天津医药 ›› 2022, Vol. 50 ›› Issue (11): 1177-1181.doi: 10.11958/20220912
陈池义( ), 张炜琪, 谢炎, 蒋文涛△()
), 张炜琪, 谢炎, 蒋文涛△()
收稿日期:2022-08-19
出版日期:2022-11-15
发布日期:2022-11-11
通讯作者:
蒋文涛
E-mail:ccy_616@126.com;jiangwentao@nankai.edu.cn
作者简介:陈池义(1987),男,住院医师,主要从事肝脏移植的临床与基础研究。E-mail:基金资助:
CHEN Chiyi(), ZHANG Weiqi, XIE Yan, JIANG Wentao△()
Received:2022-08-19
Published:2022-11-15
Online:2022-11-11
Contact:
JIANG Wentao
E-mail:ccy_616@126.com;jiangwentao@nankai.edu.cn
陈池义, 张炜琪, 谢炎, 蒋文涛. 肿瘤组织Ki67的表达与肝细胞癌肝移植患者预后的关系[J]. 天津医药, 2022, 50(11): 1177-1181.
CHEN Chiyi, ZHANG Weiqi, XIE Yan, JIANG Wentao. Association of the expression of Ki67 with the prognosis of liver transplantation in patients with hepatocellular carcinoma[J]. Tianjin Medical Journal, 2022, 50(11): 1177-1181.
摘要:
目的 探讨肝细胞癌(HCC)组织中Ki67的表达与肝移植(LT)患者预后的关系。方法 收集178例接受原位肝移植治疗的HCC患者的临床资料和免疫组化结果,按照患者肿瘤组织Ki67表达水平的中位数将患者分为Ki67高表达组和低表达组。比较2组患者的临床指标。采用Kaplan-Meier法绘制生存曲线,比较2组患者的预后情况。采用单因素和多因素Cox回归分析影响患者LT术后预后的危险因素。结果 178例研究对象中,Ki67高表达组85例,低表达组93例。Ki67高表达组患者术后1、3、5年总体生存率(78.7%、52.6%、39.5%)与无复发生存率(47.9%、34.7%、32.0%)明显低于Ki67低表达组(86.5%、76.3%、76.3%;84.4%、77.5%、72.4%,Log-rank χ2分别为9.016和28.467,P<0.01)。Cox多因素分析显示Ki67高表达是影响患者术后无复发生存的独立危险因素(HR=3.653,95%CI:1.997~6.683,均P<0.01)。Ki67高表达患者术前血清甲胎蛋白水平、微血管侵犯以及肿瘤低分化的发生率高于低表达组(P<0.05)。结论 HCC组织中Ki67的表达与患者LT术后的预后有关,Ki67可作为预测肝细胞癌肝移植患者预后的一个潜在指标。
中图分类号:

图1 免疫组化检测Ki67在肝癌组织中的表达(×400) A:肝癌组织Ki67高表达;B:肝癌组织Ki67低表达。
Fig.1 The expression of Ki67 in liver cancer tissues detected by immunohistochemistry (×400)
| 组别 | n | 年龄(岁) | AST(U/L) | ALT(U/L) | TB(μmol/L) | ALB(g/L) | WBC(×109/L) | HGB(g/L) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 低表达组 | 93 | 54.60±8.92 | 42.50(29.75,67.35) | 34.30(22.00,52.65) | 26.54(14.35,43.09) | 35.62±6.19 | 4.13(2.94,5.49) | 129.00(104.00,146.50) | ||||||||||||||||
| 高表达组 | 85 | 53.86±9.87 | 51.00(28.70,100.40) | 39.60(23.15,57.30) | 22.59(14.45,63.12) | 35.72±6.03 | 4.62(3.19,6.87) | 130.00(111.00,142.00) | ||||||||||||||||
| t、Z或χ2 | 0.528 | 1.587 | 1.241 | 0.406 | 0.107 | 1.889 | 0.220 | |||||||||||||||||
| 组别 | PLT(×109/L) | INR | PT(s) | MELD评分(分) | AFP(μg/L) | 肿瘤最大直径(cm) | ||||||||||||||||||
| 低表达组 | 85.00(55.00,138.50) | 1.22(1.06,1.34) | 13.70(11.90,15.05) | 8.26(7.06,9.90) | 44.54(6.63,481.10) | 3.00(2.30,5.00) | ||||||||||||||||||
| 高表达组 | 116.00(70.50,155.50) | 1.19(1.09,1.36) | 13.30(12.20,15.30) | 7.85(6.91,9.92) | 133.50(12.60,3 071.00) | 3.50(2.00,7.00) | ||||||||||||||||||
