天津医药 ›› 2024, Vol. 52 ›› Issue (2): 182-187.doi: 10.11958/20230235
江洪洋( ), 樊世文, 刘铁龙, 谢丽萍△()
), 樊世文, 刘铁龙, 谢丽萍△()
收稿日期:2023-02-27
修回日期:2023-04-03
出版日期:2024-02-15
发布日期:2024-01-26
通讯作者:
△ E-mail:作者简介:江洪洋(1992),男,硕士在读,主要从事临床麻醉应用研究。E-mail:
JIANG Hongyang(), FAN Shiwen, LIU Tielong, XIE Liping△()
Received:2023-02-27
Revised:2023-04-03
Published:2024-02-15
Online:2024-01-26
Contact:
△ E-mail: 江洪洋, 樊世文, 刘铁龙, 谢丽萍. 个体化PEEP联合定期肺复张对行腹腔镜结直肠癌根治术老年患者术后肺不张的影响[J]. 天津医药, 2024, 52(2): 182-187.
JIANG Hongyang, FAN Shiwen, LIU Tielong, XIE Liping. Effect of individualized PEEP combined with regular lung recruitment maneuvers on atelectasis after laparoscopic radical resection of colorectal cancer in elderly patients[J]. Tianjin Medical Journal, 2024, 52(2): 182-187.
摘要:
目的 评估肺超声下驱动压(ΔP)引导的个体化呼气末正压通气(PEEP)联合定期肺复张对Trendelenburg体位下行腹腔镜结直肠癌根治术的老年患者术后肺不张的影响。方法 纳入年龄65~85岁、美国麻醉医师协会分级Ⅰ—Ⅲ级,拟行腹腔镜下结直肠癌根治术的患者62例并分为试验组和对照组(各31例)。2组均在气腹开始后进行第1次肺复张,随后立即以最低ΔP滴定个体化PEEP,气腹结束后进行第2次肺复张。试验组自气腹开始每30 min额外进行一次肺复张,对照组则不干预。以麻醉诱导前(T0)、气腹后30 min(T1)、气腹后90 min(T2)、手术结束时(T3)、进入麻醉复苏室(PACU)45 min后(T4)为观察记录时间点。记录T0、T3和T4时肺超声评分(LUS);T1—T3时肺动态顺应性(Cdyn);T0—T4时间点氧合指数(OI)、平均动脉压(MAP)、心率(HR);记录肺复张期间低血压、PACU中低氧饱和事件以及术后7 d内肺部并发症(POPC)发生率。结果 与对照组相比,试验组在T3和T4时LUS下降(P<0.05),T2、T3时OI和Cdyn升高(P<0.05)。试验组在PACU中低氧饱和事件发生率较对照组下降(P<0.05)。2组患者肺复张期间低血压发生率和术后7 d内POPC发生率差异无统计学意义(P>0.05)。结论 个体化PEEP联合定期肺复张可有效减少老年患者腹腔镜结直肠癌根治术后即刻和PACU中的肺不张。
中图分类号:
| 组别 | n | 年龄/岁 | 性别(男/女) | BMI/(kg/m2) | 吸烟史 |
|---|---|---|---|---|---|
| 对照组 | 31 | 72(67,76) | 20/11 | 23.7±2.7 | 15/14/2 |
| 试验组 | 31 | 74(70,79) | 15/16 | 23.5±2.4 | 19/11/1 |
| Z、χ2或t | 1.637 | 1.640 | 0.345 | 1.243 |
表1 2组患者年龄、性别、BMI、吸烟史比较
Tab.1 Comparison of age, gender, BMI and smoking history between the two groups
| 组别 | n | 年龄/岁 | 性别(男/女) | BMI/(kg/m2) | 吸烟史 |
|---|---|---|---|---|---|
| 对照组 | 31 | 72(67,76) | 20/11 | 23.7±2.7 | 15/14/2 |
| 试验组 | 31 | 74(70,79) | 15/16 | 23.5±2.4 | 19/11/1 |
| Z、χ2或t | 1.637 | 1.640 | 0.345 | 1.243 |
| 组别 | n | 高血压 | 糖尿病 | FEV1/FVC | Hb/(g/L) | ASA分级(Ⅰ/Ⅱ/Ⅲ) | ARISCAT评分(26~44/>44) |
|---|---|---|---|---|---|---|---|
| 对照组 | 31 | 13(41.9) | 4(12.9) | 74.9±7.9 | 120.8±14.4 | 4/24/3 | 8/23 |
| 试验组 | 31 | 16(51.6) | 7(22.6) | 77.6±8.0 | 117.5±12.9 | 3/23/5 | 11/20 |
