天津医药 ›› 2026, Vol. 54 ›› Issue (2): 189-195.doi: 10.11958/20252555
陈丽1( ), 陈楠2
), 陈楠2
收稿日期:2025-07-21
修回日期:2025-10-13
出版日期:2026-02-15
发布日期:2026-02-12
作者简介:陈丽(1983),女,主治医师,主要从事普通内科方面研究。E-mail:
CHEN Li1(), CHEN Nan2
Received:2025-07-21
Revised:2025-10-13
Published:2026-02-15
Online:2026-02-12
陈丽, 陈楠. COPD进展为Ⅱ型呼吸衰竭预警模型的建立与验证[J]. 天津医药, 2026, 54(2): 189-195.
CHEN Li, CHEN Nan. Establishment and verification of the early warning model for COPD progressing to type II respiratory failure[J]. Tianjin Medical Journal, 2026, 54(2): 189-195.
摘要:
目的 建立并验证慢性阻塞性肺疾病(COPD)进展为Ⅱ型呼吸衰竭潜在高危人群的早期风险预警模型。方法 采用分层随机抽样法将符合纳入标准的297例急性期住院治疗后转为稳定期的COPD患者按照7∶3分为建模集(n=208)与验证集(n=89)。将建模集患者按照再次急性加重是否进展为Ⅱ型呼吸衰竭分为进展组(n=81)和非进展组(n=127)。比较进展组与非进展组临床资料,采用随机森林初步筛选预测特征变量,经最小绝对收缩和选择算子(LASSO)回归进一步压缩筛选出重要预测特征变量,构建并验证列线图预警识别模型。结果 建模集与验证集患者年龄、性别、体质量指数、既往史、稳定期治疗方案、病程、COPD防治全球倡仪(GOLD)肺功能分级、过去1年急性加重次数、肌少症及实验室检查指标[白细胞、血红蛋白、血小板、中性粒细胞、嗜酸性粒细胞(EOS)、白蛋白、肺泡表面活性蛋白-D(SP-D)]比较差异无统计学意义;建模集中进展组年龄、GOLD肺功能分级、过去1年急性加重次数≥2次患者占比、肌少症患者占比、EOS、SP-D高于非进展组,病程长于非进展组,白蛋白低于非进展组(P<0.05),基于此随机森林筛选出前6位重要特征变量依次为病程、GOLD肺功能分级、过去1年急性加重次数、肌少症、EOS、SP-D,经LASSO进一步压缩后最终确定GOLD肺功能分级、过去1年急性加重次数、肌少症、EOS、SP-D是COPD进展为Ⅱ型呼吸衰竭的重要预测因子(P<0.05);基于此构建的预警识别模型一致性指数(C-index)为0.904;受试者工作特征曲线显示,在建模集与验证集中,该模型的曲线下面积分别为0.904(95%CI:0.860~0.948)、0.924(95%CI:0.861~0.986);校准曲线、决策曲线结果显示,该模型具有良好的校准性、临床适用性。结论 基于预测因子构建的列线图预警识别模型具有良好的预测性能及临床适用性。
中图分类号:
| 组别 | n | 年龄/岁 | 性别 | BMI/ (kg/m2) | 合并症 | 吸烟 | 饮酒 | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | 糖尿病 | 高血压 | 冠心病 | |||||||||||||||||||||||||||
| 建模集 | 208 | 66.49±9.30 | 149(71.63) | 59(28.37) | 22.90±0.74 | 42(20.19) | 52(25.00) | 23(11.06) | 81(38.94) | 19(9.13) | |||||||||||||||||||||
| 验证集 | 89 | 66.53±8.11 | 69(77.53) | 20(22.47) | 22.85±0.68 | 21(23.60) | 18(20.22) | 6(6.74) | 29(32.58) | 11(12.36) | |||||||||||||||||||||
| t或χ2 | 0.035 | 1.109 | 0.546 | 0.432 | 0.789 | 1.318 | 1.080 | 0.714 | |||||||||||||||||||||||
