天津医药 ›› 2026, Vol. 54 ›› Issue (6): 612-617.doi: 10.11958/20253576
焦宇兵( ), 雷晓娟, 郭武华△()
), 雷晓娟, 郭武华△()
收稿日期:2025-12-11
修回日期:2026-03-16
出版日期:2026-06-15
发布日期:2026-06-15
通讯作者:
△E-mail:guowuhua@aliyun.com
作者简介:焦宇兵(1989),男,主治医师,主要从事肝脏疾病的介入微创治疗方面研究。E-mail:基金资助:
JIAO Yubing(), LEI Xiaojuan, GUO Wuhua△()
Received:2025-12-11
Revised:2026-03-16
Published:2026-06-15
Online:2026-06-15
Contact:
△E-mail:guowuhua@aliyun.com
焦宇兵, 雷晓娟, 郭武华. 自发性门体分流对乙型肝炎肝硬化失代偿期患者预后的影响及预测模型构建[J]. 天津医药, 2026, 54(6): 612-617.
JIAO Yubing, LEI Xiaojuan, GUO Wuhua. Impact and prediction model construction of spontaneous portosystemic shunts on the prognosis of patients with hepatitis B virus-related decompensated cirrhosis[J]. Tianjin Medical Journal, 2026, 54(6): 612-617.
摘要:
目的 探讨自发性门体分流(SPSS)对乙型肝炎肝硬化失代偿期(HBV-DC)患者预后的影响,基于SPSS分流道总横截面积(TSA)构建预后列线图模型并评估其预测价值。方法 根据腹部CT测量的TSA将641例HBV-DC患者分为无SPSS组169例、小型SPSS组(TSA<83 mm2)343例和大型SPSS组(TSA≥83 mm2)129例。比较3组一般资料、肝硬化并发症及预后,应用Cox比例风险模型筛选HBV-DC患者死亡的独立危险因素,构建列线图模型并进行验证,采用受试者工作特征(ROC)曲线及曲线下面积(AUC)比较该模型与传统预后模型的预测价值。结果 与无SPSS组比较,小型SPSS组和大型SPSS组血红蛋白(Hb)、血小板计数(PLT)水平降低,国际标准化比值(INR)、血肌酐水平升高,门静脉血栓和食管胃静脉曲张破裂出血(EGVB)发生率升高(P<0.05);与小型SPSS组比较,大型SPSS组PLT水平、中-大量腹水发生率降低,INR、终末期肝病模型(MELD)评分升高,门静脉血栓和肝性脑病发生率升高(P<0.05)。无SPSS组、小型SPSS组和大型SPSS组累积总生存率呈依次下降趋势(P<0.05)。多因素Cox回归分析显示,高龄、Hb降低,总胆红素(TBil)、INR、TSA增加,有大量腹水和肝性脑病是患者死亡的独立危险因素(P<0.05);据此构建的列线图模型C指数为0.711(95%CI:0.639~0.783),校准曲线显示模型具有较好的校准能力,决策曲线分析显示模型具有良好的正向净收益。6、12及24个月ROC曲线分析结果显示,列线图模型的预测价值均优于Child-Turcotte-Pugh(CTP)评分、MELD评分及白蛋白-胆红素(ALBI)评分(P<0.05)。结论 TSA增加是HBV-DC患者死亡的独立危险因素,建立的预测模型对评估患者预后有较好的价值。
中图分类号:
| 组别 | n | 性别(男/女) | 年龄/岁 | WBC/(×109/L) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 无SPSS组 | 169 | 128/41 | 53.80±11.63 | 4.69(3.44,5.98) | ||||||||||||
| 小型SPSS组 | 343 | 259/84 | 55.45±12.52 | 4.19(3.14,6.05) | ||||||||||||
| 大型SPSS组 | 129 | 100/29 | 54.12±12.38 | 3.93(2.54,5.80)a | ||||||||||||
| χ2、F或H | 0.214 | 1.227 | 7.420* | |||||||||||||
| 组别 | Hb/(g/L) | PLT/(×109/L) | ALB/(g/L) | |||||||||||||
| 无SPSS组 | 122(109,137) | 101(69,133) | 31(26,35) | |||||||||||||
| 小型SPSS组 | 108(90,123)a | 77(57,107)a | 30(26,34) | |||||||||||||
| 大型SPSS组 | 102(86,117)a | 62(38,87)ab | 29(26,33)a | |||||||||||||