| Z、χ2或t | 0.583 | 0.995 | 1.316 | 0.939 | 0.728 | 0.683 |
表2 2组患者术前一般资料比较
Tab.2 Comparison of preoperative general data between the two groups
| 组别 | n | 高血压 | 糖尿病 | FEV1/FVC | Hb/(g/L) | ASA分级(Ⅰ/Ⅱ/Ⅲ) | ARISCAT评分(26~44/>44) |
|---|---|---|---|---|---|---|---|
| 对照组 | 31 | 13(41.9) | 4(12.9) | 74.9±7.9 | 120.8±14.4 | 4/24/3 | 8/23 |
| 试验组 | 31 | 16(51.6) | 7(22.6) | 77.6±8.0 | 117.5±12.9 | 3/23/5 | 11/20 |
| Z、χ2或t | 0.583 | 0.995 | 1.316 | 0.939 | 0.728 | 0.683 |
| 组别 | n | PEEP/ cmH2O | 气腹时间/ min | 手术时间/ min | 苏醒时间/ min | 手术类型 (直肠癌/结肠癌) | 输液量/ mL | 估计失血量/ mL | 尿量/ mL |
|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 31 | 9(8,10) | 162(137,185) | 201(183,221) | 13.9±3.5 | 16/15 | 2 000(1 600,2 300) | 150(100,150) | 350(200,550) |
| 试验组 | 31 | 9(7,10) | 180(145,209) | 211(180,238) | 13.4±3.5 | 13/18 | 2 000(1 500,2 500) | 150(100,200) | 420(200,620) |
| Z、χ2或t | 0.857 | 1.352 | 0.514 | 0.647 | 0.583 | 0.542 | 0.670 | 0.789 |
表3 2组患者术中一般资料比较
Tab.3 Comparison of intraoperative data between the two groups
| 组别 | n | PEEP/ cmH2O | 气腹时间/ min | 手术时间/ min | 苏醒时间/ min | 手术类型 (直肠癌/结肠癌) | 输液量/ mL | 估计失血量/ mL | 尿量/ mL |
|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 31 | 9(8,10) | 162(137,185) | 201(183,221) | 13.9±3.5 | 16/15 | 2 000(1 600,2 300) | 150(100,150) | 350(200,550) |
| 试验组 | 31 | 9(7,10) | 180(145,209) | 211(180,238) | 13.4±3.5 | 13/18 | 2 000(1 500,2 500) | 150(100,200) | 420(200,620) |
| Z、χ2或t | 0.857 | 1.352 | 0.514 | 0.647 | 0.583 | 0.542 | 0.670 | 0.789 |
| 组别 | n | T0 | T3 | T4 |
|---|---|---|---|---|
| 对照组 | 31 | 0(0,2) | 10(8,10) | 9(8,11) |
| 试验组 | 31 | 1(0,2) | 8(6,9) | 6(5,8) |
| Z | 0.238 | 3.481** | 3.962** |
表4 2组患者不同时间点LUS比较 [分,M(P25, P75 )]
Tab.4 Comparison of LUS at different time points between the two groups
| 组别 | n | T0 | T3 | T4 |
|---|---|---|---|---|
| 对照组 | 31 | 0(0,2) | 10(8,10) | 9(8,11) |
| 试验组 | 31 | 1(0,2) | 8(6,9) | 6(5,8) |
| Z | 0.238 | 3.481** | 3.962** |
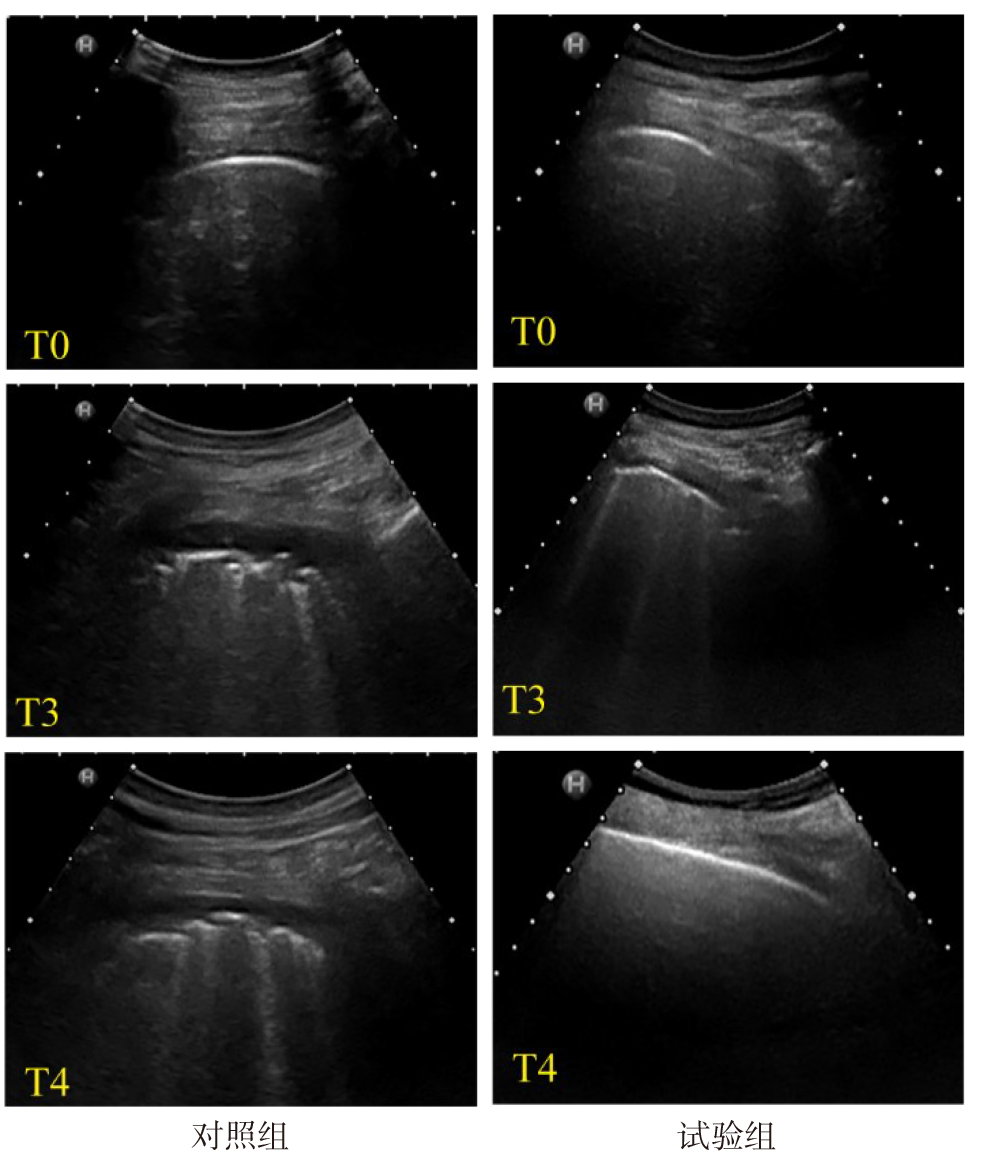
图1 2组不同时点肺后上区的肺超声图像 T0时2组均可见正常的胸膜线(0分);T3时,对照组可见不规则的胸膜线,由多个小的实变分隔(2分),试验组可见规则的胸膜线及多条未合并的B线(1分);T4时,对照组可见不规则的胸膜线,由多个小的实变分隔(2分),试验组中可见正常的胸膜线(0分)。