| 组别 | 稳定期治疗方案 | 病程/ 年 | GOLD肺功能分级 | 过去1年急性加重次数 | |||||||||||||||||||||||||||
| 吸入糖皮质激素 | 支气管扩张剂 | 无创通气 | 祛痰药 | 面罩长期氧疗 | Ⅱ | Ⅲ | Ⅳ | <2次 | ≥2次 | ||||||||||||||||||||||
| 建模集 | 201(96.63) | 89(42.79) | 54(25.96) | 59(28.37) | 51(24.52) | 6.20±2.05 | 110(52.88) | 66(31.73) | 32(15.38) | 47(22.60) | 161(77.40) | ||||||||||||||||||||
| 验证集 | 82(92.13) | 41(46.07) | 20(22.47) | 29(32.58) | 16(17.98) | 6.31±1.94 | 50(56.18) | 24(26.97) | 15(16.85) | 25(28.09) | 64(71.91) | ||||||||||||||||||||
| t、χ2或u | 2.810 | 0.272 | 0.406 | 0.532 | 1.527 | 0.430 | 0.678 | 1.024 | |||||||||||||||||||||||
| 组别 | 肌少症 | 实验室检查 | |||||||||||||||||||||||||||||
| 白细胞/(×109/L) | 血红蛋白/(g/L) | 血小板/(×109/L) | 中性粒细胞 | EOS | 白蛋白/(g/L) | SP-D/(μg/L) | |||||||||||||||||||||||||
| 建模集 | 19(9.13) | 6.27±0.83 | 109.56±11.32 | 202.55±26.17 | 0.54±0.17 | 0.02±0.01 | 36.15±2.79 | 50.78±16.90 | |||||||||||||||||||||||
| 验证集 | 13(14.61) | 6.18±0.75 | 110.42±13.08 | 198.43±27.65 | 0.53±0.16 | 0.02±0.01 | 36.20±2.48 | 51.20±14.37 | |||||||||||||||||||||||
| t或χ2 | 1.941 | 0.881 | 0.572 | 1.222 | 0.473 | 0.000 | 0.146 | 0.205 | |||||||||||||||||||||||
表1 建模集与验证集患者的临床资料比较
Tab.1 Comparison of clinical data of patients between the modeling set and the validation set
| 组别 | n | 年龄/岁 | 性别 | BMI/ (kg/m2) | 合并症 | 吸烟 | 饮酒 | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | 糖尿病 | 高血压 | 冠心病 | |||||||||||||||||||||||||||
| 建模集 | 208 | 66.49±9.30 | 149(71.63) | 59(28.37) | 22.90±0.74 | 42(20.19) | 52(25.00) | 23(11.06) | 81(38.94) | 19(9.13) | |||||||||||||||||||||
| 验证集 | 89 | 66.53±8.11 | 69(77.53) | 20(22.47) | 22.85±0.68 | 21(23.60) | 18(20.22) | 6(6.74) | 29(32.58) | 11(12.36) | |||||||||||||||||||||
| t或χ2 | 0.035 | 1.109 | 0.546 | 0.432 | 0.789 | 1.318 | 1.080 | 0.714 | |||||||||||||||||||||||
| 组别 | 稳定期治疗方案 | 病程/ 年 | GOLD肺功能分级 | 过去1年急性加重次数 | |||||||||||||||||||||||||||