| H | 52.854** | 55.309** | 7.174* | |||||||||||||
| 组别 | TBil/(μmol/L) | INR | SCr/(μmol/L) | |||||||||||||
| 无SPSS组 | 37.2(22.2,99.8) | 1.25(1.09,1.51) | 66(56,76) | |||||||||||||
| 小型SPSS组 | 36.3(20.1,72.3) | 1.30(1.17,1.54)a | 69(57,84)a | |||||||||||||
| 大型SPSS组 | 45.8(27.5,77.0) | 1.48(1.26,1.76)ab | 69(59,86)a | |||||||||||||
| H | 5.475 | 30.022** | 6.612* | |||||||||||||
| 组别 | CTP评分/分 | MELD评分/分 | ALBI评分/分 | |||||||||||||
| 无SPSS组 | 9(7,10) | 12(9,17) | -1.51(-1.98,-1.08) | |||||||||||||
| 小型SPSS组 | 9(8,11) | 13(10,17) | -1.42(-1.93,-1.05) | |||||||||||||
| 大型SPSS组 | 9(8,11)a | 15(12,18)ab | -1.37(-1.65,-1.00) | |||||||||||||
| H | 6.979* | 14.594** | 5.979 | |||||||||||||
表1 3组一般资料比较
Tab.1 Comparison of general characteristics between the three groups
| 组别 | n | 性别(男/女) | 年龄/岁 | WBC/(×109/L) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 无SPSS组 | 169 | 128/41 | 53.80±11.63 | 4.69(3.44,5.98) | ||||||||||||
| 小型SPSS组 | 343 | 259/84 | 55.45±12.52 | 4.19(3.14,6.05) | ||||||||||||
| 大型SPSS组 | 129 | 100/29 | 54.12±12.38 | 3.93(2.54,5.80)a | ||||||||||||
| χ2、F或H | 0.214 | 1.227 | 7.420* | |||||||||||||
| 组别 | Hb/(g/L) | PLT/(×109/L) | ALB/(g/L) | |||||||||||||
| 无SPSS组 | 122(109,137) | 101(69,133) | 31(26,35) | |||||||||||||
| 小型SPSS组 | 108(90,123)a | 77(57,107)a | 30(26,34) | |||||||||||||
| 大型SPSS组 | 102(86,117)a | 62(38,87)ab | 29(26,33)a | |||||||||||||
| H | 52.854** | 55.309** | 7.174* | |||||||||||||
| 组别 | TBil/(μmol/L) | INR | SCr/(μmol/L) | |||||||||||||
| 无SPSS组 | 37.2(22.2,99.8) | 1.25(1.09,1.51) | 66(56,76) | |||||||||||||
| 小型SPSS组 | 36.3(20.1,72.3) | 1.30(1.17,1.54)a | 69(57,84)a | |||||||||||||
| 大型SPSS组 | 45.8(27.5,77.0) | 1.48(1.26,1.76)ab | 69(59,86)a | |||||||||||||
| H | 5.475 | 30.022** | 6.612* | |||||||||||||
| 组别 | CTP评分/分 | MELD评分/分 | ALBI评分/分 | |||||||||||||
| 无SPSS组 | 9(7,10) | 12(9,17) | -1.51(-1.98,-1.08) | |||||||||||||
| 小型SPSS组 | 9(8,11) | 13(10,17) | -1.42(-1.93,-1.05) | |||||||||||||
| 大型SPSS组 | 9(8,11)a | 15(12,18)ab | -1.37(-1.65,-1.00) | |||||||||||||
| H | 6.979* | 14.594** | 5.979 | |||||||||||||
| 组别 | n | 腹水分级 (无-少/中/大量) | 门静脉 血栓 | 肝性 脑病 | EGVB |
|---|---|---|---|---|---|