Fig.1 Lung ultrasound images of the posterior superior region of lung at different time points in the two groups
| 组别 | T1 | T2 | T3 |
|---|---|---|---|
| 对照组 | 24.9±3.9 | 22.4±3.3 | 35.5±7.7 |
| 试验组 | 24.1±3.6 | 24.2±3.8 | 39.7±6.7 |
| t | 0.894 | 2.033* | 2.273* |
表5 2组患者术中Cdyn比较 (n=31,mL/cmH2O,$\bar{x}±s$)
Tab.5 Comparison of intraoperative Cdyn between the two groups
| 组别 | T1 | T2 | T3 |
|---|---|---|---|
| 对照组 | 24.9±3.9 | 22.4±3.3 | 35.5±7.7 |
| 试验组 | 24.1±3.6 | 24.2±3.8 | 39.7±6.7 |
| t | 0.894 | 2.033* | 2.273* |
| 组别 | T0 | T1 | |||
|---|---|---|---|---|---|
| 对照组 | 338.1±20.1 | 390.1±87.0 | |||
| 试验组 | 343.4±26.2 | 373.7±84.7 | |||
| t | 0.889 | 0.752 | |||
| 组别 | T2 | T3 | T4 | ||
| 对照组 | 392.5±64.1 | 398.8±54.0 | 329.1±22.4 | ||
| 试验组 | 435.9±69.3 | 462.6±57.5 | 338.9±30.3 | ||
| t | 2.560* | 4.508** | 1.444 | ||
表6 2组患者OI比较 (n=31,mmHg,$\bar{x}±s$)
Tab.6 Comparison of OI between the two groups
| 组别 | T0 | T1 | |||
|---|---|---|---|---|---|
| 对照组 | 338.1±20.1 | 390.1±87.0 | |||
| 试验组 | 343.4±26.2 | 373.7±84.7 | |||
| t | 0.889 | 0.752 | |||
| 组别 | T2 | T3 | T4 | ||
| 对照组 | 392.5±64.1 | 398.8±54.0 | 329.1±22.4 | ||
| 试验组 | 435.9±69.3 | 462.6±57.5 | 338.9±30.3 | ||
| t | 2.560* | 4.508** | 1.444 | ||
| 组别 | MAP/mmHg | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T4 | ||||||
| 对照组 | 90.1±9.1 | 85.8±9.7 | 87.1±8.8 | 89.6±7.8 | 91.2±9.2 | |||||
| 试验组 | 89.2±10.1 | 81.8±6.9 | 85.1±7.7 | 88.4±10.0 | 90.3±8.4 | |||||
| 组别 | HR/(次/min) | |||||||||
| T0 | T1 | T2 | T3 | T4 | ||||||
| 对照组 | 74.1±8.3 | 71.7±7.1 | 69.5±8.1 | 72.9±8.9 | 76.6±8.8 | |||||
| 试验组 | 77.0±10.6 | 72.1±10.0 | 69.2±9.2 | 74.0±8.8 | 79.2±10.5 | |||||
表7 2组患者MAP和HR的比较 (n=31,$\bar{x}±s$)
Tab.7 Comparison of MAP and HR between the two groups
| 组别 | MAP/mmHg | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T4 | ||||||
| 对照组 | 90.1±9.1 | 85.8±9.7 | 87.1±8.8 | 89.6±7.8 | 91.2±9.2 | |||||
| 试验组 | 89.2±10.1 | 81.8±6.9 | 85.1±7.7 | 88.4±10.0 | 90.3±8.4 | |||||
| 组别 | HR/(次/min) | |||||||||
| T0 | T1 | T2 | T3 | T4 | ||||||
| 对照组 | 74.1±8.3 | 71.7±7.1 | 69.5±8.1 | 72.9±8.9 | 76.6±8.8 | |||||
| 试验组 | 77.0±10.6 | 72.1±10.0 | 69.2±9.2 | 74.0±8.8 | 79.2±10.5 | |||||
| 组别 | n | 肺复张期间 低血压 | 术中血管活性药 总体使用 | PACU中低氧 饱和事件 |
|---|---|---|---|---|