| t、Z或χ2 | 1.871 | 0.039 | 0.016 | 0.221 | 2.337* | 0.390 | ||||||||||||||||||
| 组别 | 性别 | 肿瘤个数 | 卫星灶 | 微血管侵犯 | 肿瘤低分化 | |||||||||||||||||||
| 男 | 女 | 单个 | 多个 | 有 | 无 | 有 | 无 | 是 | 否 | |||||||||||||||
| 低表达组 | 81(87.10) | 12(12.90) | 42(45.16) | 51(54.84) | 14(15.05) | 79(84.95) | 33(35.48) | 60(64.52) | 4(4.30) | 89(95.70) | ||||||||||||||
| 高表达组 | 75(88.24) | 10(11.76) | 33(38.82) | 52(61.18) | 12(14.12) | 73(85.88) | 44(51.76) | 41(48.24) | 22(25.88) | 63(74.12) | ||||||||||||||
| t、Z或χ2 | 0.053 | 0.732 | 0.031 | 4.796* | 16.583** | |||||||||||||||||||
表1 2组患者临床病理资料比较
Tab.1 Comparison of clinicopathological data between the two groups
| 组别 | n | 年龄(岁) | AST(U/L) | ALT(U/L) | TB(μmol/L) | ALB(g/L) | WBC(×109/L) | HGB(g/L) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 低表达组 | 93 | 54.60±8.92 | 42.50(29.75,67.35) | 34.30(22.00,52.65) | 26.54(14.35,43.09) | 35.62±6.19 | 4.13(2.94,5.49) | 129.00(104.00,146.50) | ||||||||||||||||
| 高表达组 | 85 | 53.86±9.87 | 51.00(28.70,100.40) | 39.60(23.15,57.30) | 22.59(14.45,63.12) | 35.72±6.03 | 4.62(3.19,6.87) | 130.00(111.00,142.00) | ||||||||||||||||
| t、Z或χ2 | 0.528 | 1.587 | 1.241 | 0.406 | 0.107 | 1.889 | 0.220 | |||||||||||||||||
| 组别 | PLT(×109/L) | INR | PT(s) | MELD评分(分) | AFP(μg/L) | 肿瘤最大直径(cm) | ||||||||||||||||||
| 低表达组 | 85.00(55.00,138.50) | 1.22(1.06,1.34) | 13.70(11.90,15.05) | 8.26(7.06,9.90) | 44.54(6.63,481.10) | 3.00(2.30,5.00) | ||||||||||||||||||
| 高表达组 | 116.00(70.50,155.50) | 1.19(1.09,1.36) | 13.30(12.20,15.30) | 7.85(6.91,9.92) | 133.50(12.60,3 071.00) | 3.50(2.00,7.00) | ||||||||||||||||||
| t、Z或χ2 | 1.871 | 0.039 | 0.016 | 0.221 | 2.337* | 0.390 | ||||||||||||||||||
| 组别 | 性别 | 肿瘤个数 | 卫星灶 | 微血管侵犯 | 肿瘤低分化 | |||||||||||||||||||
| 男 | 女 | 单个 | 多个 | 有 | 无 | 有 | 无 | 是 | 否 | |||||||||||||||
| 低表达组 | 81(87.10) | 12(12.90) | 42(45.16) | 51(54.84) | 14(15.05) | 79(84.95) | 33(35.48) | 60(64.52) | 4(4.30) | 89(95.70) | ||||||||||||||
| 高表达组 | 75(88.24) | 10(11.76) | 33(38.82) | 52(61.18) | 12(14.12) | 73(85.88) | 44(51.76) | 41(48.24) | 22(25.88) | 63(74.12) | ||||||||||||||
| t、Z或χ2 | 0.053 | 0.732 | 0.031 | 4.796* | 16.583** | |||||||||||||||||||
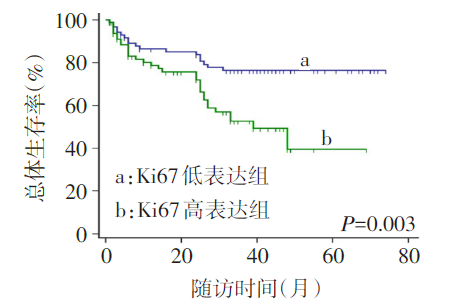
图2 2组患者肝移植术后OS比较
Fig.2 Comparison of overall survival between two groups of patients after liver transplantation
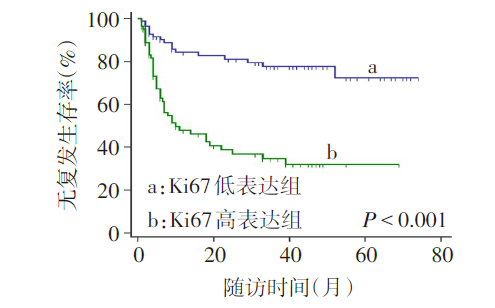
图3 2组患者肝移植术后RFS比较