| 无SPSS组 | 169 | 68/76/25 | 2(1.18) | 15(8.88) | 7(4.14) |
| 小型SPSS组 | 343 | 96/169/78a | 26(7.58)a | 39(11.37) | 45(13.12)a |
| 大型SPSS组 | 129 | 52/55/22b | 22(17.05)ab | 32(24.81)ab | 25(19.38)a |
| χ2 | 12.346* | 25.672** | 18.642** | 16.927** |
表2 3组患者肝硬化并发症比较
Tab.2 Comparison of cirrhosis-related complications between the three groups
| 组别 | n | 腹水分级 (无-少/中/大量) | 门静脉 血栓 | 肝性 脑病 | EGVB |
|---|---|---|---|---|---|
| 无SPSS组 | 169 | 68/76/25 | 2(1.18) | 15(8.88) | 7(4.14) |
| 小型SPSS组 | 343 | 96/169/78a | 26(7.58)a | 39(11.37) | 45(13.12)a |
| 大型SPSS组 | 129 | 52/55/22b | 22(17.05)ab | 32(24.81)ab | 25(19.38)a |
| χ2 | 12.346* | 25.672** | 18.642** | 16.927** |
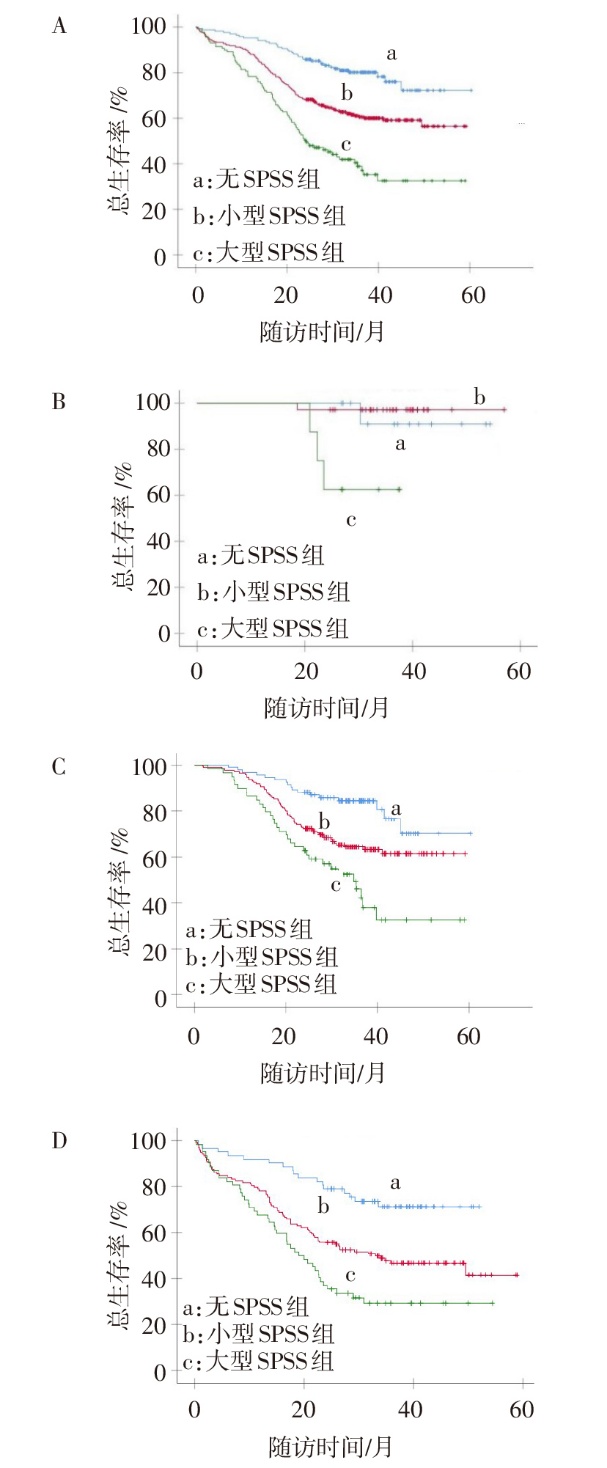
图1 SPSS不同分组的HBV-DC患者总体及不同CTP分级下的总生存率比较 A:各组累积总生存率,Log-rank χ2 =54.585,P<0.001;B—D:CTP分级A、B、C级中3组累积总生存率,Log-rank χ2分别为11.504、23.125、23.209,P<0.05。
Fig.1 Comparison of overall survival rates between HBV-DC patients in different SPSS groups and under different CTP grades
| 变量 | β | SE | Wald χ2 | P | HR(95%CI) |
|---|---|---|---|---|---|
| 性别 | -0.246 | 0.143 | -1.718 | 0.086 | 0.782(0.590~1.035) |
| 年龄 | 0.013 | 0.005 | 2.421 | 0.015 | 1.013(1.002~1.024) |
| WBC | 0.034 | 0.019 | 1.847 | 0.065 | 1.035(0.998~1.074) |
| Hb | -0.013 | 0.002 | -5.217 | <0.001 | 0.987(0.982~0.992) |
| PLT | -0.002 | 0.001 | -1.922 | 0.055 | 0.998(0.995~1.000) |
| ALB | -0.060 | 0.012 | -5.118 | <0.001 | 0.941(0.920~0.963) |
| TBil | 0.002 | 0.001 | 3.995 | <0.001 | 1.002(1.001~1.003) |
| INR | 0.649 | 0.098 | 6.627 | <0.001 | 1.914(1.579~2.319) |
| SCr | 0.003 | 0.002 | 2.121 | 0.034 | 1.003(1.001~1.006) |
| TSA | 0.002 | 0.001 | 6.676 | <0.001 | 1.003(1.002 ~1.004) |
| 腹水分级 | 10.524 | 0.005 | |||
| 中量 | 0.265 | 0.152 | 1.740 | 0.082 | 1.303(0.967~1.755) |
| 大量 | 0.573 | 0.178 | 3.216 | 0.001 | 1.773(1.251~2.513) |
| 肝性脑病 | 0.885 | 0.156 | 5.661 | <0.001 | 2.424(1.784~3.293) |
| 门静脉血栓 | 0.158 | 0.223 | 0.706 | 0.480 | 1.171(0.756~1.814) |
| EGVB | 0.009 | 0.198 | 0.047 | 0.962 | 1.009(0.685~1.487) |
表3 影响患者总生存期的单因素Cox回归分析
Tab.3 Univariate Cox regression analysis for overall survival of patients
| 变量 | β | SE | Wald χ2 | P | HR(95%CI) |
|---|---|---|---|---|---|