| 吸入糖皮质激素 | 支气管扩张剂 | 无创通气 | 祛痰药 | 面罩长期氧疗 | Ⅱ | Ⅲ | Ⅳ | <2次 | ≥2次 | ||||||||||||||||||||||
| 建模集 | 201(96.63) | 89(42.79) | 54(25.96) | 59(28.37) | 51(24.52) | 6.20±2.05 | 110(52.88) | 66(31.73) | 32(15.38) | 47(22.60) | 161(77.40) | ||||||||||||||||||||
| 验证集 | 82(92.13) | 41(46.07) | 20(22.47) | 29(32.58) | 16(17.98) | 6.31±1.94 | 50(56.18) | 24(26.97) | 15(16.85) | 25(28.09) | 64(71.91) | ||||||||||||||||||||
| t、χ2或u | 2.810 | 0.272 | 0.406 | 0.532 | 1.527 | 0.430 | 0.678 | 1.024 | |||||||||||||||||||||||
| 组别 | 肌少症 | 实验室检查 | |||||||||||||||||||||||||||||
| 白细胞/(×109/L) | 血红蛋白/(g/L) | 血小板/(×109/L) | 中性粒细胞 | EOS | 白蛋白/(g/L) | SP-D/(μg/L) | |||||||||||||||||||||||||
| 建模集 | 19(9.13) | 6.27±0.83 | 109.56±11.32 | 202.55±26.17 | 0.54±0.17 | 0.02±0.01 | 36.15±2.79 | 50.78±16.90 | |||||||||||||||||||||||
| 验证集 | 13(14.61) | 6.18±0.75 | 110.42±13.08 | 198.43±27.65 | 0.53±0.16 | 0.02±0.01 | 36.20±2.48 | 51.20±14.37 | |||||||||||||||||||||||
| t或χ2 | 1.941 | 0.881 | 0.572 | 1.222 | 0.473 | 0.000 | 0.146 | 0.205 | |||||||||||||||||||||||
| 组别 | n | 年龄/岁 | 性别 | BMI/ (kg/m2) | 病程/ 年 | 合并症 | 吸烟 | 饮酒 | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | 糖尿病 | 高血压 | 冠心病 | ||||||||||||||||||||||||||
| 非进展组 | 127 | 65.20±8.13 | 89(70.08) | 38(29.92) | 22.95±0.57 | 5.56±1.80 | 23(18.11) | 30(23.62) | 11(8.66) | 46(36.22) | 13(10.24) | |||||||||||||||||||
| 进展组 | 81 | 68.51±6.40 | 60(74.07) | 21(25.93) | 22.82±0.63 | 7.20±1.95 | 19(23.46) | 22(27.16) | 12(14.81) | 35(43.21) | 6(7.41) | |||||||||||||||||||
| t或χ2 | 3.101** | 0.389 | 1.539 | 6.202** | 0.877 | 0.330 | 1.904 | 1.016 | 0.477 | |||||||||||||||||||||
| 组别 | 稳定期治疗方案 | GOLD肺功能分级 | 过去1年急性加重次数 | |||||||||||||||||||||||||||
| 吸入糖皮质激素 | 支气管扩张剂 | 无创通气 | 祛痰药 | 面罩长期氧疗 | Ⅱ | Ⅲ | Ⅳ | <2次 | ≥2次 | |||||||||||||||||||||