| 对照组 | 31 | 2(6.5) | 17(54.8) | 10(32.3) |
| 试验组 | 31 | 6(19.4) | 20(64.5) | 3(9.7) |
| χ2 | 1.292 | 0.603 | 4.769* |
表8 2组患者肺复张期间低血压、术中血管活性药总体使用情况、PACU中低氧饱和事件发生率比较 [例(%)]
Tab.8 Comparison of the incidence of hypotension during RM, the overall use of vasoactive drugs during operation and the incidence of hypoxia saturation events in PACU between the two groups
| 组别 | n | 肺复张期间 低血压 | 术中血管活性药 总体使用 | PACU中低氧 饱和事件 |
|---|---|---|---|---|
| 对照组 | 31 | 2(6.5) | 17(54.8) | 10(32.3) |
| 试验组 | 31 | 6(19.4) | 20(64.5) | 3(9.7) |
| χ2 | 1.292 | 0.603 | 4.769* |
| 组别 | 咳嗽并咳痰 | 术后低氧血症 | 肺炎 | 肺不张 | 胸腔积液 |
|---|---|---|---|---|---|
| 对照组 | 10(32.3) | 2(6.5) | 1(3.2) | 4(12.9) | 5(16.1) |
| 试验组 | 13(41.9) | 0 | 0 | 2(6.5) | 2(6.5) |
| χ2或P | 0.622 | 0.517 | 0.999▲ | 0.185 | 0.644 |
表9 2组患者术后7 d内POPC比较 [n=31,例(%)]
Tab.9 Comparison of POPC within 7 days after surgery between the two groups
| 组别 | 咳嗽并咳痰 | 术后低氧血症 | 肺炎 | 肺不张 | 胸腔积液 |
|---|---|---|---|---|---|
| 对照组 | 10(32.3) | 2(6.5) | 1(3.2) | 4(12.9) | 5(16.1) |
| 试验组 | 13(41.9) | 0 | 0 | 2(6.5) | 2(6.5) |
| χ2或P | 0.622 | 0.517 | 0.999▲ | 0.185 | 0.644 |
| [1] | ZENG C, LAGIER D, LEE J W, et al. Perioperative pulmonary atelectasis:Part I. biology and mechanisms[J]. Anesthesiology(Philadelphia), 2022, 136(1):181. doi:10.1097/ALN.0000000000003943. |
| [2] | SHONO A, KATAYAMA N, FUJIHARA T, et al. Positive end-expiratory pressure and distribution of ventilation in pneumoperitoneum combined with steep trendelenburg position[J]. Anesthesiology, 2020, 132(3):476-490. doi:10.1097/ALN.0000000000003062. |
| [3] | LAGIER D, ZENG C, FERNANDEZ-BUSTAMANTE A, et al. Perioperative pulmonary atelectasis:Part II. clinical implications[J]. Anesthesiology, 2022, 136(1):206-236. doi:10.1097/ALN.0000000000004009. |
| [4] | FERNANDEZ-BUSTAMANTE A, FRENDL G, SPRUNG J, et al. Postoperative pulmonary complications,early mortality,and hospital stay following noncardiothoracic surgery:a multicenter study by the perioperative research network investigators[J]. JAMA Surg, 2017, 152(2):157-166. doi:10.1001/jamasurg.2016.4065. |
| [5] | 中华医学会麻醉学分会“围术期肺保护性通气策略临床应用专家共识”工作小组. 围术期肺保护性通气策略临床应用专家共识[J]. 中华麻醉学杂志, 2020, 40(5):513-519. |