Fig.3 Comparison of recurrence-free survival between two groups of patients after liver transplantation
| 编号 | 变量名称 | 赋值 |
|---|---|---|
| Y | 患者死亡/肿瘤复发 | 发生=1,未发生=0 |
| X1 | 年龄 | >55岁=1,≤55岁=0 |
| X2 | 性别 | 男=1,女=0 |
| X3 | 肿瘤个数 | 多个=1,单个=0 |
| X4 | 卫星灶 | 有=1,无=0 |
| X5 | 微血管侵犯 | 有=1,无=0 |
| X6 | 肿瘤分化程度 | 低分化=1,非低分化=0 |
| X7 | KLI | >20%=1,≤20%=0 |
| X8 | 术前血清AFP | >400 μg/L=1,≤400 μg/L=0 |
| X9 | 肿瘤最大直径 | >5 cm=1,≤5 cm=0 |
表2 变量赋值情况
Tab.2 Variable assignment
| 编号 | 变量名称 | 赋值 |
|---|---|---|
| Y | 患者死亡/肿瘤复发 | 发生=1,未发生=0 |
| X1 | 年龄 | >55岁=1,≤55岁=0 |
| X2 | 性别 | 男=1,女=0 |
| X3 | 肿瘤个数 | 多个=1,单个=0 |
| X4 | 卫星灶 | 有=1,无=0 |
| X5 | 微血管侵犯 | 有=1,无=0 |
| X6 | 肿瘤分化程度 | 低分化=1,非低分化=0 |
| X7 | KLI | >20%=1,≤20%=0 |
| X8 | 术前血清AFP | >400 μg/L=1,≤400 μg/L=0 |
| X9 | 肿瘤最大直径 | >5 cm=1,≤5 cm=0 |
| 变量 | B | SE | Wald χ2 | P | HR | HR 95%CI |
|---|---|---|---|---|---|---|
| 年龄 | 0.510 | 0.281 | 3.305 | 0.069 | 1.666 | 0.961~2.889 |
| 性别 | -0.222 | 0.361 | 0.379 | 0.538 | 0.801 | 0.394~1.625 |
| 肿瘤个数 | 0.827 | 0.282 | 8.622 | 0.003 | 2.286 | 1.316~3.970 |
| 肿瘤最大直径 | 1.620 | 0.271 | 35.747 | <0.001 | 5.054 | 2.972~8.597 |
| 卫星灶 | 0.911 | 0.298 | 9.323 | 0.002 | 2.486 | 1.386~4.460 |
| 微血管侵犯 | 1.573 | 0.285 | 30.392 | <0.001 | 4.819 | 2.755~8.429 |
| 肿瘤分化程度 | 0.781 | 0.315 | 6.129 | 0.013 | 2.183 | 1.177~4.050 |
| Ki67表达 | 1.412 | 0.289 | 23.811 | <0.001 | 4.103 | 2.327~7.235 |
| 术前血清AFP | 1.435 | 0.262 | 29.904 | <0.001 | 4.199 | 2.511~7.022 |
表3 影响患者术后无复发生存的单因素Cox回归分析
Tab.3 Univariate Cox regression analysis on recurrence-free survival of patients
| 变量 | B | SE | Wald χ2 | P | HR | HR 95%CI |
|---|---|---|---|---|---|---|
| 年龄 | 0.510 | 0.281 | 3.305 | 0.069 | 1.666 | 0.961~2.889 |
| 性别 | -0.222 | 0.361 | 0.379 | 0.538 | 0.801 | 0.394~1.625 |
| 肿瘤个数 | 0.827 | 0.282 | 8.622 | 0.003 | 2.286 | 1.316~3.970 |
| 肿瘤最大直径 | 1.620 | 0.271 | 35.747 | <0.001 | 5.054 | 2.972~8.597 |
| 卫星灶 | 0.911 | 0.298 | 9.323 | 0.002 | 2.486 | 1.386~4.460 |
| 微血管侵犯 | 1.573 | 0.285 | 30.392 | <0.001 | 4.819 | 2.755~8.429 |
| 肿瘤分化程度 | 0.781 | 0.315 | 6.129 | 0.013 | 2.183 | 1.177~4.050 |
| Ki67表达 | 1.412 | 0.289 | 23.811 | <0.001 | 4.103 | 2.327~7.235 |
| 术前血清AFP | 1.435 | 0.262 | 29.904 | <0.001 | 4.199 | 2.511~7.022 |
| 变量 | B | SE | Wald χ2 | P | HR | HR 95%CI |
|---|---|---|---|---|---|---|
| 年龄 | -0.289 | 0.283 | 1.041 | 0.307 | 0.749 | 0.430~1.305 |
| 性别 | -0.080 | 0.408 | 0.038 | 0.845 | 0.923 | 0.415~2.055 |