| 性别 | -0.246 | 0.143 | -1.718 | 0.086 | 0.782(0.590~1.035) |
| 年龄 | 0.013 | 0.005 | 2.421 | 0.015 | 1.013(1.002~1.024) |
| WBC | 0.034 | 0.019 | 1.847 | 0.065 | 1.035(0.998~1.074) |
| Hb | -0.013 | 0.002 | -5.217 | <0.001 | 0.987(0.982~0.992) |
| PLT | -0.002 | 0.001 | -1.922 | 0.055 | 0.998(0.995~1.000) |
| ALB | -0.060 | 0.012 | -5.118 | <0.001 | 0.941(0.920~0.963) |
| TBil | 0.002 | 0.001 | 3.995 | <0.001 | 1.002(1.001~1.003) |
| INR | 0.649 | 0.098 | 6.627 | <0.001 | 1.914(1.579~2.319) |
| SCr | 0.003 | 0.002 | 2.121 | 0.034 | 1.003(1.001~1.006) |
| TSA | 0.002 | 0.001 | 6.676 | <0.001 | 1.003(1.002 ~1.004) |
| 腹水分级 | 10.524 | 0.005 | |||
| 中量 | 0.265 | 0.152 | 1.740 | 0.082 | 1.303(0.967~1.755) |
| 大量 | 0.573 | 0.178 | 3.216 | 0.001 | 1.773(1.251~2.513) |
| 肝性脑病 | 0.885 | 0.156 | 5.661 | <0.001 | 2.424(1.784~3.293) |
| 门静脉血栓 | 0.158 | 0.223 | 0.706 | 0.480 | 1.171(0.756~1.814) |
| EGVB | 0.009 | 0.198 | 0.047 | 0.962 | 1.009(0.685~1.487) |
| 变量 | β | SE | Wald χ2 | P | HR(95%CI) | |
|---|---|---|---|---|---|---|
| 年龄 | 0.019 | 0.006 | 3.418 | <0.001 | 1.020(1.008~1.031) | |
| Hb | -0.009 | 0.003 | -3.508 | <0.001 | 0.991(0.985~0.996) | |
| ALB | -0.024 | 0.013 | -1.812 | 0.070 | 0.977(0.952~1.002) | |
| TBil | 0.001 | 0.001 | 2.062 | 0.039 | 1.002(1.001~1.003) | |
| INR | 0.370 | 0.149 | 2.477 | 0.013 | 1.453(1.080~1.953) | |
| SCr | -0.001 | 0.002 | -0.352 | 0.719 | 0.999(0.996~1.003) | |
| TSA | 0.002 | 0.001 | 4.816 | <0.001 | 1.002(1.001 ~1.003) | |
| 腹水分级 | 4.724 | 0.094 | ||||
| 中量 | 0.249 | 0.160 | 1.556 | 0.123 | 1.281(0.936~1.530) | |
| 大量 | 0.486 | 0.192 | 2.527 | 0.012 | 1.622(1.111~2.369) | |
| 肝性脑病 | 0.568 | 0.188 | 3.023 | 0.003 | 1.756(1.207~2.554) | |
表4 影响患者总生存期的多因素Cox回归分析
Tab.4 Multivariate Cox regression analysis for overall survival of patients
| 变量 | β | SE | Wald χ2 | P | HR(95%CI) | |
|---|---|---|---|---|---|---|
| 年龄 | 0.019 | 0.006 | 3.418 | <0.001 | 1.020(1.008~1.031) | |
| Hb | -0.009 | 0.003 | -3.508 | <0.001 | 0.991(0.985~0.996) | |
| ALB | -0.024 | 0.013 | -1.812 | 0.070 | 0.977(0.952~1.002) | |
| TBil | 0.001 | 0.001 | 2.062 | 0.039 | 1.002(1.001~1.003) | |
| INR | 0.370 | 0.149 | 2.477 | 0.013 | 1.453(1.080~1.953) | |