| 非进展组 | 124(97.64) | 53(41.73) | 34(26.77) | 36(28.35) | 33(25.98) | 86(67.72) | 31(24.41) | 10(7.87) | 41(32.28) | 86(67.72) | ||||||||||||||||||||
| 进展组 | 77(95.06) | 36(44.44) | 20(24.69) | 23(28.40) | 18(22.22) | 24(29.63) | 35(43.21) | 22(27.16) | 6(7.41) | 75(92.59) | ||||||||||||||||||||
| t、χ2或u | 1.009 | 0.149 | 0.111 | 0.000 | 0.378 | 31.033** | 17.498** | |||||||||||||||||||||||
| 组别 | 肌少症 | 实验室检查 | ||||||||||||||||||||||||||||
| 白细胞/(×109/L) | 血红蛋白/(g/L) | 血小板/(×109/L) | 中性粒细胞 | EOS | 白蛋白/(g/L) | SP-D/(μg/L) | ||||||||||||||||||||||||
| 非进展组 | 3(2.36) | 6.16±0.55 | 110.02±11.26 | 203.11±24.58 | 0.54±0.15 | 0.02±0.01 | 37.13±2.52 | 45.20±14.83 | ||||||||||||||||||||||
| 进展组 | 16(19.75) | 6.20±0.78 | 108.85±9.43 | 201.66±19.75 | 0.53±0.14 | 0.03±0.01 | 34.62±2.00 | 59.53±15.18 | ||||||||||||||||||||||
| t或χ2 | 18.021** | 0.433 | 0.777 | 0.447 | 0.481 | 7.033** | 7.570** | 6.733** | ||||||||||||||||||||||
表2 建模集中进展组与非进展组患者的临床资料比较
Tab.2 Comparison of clinical data between the progressive group and the non-progressive group in the modeling set
| 组别 | n | 年龄/岁 | 性别 | BMI/ (kg/m2) | 病程/ 年 | 合并症 | 吸烟 | 饮酒 | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | 糖尿病 | 高血压 | 冠心病 | ||||||||||||||||||||||||||
| 非进展组 | 127 | 65.20±8.13 | 89(70.08) | 38(29.92) | 22.95±0.57 | 5.56±1.80 | 23(18.11) | 30(23.62) | 11(8.66) | 46(36.22) | 13(10.24) | |||||||||||||||||||
| 进展组 | 81 | 68.51±6.40 | 60(74.07) | 21(25.93) | 22.82±0.63 | 7.20±1.95 | 19(23.46) | 22(27.16) | 12(14.81) | 35(43.21) | 6(7.41) | |||||||||||||||||||
| t或χ2 | 3.101** | 0.389 | 1.539 | 6.202** | 0.877 | 0.330 | 1.904 | 1.016 | 0.477 | |||||||||||||||||||||
| 组别 | 稳定期治疗方案 | GOLD肺功能分级 | 过去1年急性加重次数 | |||||||||||||||||||||||||||
| 吸入糖皮质激素 | 支气管扩张剂 | 无创通气 | 祛痰药 | 面罩长期氧疗 | Ⅱ | Ⅲ | Ⅳ | <2次 | ≥2次 | |||||||||||||||||||||
| 非进展组 | 124(97.64) | 53(41.73) | 34(26.77) | 36(28.35) | 33(25.98) | 86(67.72) | 31(24.41) | 10(7.87) | 41(32.28) | 86(67.72) | ||||||||||||||||||||