| 肿瘤个数 | 0.894 | 0.323 | 7.666 | 0.006 | 2.444 | 1.298~4.600 |
| 肿瘤最大直径 | 1.206 | 0.288 | 17.511 | <0.001 | 3.341 | 1.899~5.878 |
| 微血管侵犯 | 1.419 | 0.317 | 20.068 | <0.001 | 4.132 | 2.221~7.687 |
| 肿瘤分化程度 | 0.930 | 0.324 | 8.221 | 0.004 | 2.535 | 1.342~4.789 |
| Ki67表达 | 0.857 | 0.297 | 8.333 | 0.004 | 2.355 | 1.317~4.213 |
| 术前血清AFP | 1.265 | 0.290 | 19.003 | <0.001 | 3.543 | 2.006~6.257 |
表4 影响患者术后生存的单因素Cox回归分析
Tab.4 Univariate Cox regression analysis on overall survival of patients
| 变量 | B | SE | Wald χ2 | P | HR | HR 95%CI |
|---|---|---|---|---|---|---|
| 年龄 | -0.289 | 0.283 | 1.041 | 0.307 | 0.749 | 0.430~1.305 |
| 性别 | -0.080 | 0.408 | 0.038 | 0.845 | 0.923 | 0.415~2.055 |
| 肿瘤个数 | 0.894 | 0.323 | 7.666 | 0.006 | 2.444 | 1.298~4.600 |
| 肿瘤最大直径 | 1.206 | 0.288 | 17.511 | <0.001 | 3.341 | 1.899~5.878 |
| 微血管侵犯 | 1.419 | 0.317 | 20.068 | <0.001 | 4.132 | 2.221~7.687 |
| 肿瘤分化程度 | 0.930 | 0.324 | 8.221 | 0.004 | 2.535 | 1.342~4.789 |
| Ki67表达 | 0.857 | 0.297 | 8.333 | 0.004 | 2.355 | 1.317~4.213 |
| 术前血清AFP | 1.265 | 0.290 | 19.003 | <0.001 | 3.543 | 2.006~6.257 |
| 变量 | B | SE | Wald χ2 | P | HR | HR 95%CI |
|---|---|---|---|---|---|---|
| 肿瘤最大直径 | 0.945 | 0.309 | 9.344 | 0.002 | 2.572 | 1.404~4.714 |
| 微血管侵犯 | 0.905 | 0.319 | 8.055 | 0.005 | 2.472 | 1.323~4.618 |
| Ki67表达 | 1.295 | 0.308 | 17.669 | <0.001 | 3.653 | 1.997~6.683 |
| 术前血清AFP | 0.781 | 0.294 | 7.864 | 0.008 | 2.184 | 1.226~3.888 |
表5 影响患者术后无复发生存的多因素Cox回归分析
Tab.5 Multivariate Cox regression analysis on recurrence-free survival of patients
| 变量 | B | SE | Wald χ2 | P | HR | HR 95%CI |
|---|---|---|---|---|---|---|
| 肿瘤最大直径 | 0.945 | 0.309 | 9.344 | 0.002 | 2.572 | 1.404~4.714 |
| 微血管侵犯 | 0.905 | 0.319 | 8.055 | 0.005 | 2.472 | 1.323~4.618 |
| Ki67表达 | 1.295 | 0.308 | 17.669 | <0.001 | 3.653 | 1.997~6.683 |
| 术前血清AFP | 0.781 | 0.294 | 7.864 | 0.008 | 2.184 | 1.226~3.888 |
| 变量 | B | SE | Wald χ2 | P | HR | HR 95%CI |
|---|---|---|---|---|---|---|
| 微血管侵犯 | 0.827 | 0.352 | 5.525 | 0.019 | 2.287 | 1.147~4.558 |
| 术前血清AFP | 0.667 | 0.328 | 4.127 | 0.042 | 1.948 | 1.024~3.705 |
表6 影响患者术后生存的多因素Cox回归分析
Tab.6 Multivariate Cox regression analysis on overall survival of patients
| 变量 | B | SE | Wald χ2 | P | HR | HR 95%CI |
|---|---|---|---|---|---|---|
| 微血管侵犯 | 0.827 | 0.352 | 5.525 | 0.019 | 2.287 | 1.147~4.558 |
| 术前血清AFP | 0.667 | 0.328 | 4.127 | 0.042 | 1.948 | 1.024~3.705 |