| SCr | -0.001 | 0.002 | -0.352 | 0.719 | 0.999(0.996~1.003) | |
| TSA | 0.002 | 0.001 | 4.816 | <0.001 | 1.002(1.001 ~1.003) | |
| 腹水分级 | 4.724 | 0.094 | ||||
| 中量 | 0.249 | 0.160 | 1.556 | 0.123 | 1.281(0.936~1.530) | |
| 大量 | 0.486 | 0.192 | 2.527 | 0.012 | 1.622(1.111~2.369) | |
| 肝性脑病 | 0.568 | 0.188 | 3.023 | 0.003 | 1.756(1.207~2.554) | |
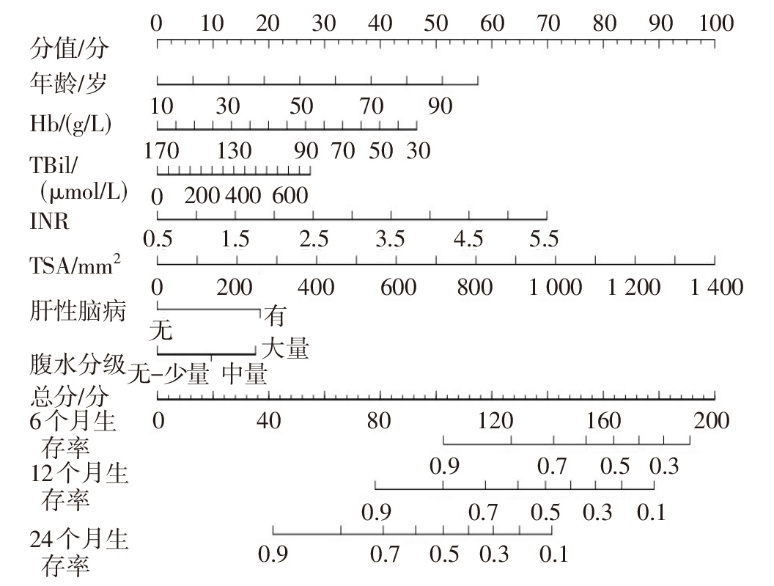
图2 预测HBV-DC患者预后的列线图
Fig.2 Nomogram for predicting prognosis in patients with HBV-DC
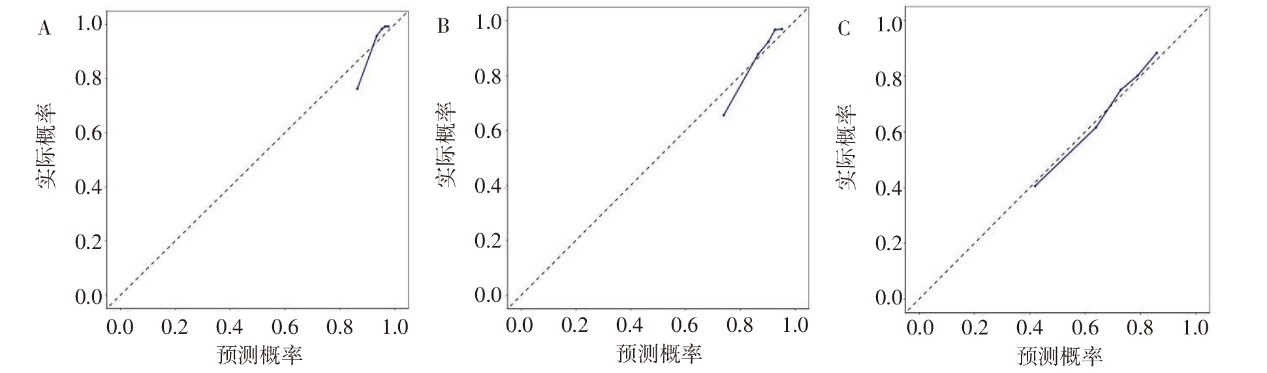
图3 列线图预测模型的校准曲线 A:6个月;B:12个月;C:24个月;图4、5同。
Fig.3 Calibration curve of the nomogram prediction model
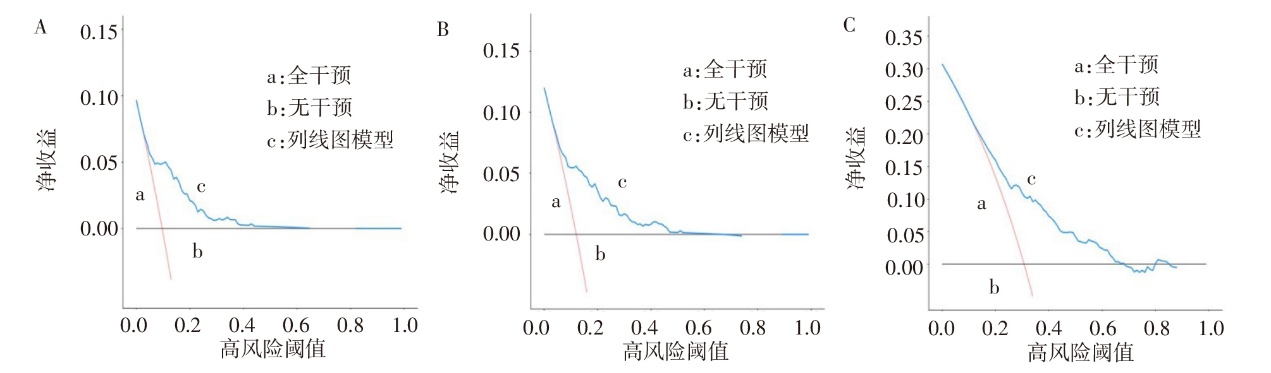
图4 列线图预测模型的决策曲线
Fig.4 Decision curve of the nomogram prediction model
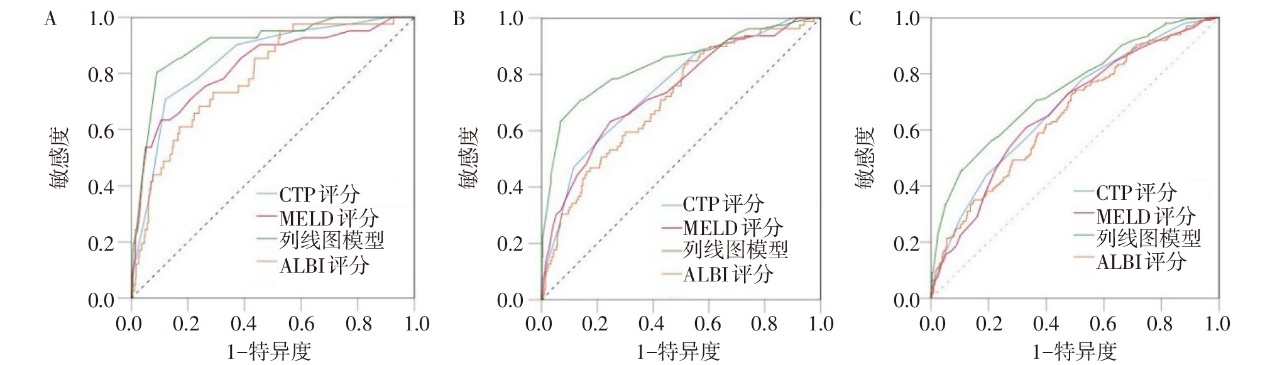
图5 列线图模型、CTP评分、MELD评分及ALBI评分预测HBV-DC患者生存率的ROC曲线
Fig.5 ROC curves of nomogram model, CTP score, MELD score and ALBI score for predicting the survival rate of HBV-DC patients
| 项目 | AUC (95%CI) | 敏感度/ % | 特异度/ % | 截断值 | 约登 指数 |
|---|---|---|---|---|---|
| 6个月生存率 | |||||
| 列线图模型 | 0.904(0.878~0.925) | 80.5 | 91.0 | 0.568 | 0.715 |
| ALBI评分 | 0.790(0.756~0.821) | 73.2 | 71.2 | -1.179分 | 0.444 |
| CTP评分 | 0.848(0.818~0.875) | 70.7 | 88.0 | 11分 | 0.587 |
| MELD评分 | 0.826(0.794~0.854) | 63.4 | 89.5 | 20分 | 0.529 |
| 12个月生存率 | |||||
| 列线图模型 | 0.837(0.806~0.865) | 70.9 | 85.9 | 0.457 | 0.568 |
| ALBI评分 | 0.709(0.672~0.744) | 84.8 | 47.5 | -1.525分 | 0.323 |
| CTP评分 | 0.762(0.727~0.795) | 60.8 | 77.8 | 10分 | 0.386 |
| MELD评分 | 0.753(0.717~0.786) | 67.1 | 75.3 | 16分 | 0.424 |
| 24个月生存率 | |||||
| 列线图模型 | 0.744(0.708~0.777) | 56.4 | 78.8 | 0.387 | 0.352 |
| ALBI评分 | 0.654(0.616~0.691) | 73.1 | 50.9 | -1.525分 | 0.240 |
| CTP评分 | 0.687(0.649~0.722) | 78.7 | 47.3 | 8分 | 0.260 |
| MELD评分 | 0.673(0.636~0.710) | 61.9 | 66.9 | 14分 | 0.288 |
表5 列线图模型、CTP评分、MELD评分及ALBI评分对HBV-DC患者预后的预测价值
Tab.5 Predictive value of nomogram model, CTP score,MELD score and ALBI score for the prognosis of patients with HBV-DC
| 项目 | AUC (95%CI) | 敏感度/ % | 特异度/ % | 截断值 | 约登 指数 |
|---|---|---|---|---|---|
| 6个月生存率 | |||||
| 列线图模型 | 0.904(0.878~0.925) | 80.5 | 91.0 | 0.568 | 0.715 |