| 进展组 | 77(95.06) | 36(44.44) | 20(24.69) | 23(28.40) | 18(22.22) | 24(29.63) | 35(43.21) | 22(27.16) | 6(7.41) | 75(92.59) | ||||||||||||||||||||
| t、χ2或u | 1.009 | 0.149 | 0.111 | 0.000 | 0.378 | 31.033** | 17.498** | |||||||||||||||||||||||
| 组别 | 肌少症 | 实验室检查 | ||||||||||||||||||||||||||||
| 白细胞/(×109/L) | 血红蛋白/(g/L) | 血小板/(×109/L) | 中性粒细胞 | EOS | 白蛋白/(g/L) | SP-D/(μg/L) | ||||||||||||||||||||||||
| 非进展组 | 3(2.36) | 6.16±0.55 | 110.02±11.26 | 203.11±24.58 | 0.54±0.15 | 0.02±0.01 | 37.13±2.52 | 45.20±14.83 | ||||||||||||||||||||||
| 进展组 | 16(19.75) | 6.20±0.78 | 108.85±9.43 | 201.66±19.75 | 0.53±0.14 | 0.03±0.01 | 34.62±2.00 | 59.53±15.18 | ||||||||||||||||||||||
| t或χ2 | 18.021** | 0.433 | 0.777 | 0.447 | 0.481 | 7.033** | 7.570** | 6.733** | ||||||||||||||||||||||
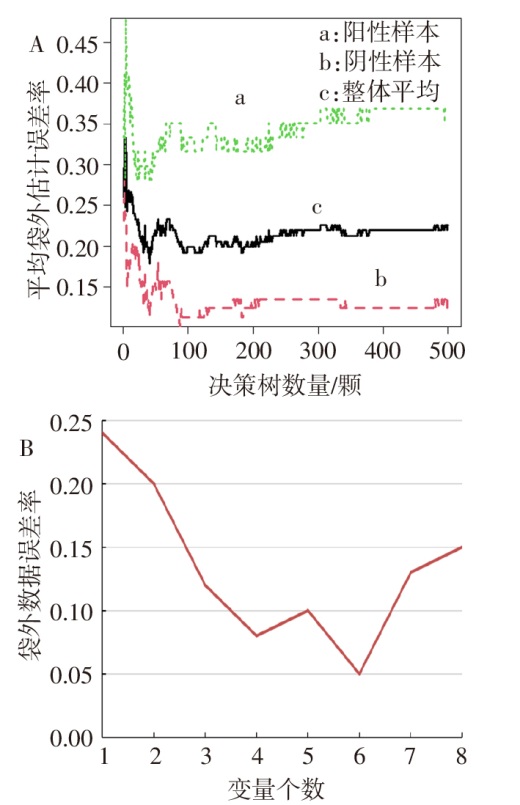
图1 COPD进展为Ⅱ型呼吸衰竭预测变量的随机森林分析结果 A:袋外样本的估计误差率图;B:决策树数量与平均袋外估计误差率变化图。
Fig.1 The results of random forest analysis of predictors of COPD progression to type Ⅱ respiratory failure
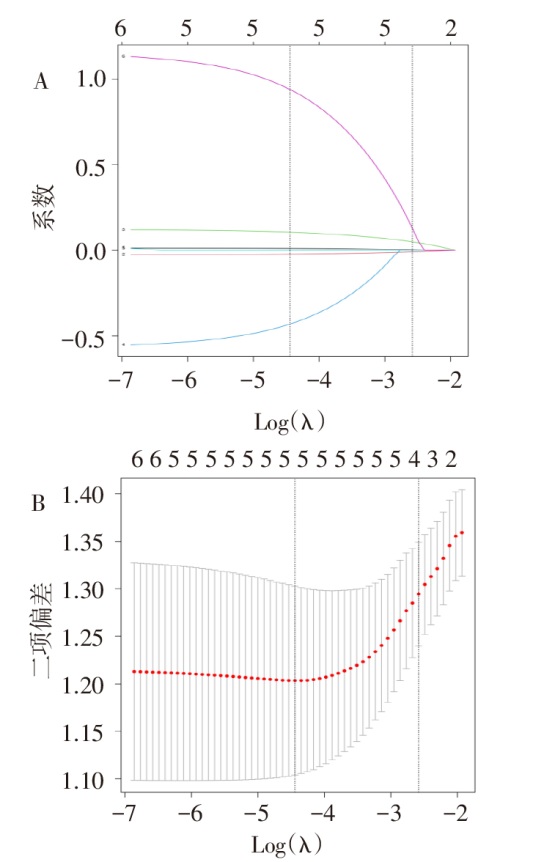
图2 COPD进展为Ⅱ型呼吸衰竭预测变量的LASSO回归分析 A:各变量系数随λ变化情况图;B:最佳惩罚系数λ选择图(1为病程、2为过去1年急性加重次数、3为EOS、4为SP-D、5为肌少症、6为GOLD肺功能分级)。
Fig. 2 LASSO regression analysis of predictive variables for COPD progression to type Ⅱ respiratory failure
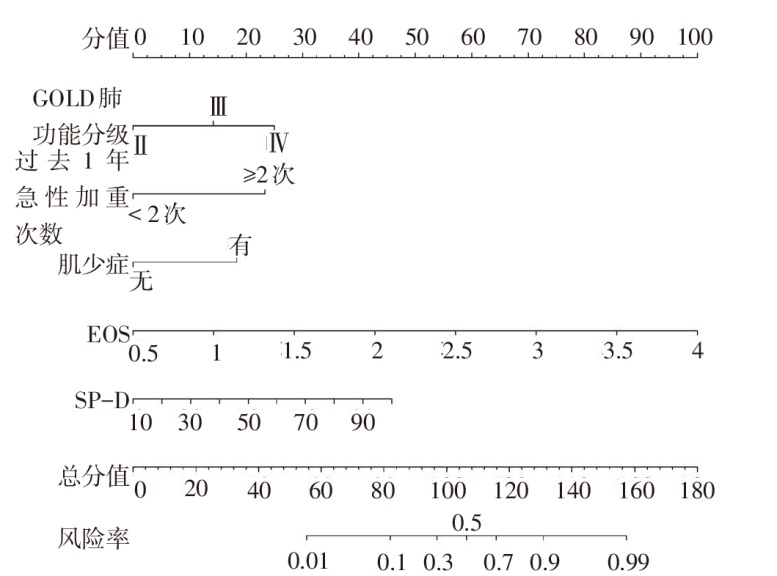
图3 COPD进展为Ⅱ型呼吸衰竭潜在高危人群早期预警识别列线图
Fig.3 Establishment of early warning and identification model for potential high-risk population of COPD progression to type Ⅱ respiratory failure
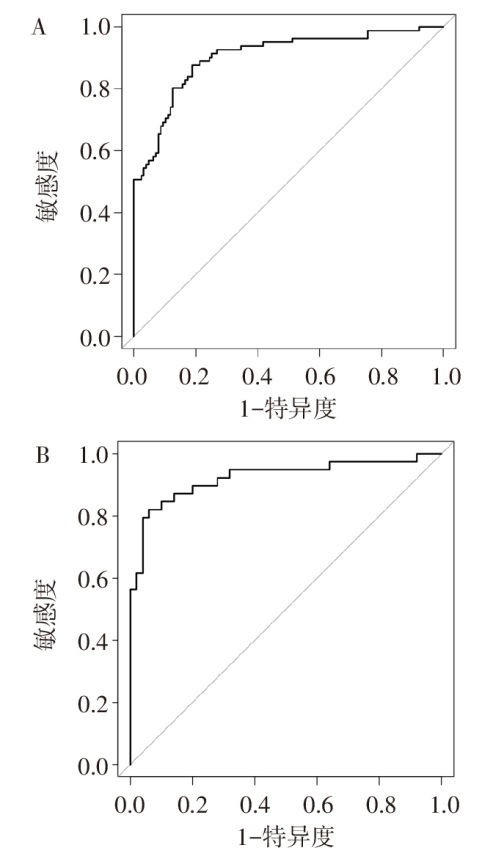
图4 COPD进展为Ⅱ型呼吸衰竭预测模型的ROC曲线 A:建模集;B:验证集。
Fig.4 ROC curve of COPD progression to type Ⅱ respiratory failure prediction model
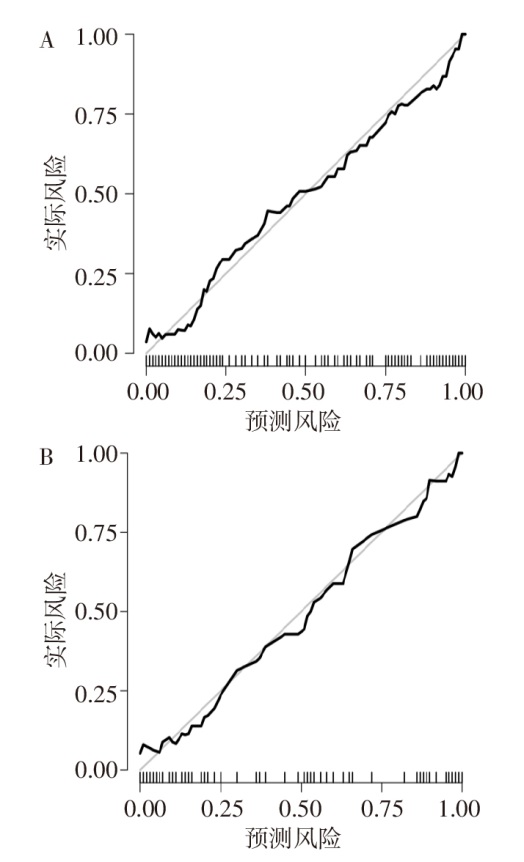
图5 COPD进展为Ⅱ型呼吸衰竭预测模型的校准曲线 A:建模集;B:验证集。
Fig.5 Calibration curve of COPD progression to type Ⅱ respiratory failure prediction model
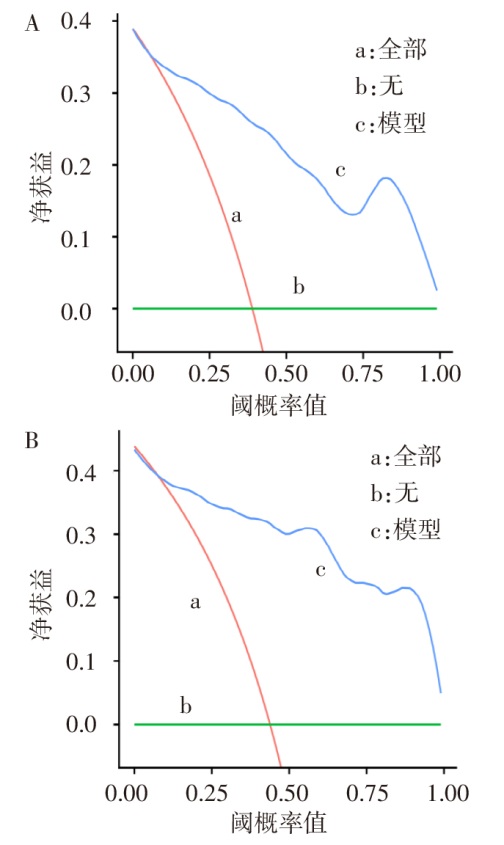