| [1] | BRAY F, FERLAY J, SOERJOMATARAM I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6):394-424. doi:10.3322/caac.21492. |
| [2] | XU X, LU D, LING Q, et al. Liver transplantation for hepatocellular carcinoma beyond the Milan criteria[J]. Gut, 2016, 65(6):1035-1041. doi:10.1136/gutjnl-2014-308513. |
| [3] | MAZZAFERRO V, CITTERIO D, BHOORI S, et al. Liver transplantation in hepatocellular carcinoma after tumour downstaging(XXL):a randomised, controlled,phase 2b/3 trial[J]. Lancet Oncol, 2020,21(7):947-956. doi:10.1016/S1470-2045(20)30224-2. |
| [4] | MA E, LI J, XING H, et al. Development of a predictive nomogram for early recurrence of hepatocellular carcinoma in patients undergoing liver transplantation[J]. Ann Transl Med, 2021, 9(6):468. doi:10.21037/atm-21-334. |
| [5] | YAO F Y, XIAO L, BASS N M, et al. Liver transplantation for hepatocellular carcinoma: validation of the UCSF-expanded criteria based on preoperative imaging[J]. Am J Transplant, 2007, 7(11):2587-2596. doi:10.1111/j.1600-6143.2007.01965.x. |
| [6] | JIANG P, JIA M, HU J, et al. Prognostic value of Ki67 in patients with stage 1-2 endometrial cancer:Validation of the cut-off value of Ki67 as a predictive factor[J]. Onco Targets Ther, 2020, 13:10841-10850. doi:10.2147/OTT.S274420. |
| [7] | CSERNI G, VÖRÖS A, LIEPNIECE-KARELE I, et al. Distribution pattern of the Ki67 labelling index in breast cancer and its implications for choosing cut-off values[J]. Breast, 2014, 23(3):259-263. doi:10.1016/j.breast.2014.02.003. |
| [8] | CAO Y, KE R, WANG S, et al. DNA topoisomerase IIα and Ki67 are prognostic factors in patients with hepatocellular carcinoma[J]. Oncol Lett, 2017, 13(6):4109-4116. doi:10.3892/ol.2017.5999. |
| [9] | GÜLSEREN V, KOCAER M, ÖZDEMIR İA, et al. Do estrogen, progesterone, P53 and Ki67 receptor ratios determined from curettage materials in endometrioid-type endometrial carcinoma predict lymph node metastasis?[J]. Curr Probl Cancer, 2020, 44(1):100498. doi:10.1016/j.currproblcancer.2019.07.003. |
| [10] | SCHOLZEN T, GERDES J. The Ki-67 protein:from the known and the unknown[J]. J Cell Physiol, 2000, 182(3):311-322. doi:10.1002/(SICI)1097-4652(200003)182:3<311::AID-JCP1>3.0.CO;2-9. |
| [11] | WILKINS A C, GUSTERSON B, SZIJGYARTO Z, et al. Ki67 is an independent predictor of recurrence in the largest randomized trial of 3 radiation fractionation schedules in localized prostate cancer[J]. Int J Radiat Oncol Biol Phys, 2018, 101(2):309-315. doi:10.1016/j.ijrobp.2018.01.072. |