| ALBI评分 | 0.790(0.756~0.821) | 73.2 | 71.2 | -1.179分 | 0.444 |
| CTP评分 | 0.848(0.818~0.875) | 70.7 | 88.0 | 11分 | 0.587 |
| MELD评分 | 0.826(0.794~0.854) | 63.4 | 89.5 | 20分 | 0.529 |
| 12个月生存率 | |||||
| 列线图模型 | 0.837(0.806~0.865) | 70.9 | 85.9 | 0.457 | 0.568 |
| ALBI评分 | 0.709(0.672~0.744) | 84.8 | 47.5 | -1.525分 | 0.323 |
| CTP评分 | 0.762(0.727~0.795) | 60.8 | 77.8 | 10分 | 0.386 |
| MELD评分 | 0.753(0.717~0.786) | 67.1 | 75.3 | 16分 | 0.424 |
| 24个月生存率 | |||||
| 列线图模型 | 0.744(0.708~0.777) | 56.4 | 78.8 | 0.387 | 0.352 |
| ALBI评分 | 0.654(0.616~0.691) | 73.1 | 50.9 | -1.525分 | 0.240 |
| CTP评分 | 0.687(0.649~0.722) | 78.7 | 47.3 | 8分 | 0.260 |
| MELD评分 | 0.673(0.636~0.710) | 61.9 | 66.9 | 14分 | 0.288 |
| [1] | ZAMANI M, ALIZADEH-TABARI S, AJMERA V, et al. Global prevalence of advanced liver fibrosis and cirrhosis in the general population: a systematic review and meta-analysis[J]. Clin Gastroenterol Hepatol, 2025, 23(7):1123-1134. doi:10.1016/j.cgh.2024.08.020. |
| [2] | YI F, GUO X, WANG L, et al. Impact of spontaneous splenorenal shunt on liver volume and long-term survival of liver cirrhosis[J]. J Gastroenterol Hepatol, 2021, 36(6):1694-1702. doi:10.1111/jgh.15386. |
| [3] | SIMÓN-TALERO M, ROCCARINA D, MARTÍNEZ J, et al. Association between portosystemic shunts and increased complications and mortality in patients with cirrhosis[J]. Gastroenterology, 2018, 154(6):1694-1705.e4. doi:10.1053/j.gastro.2018.01.028. |
| [4] | PRAKTIKNJO M, SIMÓN-TALERO M, RÖMER J, et al. Total area of spontaneous portosystemic shunts independently predicts hepatic encephalopathy and mortality in liver cirrhosis[J]. J Hepatol, 2020, 72(6):1140-1150. doi:10.1016/j.jhep.2019.12.021. |
| [5] | TURCO L, GARCIA-TSAO G, MAGNANI I, et al. Cardiopulmonary hemodynamics and C-reactive protein as prognostic indicators in compensated and decompensated cirrhosis[J]. J Hepatol, 2018, 68(5):949-958. doi:10.1016/j.jhep.2017.12.027. |
| [6] | ABRALDES J G, TREBICKA J, CHALASANI N, et al. Prioritization of therapeutic targets and trial design in cirrhotic portal hypertension[J]. Hepatology, 2019, 69(3):1287-1299. doi:10.1002/hep.30314. |