图6 COPD进展为Ⅱ型呼吸衰竭预测模型的DCA曲线 A:建模集;B:验证集。
Fig.6 DCA curve of COPD progression to type Ⅱ respiratory failure prediction model
| [1] | HE J, LUO W, MEI Y, et al. Nalmefene combined noninvasive positive-pressure ventilation in Chinese patients with chronic obstructive pulmonary disease coupled with type II respiratory failure:a meta-analysis[J]. Medicine(Baltimore), 2023, 102(31):e34624. doi:10.1097/MD.0000000000034624. |
| [2] | 屠昌明, 田园, 汪鹏程, 等. SII、RAR与AECOPD患者病情严重程度及并发呼吸衰竭的关系[J]. 天津医药, 2024, 52(12):1317-1321. |
| TU C M, TIAN Y, WANG P C, et al. Relationship between SII,RAR and severity of disease and respiratory failure in patients with AECOPD[J]. Tianjin Med J, 2024, 52(12):1317-1321. doi:10.11958/20241172. | |
| [3] | 周丹, 陈灵敏, 陈钢强, 等. 构建Nomogram预测模型探讨慢性阻塞性肺疾病患者并发呼吸衰竭的危险因素[J]. 中国急救医学, 2023, 43(5):383-387. |
| ZHOU D, CHEN L M, CHEN G Q, et al. Constructing a nomogram prediction model to explore the risk factors of respiratory failure in patients with chronic obstructive pulmonary disease[J]. Chin J Emerg Med, 2023, 43(5):383-387. doi:10.3969/j.issn.1002-1949.2023.05.009. | |
| [4] | 顾馨雨, 於江泉, 杨艳霞, 等. 慢性阻塞性肺疾病急性加重期并发呼吸衰竭危险因素的Meta分析[J]. 实用心脑肺血管病杂志, 2023, 31(5):82-88,95. |
| GU X Y, YU J Q, YANG Y X, et al. Meta analysis of risk factors for respiratory failure in acute exacerbation of chronic obstructive pulmonary disease[J]. J Pract Cardiovasc Cerebrovasc Dis, 2023, 31(5):82-88,95. doi:10.12114/j.issn.1008-5971.2023.00.080. | |
| [5] | CHEN L, LU L, FANG Y, et al. Glasgow Coma Scale on admission as predictor of neurological sequelae at discharge and acute respiratory failure in patients with heatstroke[J]. Postgrad Med J, 2023, 99(1178):1237-1245. doi:10.1093/postmj/qgad071. |
| [6] | WU Z, CHEN H, KE S, et al. Identifying potential biomarkers of idiopathic pulmonary fibrosis through machine learning analysis[J]. Sci Rep, 2023, 13(1):16559. doi:10.1038/s41598-023-43834-z. |