| [12] | GRANT L, BANERJI S, MURPHY L, et al. Androgen receptor and Ki67 expression and survival outcomes in non-small cell lung cancer[J]. Horm Cancer, 2018, 9(4):288-294. doi:10.1007/s12672-018-0336-7. |
| [13] | JACOBSEN F, KOHSAR J, GEBAUER F, et al. Loss of p16 and high Ki67 labeling index is associated with poor outcome in esophageal carcinoma[J]. Oncotarget, 2020, 11(12):1007-1016. doi:10.18632/oncotarget.27507. |
| [14] | TEMRAZ S, SHAMSEDDINE A, MUKHERJI D, et al. Ki67 and P53 in relation to disease progression in metastatic pancreatic cancer:A single institution analysis[J]. Pathol Oncol Res, 2019, 25(3):1059-1066. doi:10.1007/s12253-018-0464-y. |
| [15] | THOTAKURA M, TIRUMALASETTI N, KRISHNA R. Role of Ki-67 labeling index as an adjunct to the histopathological diagnosis and grading of astrocytomas[J]. J Cancer Res Ther, 2014, 10(3):641-645. doi:10.4103/0973-1482.139154. |
| [16] | GENÇ C G, FALCONI M, PARTELLI S, et al. Recurrence of pancreatic neuroendocrine tumors and survival predicted by Ki67[J]. Ann Surg Oncol, 2018, 25(8):2467-2474. doi:10.1245/s10434-018-6518-2. |
| [17] | PETRY C, POLI J, DE AZEVEDO DOSSIN I, et al. Evaluation of the potential of the Ki67 index to predict tumor evolution in patients with pituitary adenoma[J]. Int J Clin Exp Pathol, 2019, 12(1):320-326. |
| [18] | ZHANG X, WU Z, PENG Y, et al. Correlationship between Ki67,VEGF,and p53 and hepatocellular carcinoma recurrence in liver transplant patients[J]. Biomed Res Int, 2021, 2021:6651397. doi:10.1155/2021/6651397. |
| [19] | 贾磊, 李豪, 白鸿太, 等. CD34和Ki67的表达预测肝癌术后复发的风险[J]. 肝脏, 2020, 25(2):197-199. |
| JIA L, LI H, BAI H T, et al. The expression of CD34 and Ki67 predicts the risk of postoperative recurrence of hepatocellular carcinoma[J]. Chinese Hepatology, 2020, 25(2):197-199. doi:10.3969/j.issn.1008-1704.2020.02.034. | |
| [20] | 郭飞宇, 杨军, 熊书名, 等. 耐药基因蛋白和Ki67在原发性肝癌中的表达及其在预后中的价值[J]. 中华肝脏外科手术学电子杂志, 2018, 7(1):77-81. |
| GUO F Y, YANG J, XIONG S M, et al. Expressions of drug resistance gene proteins and Ki67 in primary liver cancer and their value in prognosis[J]. Chin J Hepat Surg(Electronic Edition), 2018, 7(1):77-81. doi:10.3877/cma.j.issn.2095-3232.2018.01.019. | |
| [21] | 张彦, 陆伟. Ki67在HBV相关肝细胞癌病理组织中的表达及其临床意义[J]. 天津医药, 2015, 43(8):929-931. |