| [7] | HEO S, LEE S S, CHOI S H, et al. CT rule-in and rule-out criteria for clinically significant portal hypertension in chronic liver disease[J]. Radiology, 2023, 309(1):e231208. doi:10.1148/radiol.231208. |
| [8] | NARDELLI S, RIGGIO O, TURCO L, et al. Relevance of spontaneous portosystemic shunts detected with CT in patients with cirrhosis[J]. Radiology, 2021, 299(1):133-140. doi:10.1148/radiol.2021203051. |
| [9] | GREINERT R, ZIPPRICH A, SIMÓN-TALERO M, et al. Covert hepatic encephalopathy and spontaneous portosystemic shunts increase the risk of developing overt hepatic encephalopathy[J]. Liver Int, 2020, 40(12):3093-3102. doi:10.1111/liv.14660. |
| [10] | TARANTINO G, CITRO V, CONCA P, et al. What are the implications of the spontaneous spleno-renal shunts in liver cirrhosis?[J]. BMC Gastroenterol, 2009, 9:89. doi:10.1186/1471-230X-9-89. |
| [11] | LIPINSKI M, SABOROWSKI M, HEIDRICH B, et al. Clinical characteristics of patients with liver cirrhosis and spontaneous portosystemic shunts detected by ultrasound in a tertiary care and transplantation centre[J]. Scand J Gastroenterol, 2018, 53(9):1107-1113. doi:10.1080/00365521.2018.1498913. |
| [12] | SAKS K, JENSEN K K, MCLOUTH J, et al. Influence of spontaneous splenorenal shunts on clinical outcomes in decompensated cirrhosis and after liver transplantation[J]. Hepatol Commun, 2018, 2(4):437-444. doi:10.1002/hep4.1157. |
| [13] | VIDAL-GONZÁLEZ J, MARTÍNEZ J, MULAY A, et al. Evolution of spontaneous portosystemic shunts over time and following aetiological intervention in patients with cirrhosis[J]. JHEP Rep, 2023, 6(2):100977. doi:10.1016/j.jhepr.2023.100977. |
| [14] | DAJTI E, RENZULLI M, COLECCHIA A, et al. Size and location of spontaneous portosystemic shunts predict the risk of decompensation in cirrhotic patients[J]. Dig Liver Dis, 2022, 54(1):103-110. doi:10.1016/j.dld.2020.12.114. |
| [15] | SAAD W E. Portosystemic shunt syndrome and endovascular management of hepatic encephalopathy[J]. Semin Intervent Radiol, 2014, 31(3):262-265. doi:10.1055/s-0034-1382795. |
| [16] | GINÈS P, KRAG A, ABRALDES J G, et al. Liver cirrhosis[J]. Lancet, 2021, 398(10308):1359-1376. doi:10.1016/S0140-6736(21)01374-X. |