| [7] | VESTBO J, HURD S S, AGUSTÍ A G, et al. Global strategy for the diagnosis,management,and prevention of chronic obstructive pulmonary disease:GOLD executive summary[J]. Am J Respir Crit Care Med, 2013, 187(4):347-365. doi:10.1164/rccm.201204-0596PP. |
| [8] | BARUA R S, RIGOTTI N A, BENOWITZ N L, et al. 2018 ACC Expert Consensus Decision Pathway on Tobacco Cessation Treatment:a report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents[J]. J Am Coll Cardiol, 2018, 72(25):3332-3365. doi:10.1016/j.jacc.2018.10.027. |
| [9] | 中华预防医学会, 中华预防医学会心脏病预防与控制专业委员会, 中华医学会糖尿病学分会, 等. 中国健康生活方式预防心血管代谢疾病指南[J]. 中国循环杂志, 2020, 35(3):209-230. |
| Chinese Preventive Medicine Association, Chinese Preventive Medicine Association Heart Disease Prevention and Control Professional Committee, Chinese Medical Association Diabetes Branch, et al. Guidelines for preventing cardiovascular metabolic diseases through healthy lifestyle in China[J]. Chin J Circulat, 2020, 35(3):209-230. doi:10.3969/j.issn.1000-3614.2020.03.001. | |
| [10] | LAMBA T S, SHARARA R S, SINGH A C, et al. Pathophysiology and classification of respiratory failure[J]. Crit Care Nurs Q, 2016, 39(2):85-93. doi:10.1097/CNQ.0000000000000102. |
| [11] | HUR K Y, MOON M K, PARK J S, et al. 2021 Clinical Practice Guidelines for Diabetes Mellitus of the Korean Diabetes Association[J]. Diabetes Metab J, 2021, 45(4):461-481. doi:10.4093/dmj.2021.0156. |
| [12] | WHELTON P K, CAREY R M, ARONOW W S, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention,Detection,Evaluation,and Management of High Blood Pressure in Adults:a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines[J]. Hypertension, 2018, 71(6):e13-e115. doi:10.1161/HYP.0000000000000065. |
| [13] | YAMAGISHI M, TAMAKI N, AKASAKA T, et al. Jcs 2018 guideline on diagnosis of chronic coronary heart diseases[J]. Circ J, 2021, 85(4):402-572. doi:10.1253/circj.CJ-19-1131. |
