHEZELBASH S, et al. Calcium handling abnormalities as a target for atrial fibrillation therapeutics:how close to clinical implementation?[J]. J Cardiovasc Pharmacol, 2015, 66(6):515-522. doi:10.1097/FJC.0000000000000253. |
| [20] | CHEN W T, CHEN Y C, HSIEH M H, et al. The uremic toxin indoxyl sulfate increases pulmonary vein and atrial arrhythmogenesis[J]. J Cardiovasc Electrophysiol, 2015, 26(2):203-210. doi:10.1111/jce.12554. |
| [21] | KUGA K, KUSAKARI Y, UESUGI K, et al. Fibrosis growth factor 23 is a promoting factor for cardiac fibrosis in the presence of transforming growth factor-β1[J]. PLoS One, 2020, 15(4):e0231905. doi:10.1371/journal.pone.0231905. |
| [22] | LEIFHEIT-NESTLER M, KIRCHHOFF F, NESPOR J, et al. Fibroblast growth factor 23 is induced by an activated renin-angiotensin-aldosterone system in cardiac myocytes and promotes the pro-fibrotic crosstalk between cardiac myocytes and fibroblasts[J]. Nephrol Dial Transplant, 2018, 33(10):1722-1734. doi:10.1093/ndt/gfy006. |
| [23] | GRABNER A, AMARAL A P, SCHRAMM K, et al. Activation of cardiac fibroblast growth factor receptor 4 causes left ventricular hypertrophy[J]. Cell Metab, 2015, 22(6):1020-1032. doi:10.1016/j.cmet.2015.09.002. |
| [24] | HAN X, CAI C, XIAO Z, et al. FGF23 induced left ventricular hypertrophy mediated by FGFR4 signaling in the myocardium is attenuated by soluble Klotho in mice[J]. J Mol Cell Cardiol, 2020, 138:66-74. doi:10.1016/j.yjmcc.2019.11.149. |
| [25] | SINGH S, GRABNER A, YANUCIL C, et al. Fibroblast growth factor 23 directly targets hepatocytes to promote inflammation in chronic kidney disease[J]. Kidney Int, 2016, 90(5):985-996. doi:10.1016/j.kint.2016.05.019. |
| [1] | 姜天佑, 李敏, 孙碧文, 李越洋, 邢丽静, 田晨. Let-7b诱导白血病相关巨噬细胞复极抑制AML的发展[J]. 天津医药, 2026, 54(3): 225-231. |
| [2] | 黄熷远, 付靖, 赵亚, 王龙灏, 仓顺东. 非小细胞肺癌EGFR-TKI耐药与p53基因突变的研究进展[J]. 天津医药, 2026, 54(3): 333-336. |
| [3] | 刘魁智, 宣学习, 周芃, 袁孝伟, 朱自强. 炙甘草汤调控miR-26b-5p/SMAD4通路对心房颤动大鼠模型心房重构的影响[J]. 天津医药, 2026, 54(1): 14-22. |
| [4] | 李文秀, 朱振宇, 柴慧, 郑晓轩, 卢婧, 李润琴. 心房颤动患者左心耳血栓形成机制的研究进展[J]. 天津医药, 2025, 53(9): 1005-1008. |
| [5] | 陈苗苗, 张亚征, 赵芳, 杨立恒, 焦丽娜, 赵晓赟. 阻塞性睡眠呼吸暂停和心房颤动因果关系的多组学孟德尔随机化分析[J]. 天津医药, 2025, 53(9): 946-951. |
| [6] | 万艳波, 刘明, 王勇. 秦皮甲素调节HMGB1/RAGE信号通路对缺氧/复氧诱导的心肌细胞损伤的影响[J]. 天津医药, 2025, 53(8): 796-801. |
| [7] | 冯学武, 李景娟, 蒯婉君. 高龄非瓣膜性心房颤动患者新型口服抗凝药依从性分析[J]. 天津医药, 2025, 53(8): 884-888. |
| [8] | 贾文歆, 周利娟, 王丽香. 血清CCL21、NLRP3与脑梗死患者机械取栓术后出血转化的相关性研究[J]. 天津医药, 2025, 53(7): 700-703. |
| [9] | 吴素勤, 徐子舒, 许智晶, 吴洁, 王聪梅. 重症颅脑损伤减压术患者血清MMP-10、TLR2水平及其与疾病转归的关系[J]. 天津医药, 2025, 53(7): 704-708. |
| [10] | 吴宾, 杨自更, 金玲, 张婧, 韦红梅, 蔡冰冰, 魏玉英. miRNA-381-3p/MuRF1轴对低氧性肺动脉高压小鼠心肺损伤的影响[J]. 天津医药, 2025, 53(6): 571-577. |
| [11] | 杜凌云, 王耀武, 任楠. 肾透明细胞癌中PRMT2、TRAF2与转移相关基因表达对预后的评估价值[J]. 天津医药, 2025, 53(5): 492-497. |
| [12] | 孙鲁生, 张丽芳, 高俊杰, 汤秀英. CT定量左心结构参数与肥厚型心肌病并心房颤动射频消融术后复发的关系[J]. 天津医药, 2025, 53(5): 533-536. |
| [13] | 邓海娟, 权永娟, 李芳. 妊娠期糖尿病患者血清GPER1、CFH水平与妊娠结局的关系[J]. 天津医药, 2025, 53(4): 369-373. |
| [14] | 郑少阳, 智慧, 王曼, 武冰, 张清格, 李冠阳. 酒精性肝病患者外周血sTim-3、sST2水平与疾病严重程度的相关性[J]. 天津医药, 2025, 53(4): 383-388. |
| [15] | 彭溪, 杨莉莉, 刘敏, 张峻梅. 肺部肺炎克雷伯菌感染患者血清SOCS-1、sTREM-2、ACLY变化及临床意义[J]. 天津医药, 2025, 53(4): 397-401. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||