| [17] | LLERENA VELASTEGUI J, VERA SANCHEZ M, Villacis Lopez C. Characteristics of spontaneous portosystemic shunts in cirrhotic patients as a predictor of decompensation[J]. Dig Liver Dis, 2022, 54(9):1285-1286. doi:10.1016/j.dld.2022.05.018. |
| [18] | SONG X, ROMEIRO F G, WANG J, et al. Development and validation of modified Liaoning score for predicting the prognosis of liver cirrhosis:a retrospective,international multicenter,observational study[J]. Expert Rev Gastroenterol Hepatol, 2024, 18(1/2/3):121-128. doi:10.1080/17474124.2024.2320238. |
| [19] | VIZZUTTI F, CELSA C, CALVARUSO V, et al. Mortality after transjugular intrahepatic portosystemic shunt in older adult patients with cirrhosis:a validated prediction model[J]. Hepatology, 2023, 77(2):476-488. doi:10.1002/hep.32704. |
| [1] | 董倩, 陈淑华, 张飞. ACE2在结直肠癌耐药中的作用及其预测价值的研究[J]. 天津医药, 2026, 54(6): 561-569. |
| [2] | 曹阳, 段朋仓, 李梦雨, 史方堃, 胡晨, 邢方圆, 李花莲. 脑小血管病总负荷联合血清8-OHDG、Ficolin-3对老年穿支动脉粥样硬化病预后的预测价值[J]. 天津医药, 2026, 54(6): 618-622. |
| [3] | 张富允, 蒋龙超, 杨学燕. 食管癌患者血清TM4SF1、KLF5、SOX3水平与预后的关系[J]. 天津医药, 2026, 54(6): 623-626. |
| [4] | 黄斐, 王利航, 孙官文, 包呼和, 杨鹏波, 张雅兴. 糖尿病足溃疡患者住院期间小截肢的预测模型构建及验证[J]. 天津医药, 2026, 54(5): 478-483. |
| [5] | 彭静, 余小倩. 结直肠癌术后患者肠内营养喂养不耐受的影响因素及预警模型的构建[J]. 天津医药, 2026, 54(5): 484-488. |
| [6] | 于波, 蒲肖琳, 刘乃婷, 李雅滨, 吴志茹. 消化道黏膜肿瘤患者EMR术后迟发性出血危险因素分析[J]. 天津医药, 2026, 54(5): 522-527. |
| [7] | 陈一铭, 戈超, 徐姝琪, 孙威, 戴颖, 徐选福. CYP1B1和PSMD14在结直肠癌中的表达及其对预后的影响[J]. 天津医药, 2026, 54(4): 412-416. |
| [8] | 项亚娟, 陈长春, 张璐. 预后营养指数联合血清指标对急性脑梗死患者预后的预测价值[J]. 天津医药, 2026, 54(4): 423-428. |
| [9] | 李斌, 谭振刚, 张华清. 基于息肉特征和血清学指标构建结直肠息肉复发风险预测模型及效能分析[J]. 天津医药, 2026, 54(3): 249-253. |
| [10] | 张润春, 李树华, 王玉珍, 王巧文. 肺炎支原体肺炎患儿血清LXA4和KLF5表达的临床意义[J]. 天津医药, 2026, 54(3): 269-274. |
| [11] | 朱海燕, 王烨, 尹艳. 老年NSCLC患者术后胃肠功能紊乱的危险因素研究[J]. 天津医药, 2026, 54(3): 289-294. |
| [12] | 刘晓华, 韩婷婷, 高玉杰. 增强CT淋巴结边缘特征联合IPI对难治性弥漫大B细胞巴瘤的预测价值[J]. 天津医药, 2026, 54(3): 303-308. |
| [13] | 余优佳, 秦夏. 外周灌注指数联合血浆容量对感染性休克患者预后的评估价值[J]. 天津医药, 2026, 54(2): 169-172. |
| [14] | 周乔枝, 武红娟, 王科程. 慢性心力衰竭患者血浆海蟾蜍毒素、Ⅰ型胶原α1链表达水平及其与预后的相关性[J]. 天津医药, 2026, 54(2): 184-188. |
| [15] | 陈丽, 陈楠. COPD进展为Ⅱ型呼吸衰竭预警模型的建立与验证[J]. 天津医药, 2026, 54(2): 189-195. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||