| Chinese society of anesthesiology task force on clinical application of perioperative lung-protective ventilation strategies. Expert consensus on clinical application of perioperative lung-protective ventilation strategies[J]. Chin J Anesthesiol, 2020, 40(5):513-519. doi:10.3760/cma.j.cn131073.20200402.00501. | |
| [6] | YOUNG C C, HARRIS E M, VACCHIANO C, et al. Lung-protective ventilation for the surgical patient:International expert panel-based consensus recommendations[J]. Br J Anaesth, 2019, 123(6):898-913. doi:10.1016/j.bja.2019.08.017. |
| [7] | ZHOU L, LI H, LI M, et al. Individualized positive end-expiratory pressure guided by respiratory mechanics during anesthesia for the prevention of postoperative pulmonary complications:a systematic review and meta-analysis[J]. J Clin Monit Comput, 2023, 37(2):365-377. doi:10.1007/s10877-022-00960-9. |
| [8] | MONASTESSE A, GIRARD F, MASSICOTTE N, et al. Lung ultrasonography for the assessment of perioperative atelectasis:a pilot feasibility study[J]. Anesth Analg, 2017, 124(2):494-504. doi:10.1213/ANE.0000000000001603. |
| [9] | MINI G, RAY B R, ANAND R K, et al. Effect of driving pressure-guided positive end-expiratory pressure (PEEP) titration on postoperative lung atelectasis in adult patients undergoing elective major abdominal surgery:a randomized controlled trial[J]. Surgery, 2021, 170(1):277-283. doi:10.1016/j.surg.2021.01.047. |
| [10] | ÖSTBERG E, THORISSON A, ENLUND M, et al. Positive end-expiratory pressure alone minimizes atelectasis formation in nonabdominal surgery:a randomized controlled trial[J]. Anesthesiology, 2018, 128(6):1117-1124. doi:10.1097/ALN.0000000000002134. |
| [11] | UKERE A, MARZ A, WODACK K H, et al. Perioperative assessment of regional ventilation during changing body positions and ventilation conditions by electrical impedance tomography[J]. Br J Anaesth, 2016, 117(2):228-235. doi:10.1093/bja/aew188. |
| [12] | O'GARA B, TALMOR D. Perioperative lung protective ventilation[J]. BMJ, 2018, 362:k3030. doi:10.1136/bmj.k3030. |
| [13] | GÉNÉREUX V, CHASSÉ M, GIRARD F, et al. Effects of positive end-expiratory pressure/recruitment manoeuvres compared with zero end-expiratory pressure on atelectasis during open gynaecological surgery as assessed by ultrasonography:a randomised controlled trial[J]. Br J Anaesth, 2020, 124(1):101-109. doi:10.1016/j.bja.2019.09.040. |