| ZHANG Y, LU W. Expression of Ki67 and its clinic significance in HBV related hepatocellular carcinoma[J]. Tianjin Med J, 2015, 43(8):929-931. doi:10.11958/j.issn.0253-9896.2015.08.027. | |
| [22] | 韩帅, 孟帆, 张宏凯, 等. Ki67、Ck19与肝细胞癌临床病理特征和磁共振成像表观扩散系数的相关性分析[J]. 中华医学杂志, 2021, 101(11):798-802. |
| HAN S, MENG F, ZHANG H K, et al. Correlation analysis of Ki67,Ck19 with clinicopathological features and apparent diffusion coefficient value of hepatocellular carcinoma[J]. Natl Med J China, 2021, 101(11):798-802. doi:10.3760/cma.j.cn112137-20210108-00058. | |
| [23] | LUO Y, REN F, LIU Y, et al. Clinicopathological and prognostic significance of high Ki-67 labeling index in hepatocellular carcinoma patients:a meta-analysis[J]. Int J Clin Exp Med, 2015, 8(7):10235-10247. |
| [24] | GOLDHIRSCH A, WINER E P, COATES A S, et al. Personalizing the treatment of women with early breast cancer:highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013[J]. Ann Oncol, 2013, 24(9):2206-2223. doi:10.1093/annonc/mdt303. |
| [1] | 张润春, 李树华, 王玉珍, 王巧文. 肺炎支原体肺炎患儿血清LXA4和KLF5表达的临床意义[J]. 天津医药, 2026, 54(3): 269-274. |
| [2] | 朱海燕, 王烨, 尹艳. 老年NSCLC患者术后胃肠功能紊乱的危险因素研究[J]. 天津医药, 2026, 54(3): 289-294. |
| [3] | 刘晓华, 韩婷婷, 高玉杰. 增强CT淋巴结边缘特征联合IPI对难治性弥漫大B细胞巴瘤的预测价值[J]. 天津医药, 2026, 54(3): 303-308. |
| [4] | 黄熷远, 付靖, 赵亚, 王龙灏, 仓顺东. 非小细胞肺癌EGFR-TKI耐药与p53基因突变的研究进展[J]. 天津医药, 2026, 54(3): 333-336. |
| [5] | 王喆, 邱林, 马贲. 番茄来源胞外囊泡样颗粒对口腔鳞状细胞癌的作用效果研究[J]. 天津医药, 2026, 54(2): 145-150. |
| [6] | 余优佳, 秦夏. 外周灌注指数联合血浆容量对感染性休克患者预后的评估价值[J]. 天津医药, 2026, 54(2): 169-172. |
| [7] | 周乔枝, 武红娟, 王科程. 慢性心力衰竭患者血浆海蟾蜍毒素、Ⅰ型胶原α1链表达水平及其与预后的相关性[J]. 天津医药, 2026, 54(2): 184-188. |
| [8] | 黄慧琦, 伍秋苑, 张昆, 李佩贤, 熊亚明, 叶国麟, 周丹. 川楝素联合奥拉帕尼在三阴性乳腺癌中的抗肿瘤机制研究[J]. 天津医药, 2025, 53(9): 897-902. |
| [9] | 周鹏鹏, 丁烁, 姚卫康, 罗祎. 原发性肝癌患者术前免疫因素及与病理特征的关系[J]. 天津医药, 2025, 53(9): 952-956. |
| [10] | 高正杰, 孟涛, 张俏, 陈炳合, 侯栋, 朱绍辉. 术前CALLY指数对根治性胃切除术患者短期预后的预测价值[J]. 天津医药, 2025, 53(9): 967-971. |
| [11] | 杨桃, 全艳, 张加孟, 谢清耘, 黄麟洲. 甲状腺结节细针穿刺细胞学联合BRAF基因检测在甲状腺良恶性肿瘤鉴别诊断中的应用价值[J]. 天津医药, 2025, 53(9): 972-975. |
| [12] | 蒋苏, 李东霞, 吕新翔, 崔艳红, 吕李婷. 基于PI3K/Akt/NF-κB信号通路探讨黄连素对特应性皮炎大鼠皮肤病理变化的治疗作用[J]. 天津医药, 2025, 53(7): 679-683. |
| [13] | 金吴娟, 倪刚, 黄欣宇, 王羊洋. 老年消化道出血患者不良预后的列线图预测模型的构建与验证[J]. 天津医药, 2025, 53(7): 694-699. |
| [14] | 吴素勤, 徐子舒, 许智晶, 吴洁, 王聪梅. 重症颅脑损伤减压术患者血清MMP-10、TLR2水平及其与疾病转归的关系[J]. 天津医药, 2025, 53(7): 704-708. |
| [15] | 曹振振, 叶睿, 刘佳瑶, 孟彤, 孙荣, 徐菱遥. 血清Hsp90α联合β2-MG检测在结直肠癌早期诊断和预后评估中的应用价值[J]. 天津医药, 2025, 53(7): 756-760. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||