| [14] | FRASSANITO L, SONNINO C, PITONI S, et al. Lung ultrasound to monitor the development of pulmonary atelectasis in gynecologic oncologic surgery[J]. Minerva Anestesiol, 2020, 86(12):1287-1295. doi:10.23736/S0375-9393.20.14687-X. |
| [15] | 刘彬彬, 温晓晖, 唐小芳, 等. 全麻人工气腹下老年患者肺不张发生的特点及其与膈肌抑制程度的关系[J]. 中华麻醉学杂志, 2021, 41(6):670-673. |
| LIU B B, WEN X H, TANG X F, et al. Characteristics of atelectasis and its relationship with degree of diaphragm inhibition in elderly patients with artificial pneumoperitoneum under general anesthesia[J]. Chin J Anesthesiol, 2021, 41(6):670-673. doi:10.3760/cma.j.cn131073.20201221.00608. | |
| [16] | JO Y Y, LEE K C, CHANG Y J, et al. Effects of an alveolar recruitment maneuver during lung protective ventilation on postoperative pulmonary complications in elderly patients undergoing laparoscopy[J]. Clin Interv Aging, 2020, 15:1461-1469. doi:10.2147/CIA.S264987. |
| [17] | GARCÍA-FERNÁNDEZ J, ROMERO A, BLANCO A, et al. Recruitment manoeuvres in anaesthesia:How many more excuses are there not to use them?[J]. Rev Esp Anestesiol Reanim (Engl Ed), 2018, 65(4):209-217. doi:10.1016/j.redar.2017.12.006. |
| [18] | WEI K, MIN S, CAO J, et al. Repeated alveolar recruitment maneuvers with and without positive end-expiratory pressure during bariatric surgery:a randomized trial[J]. Minerva Anestesiol, 2018, 84(4):463-472. doi:10.23736/S0375-9393.17.11897-3. |
| [19] | JUNG K, KIM S, KIM B J, et al. Comparison of positive end-expiratory pressure versus tidal volume-induced ventilator-driven alveolar recruitment maneuver in robotic prostatectomy:a randomized controlled study[J]. J Clin Med, 2021, 10(17):3921. doi:10.3390/jcm10173921. |
| [20] | SEVERAC M, CHIALI W, SEVERAC F, et al. Alveolar recruitment manoeuvre results in improved pulmonary function in obese patients undergoing bariatric surgery:a randomised trial[J]. Anaesth Crit Care Pain Med, 2021, 40(3):100775. doi:10.1016/j.accpm.2020.09.011. |
| [21] | ACOSTA C M, SARA T, CARPINELLA M, et al. Lung recruitment prevents collapse during laparoscopy in children:a randomised controlled trial[J]. Eur J Anaesthesiol, 2018, 35(8):573-580. doi:10.1097/EJA.0000000000000761. |
| [22] | COSTA L A, HAJJAR L A, VOLPE M S, et al. Effect of intensive vs moderate alveolar recruitment strategies added to lung-protective ventilation on postoperative pulmonary complications:a randomized clinical trial[J]. JAMA, 2017, 317(14):1422-1432. doi:10.1001/jama.2017.2297. |
| [23] | CUI Y, CAO R, LI G, et al. The effect of lung recruitment maneuvers on post-operative pulmonary complications for patients undergoing general anesthesia:a meta-analysis[J]. PLoS One, 2019, 14(5):e217405. doi:10.1371/journal.pone.0217405. |
| [1] | 赵丽, 马秀丽, 刘毅, 朱毅. 全麻下腹腔镜胃癌根治术后谵妄发生的危险因素分析[J]. 天津医药, 2026, 54(3): 259-264. |
| [2] | 李佳, 赵墨菊, 杨惠茹, 高丽峰, 高月, 李侃, 郭素娜, 沈建军. 超声引导下2种神经阻滞方法在腹腔镜全子宫切除术中麻醉效果与安全性比较[J]. 天津医药, 2026, 54(3): 264-268. |
| [3] | 朱海燕, 王烨, 尹艳. 老年NSCLC患者术后胃肠功能紊乱的危险因素研究[J]. 天津医药, 2026, 54(3): 289-294. |
| [4] | 冯学武, 李景娟, 蒯婉君. 高龄非瓣膜性心房颤动患者新型口服抗凝药依从性分析[J]. 天津医药, 2025, 53(8): 884-888. |
| [5] | 金吴娟, 倪刚, 黄欣宇, 王羊洋. 老年消化道出血患者不良预后的列线图预测模型的构建与验证[J]. 天津医药, 2025, 53(7): 694-699. |
| [6] | 李婉婷, 刘弘扬, 桑婧, 阮育凤, 徐丽, 李冬梅. 老年下肢骨折患者术后发生急性心脑血管意外的影响因素分析[J]. 天津医药, 2025, 53(6): 648-653. |
| [7] | 刘颖, 葛东建, 朱炫姿, 向雯, 耿明悦, 程伟. 经皮耳迷走神经刺激对妇科腹腔镜手术患者术后胃肠功能恢复的影响[J]. 天津医药, 2025, 53(2): 189-193. |
| [8] | 张易, 俞荷花, 徐天鹏. 老年重症急性胰腺炎患者继发凝血功能障碍影响因素分析及预测模型建立[J]. 天津医药, 2025, 53(11): 1180-1185. |
| [9] | 万方鑫, 刘宾, 张皓程, 张昌文, 李宝玉. 腹腔镜疝囊高位结扎联合IPOM与局麻李金斯坦修补术治疗男性全膀胱切除术后腹股沟疝[J]. 天津医药, 2025, 53(10): 1033-1036. |
| [10] | 廖洪柳, 胡艳, 李艳, 邓才望. 血清CRP、SAA、PCT联合脑脊液LDH、ADA水平测定在老年中枢神经系统感染中的应用[J]. 天津医药, 2025, 53(10): 1048-1052. |
| [11] | 张训功, 杨光辉, 杜增利, 薛培, 马梓昆. 铁死亡与老年骨折患者术后认知功能障碍的相关性[J]. 天津医药, 2025, 53(1): 47-51. |
| [12] | 吴亚蒙, 李亮亮, 王彦刚, 邢德福. 血清APOC1和Klotho表达对肾癌后腹腔镜下肾部分切除术患者预后的预测价值[J]. 天津医药, 2025, 53(1): 61-64. |
| [13] | 张新桥, 李幸, 张慧芹, 陈海婷, 刘明远. 老年糖尿病性白内障患者血清Spexin和Pannexin1表达水平及临床意义[J]. 天津医药, 2025, 53(1): 80-84. |
| [14] | 张锡友, 郭一丹, 张春霞, 周晓玲, 贾萌, 石志华, 罗洋. 老年维持性血液透析患者高钾血症与不良预后事件相关性的临床研究[J]. 天津医药, 2024, 52(8): 840-844. |
| [15] | 徐斌, 诸赟, 陈浩, 朱红俊, 高枫, 夏丛奕, 钟玲, 苏伟. 超滤治疗老年心力衰竭合并衰弱患者的有效性及安全性[J]. 天津医药, 2024, 52(7): 743-747. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||