| [14] | CRUZ-JENTOFT A J, BAHAT G, BAUER J, et al. Sarcopenia:revised European consensus on definition and diagnosis[J]. Age Ageing, 2019, 48(4):601. doi:10.1093/ageing/afz046. |
| [15] | MONTES DE OCA M, LÓPEZ VARELA M V, LAUCHO-CONTRERAS M E, et al. Classification of patients with chronic obstructive pulmonary disease according to the Latin American Thoracic Association (ALAT) staging systems and the global initiative for chronic obstructive pulmonary disease (GOLD)[J]. Arch Bronconeumol, 2017, 53(3):98-106. doi:10.1016/j.arbres.2016.08.015. |
| [16] | XU X, MA D, ZHOU F. Efficacy of naloxone combined with noninvasive ventilator in the treatment of COPD complicated with type II respiratory failure[J]. Minerva Surg, 2022, 77(6):634-636. doi:10.23736/S2724-5691.21.09291-1. |
| [17] | 姜锐, 李雪娇, 贺银虹, 等. HI-NPPV治疗AECOPD合并严重II型呼吸衰竭的临床疗效[J]. 中南大学学报(医学版), 2024, 49(2):266-272. |
| JIANG R, LI X J, HE Y L, et al. Clinical efficacy of HI-NPPV in the treatment of AECOPD combined with severe type II respiratory failure[J]. J Centr South Univ Med Sci, 2024, 49(2):266-272. doi:10.11817/j.issn.1672-7347.230329. | |
| [18] | 王霞, 侯嘉. 外周血ADAM19 DNA甲基化生物标记物对慢性阻塞性肺疾病的诊断价值[J]. 宁夏医科大学学报, 2022, 44(8):823-828. |
| WANG X, HOU J. Diagnostic value of peripheral blood ADAM19 DNA methylation biomarkers for chronic obstructive pulmonary disease[J]. J Ningxia Med Univ, 2022, 44(8):823-828. doi:10.16050/j.cnki.issn1674-6309.2022.08.014. | |
| [19] | 卢新卫, 李海天, 王晶, 等. 慢性阻塞性肺疾病患者的肌肉量水平对病情进展的影响[J]. 公共卫生与预防医学, 2024, 35(1):96-99. |
| LU X W, LI H T, WANG J, et al. The impact of muscle mass level on disease progression in patients with chronic obstructive pulmonary disease[J]. Public Health Prevent Med, 2024, 35(1):96-99. doi:10.3969/j.issn.1006-2483.2024.01.022. | |
| [20] | 焦维克, 张文, 张灿辉, 等. 影响AECOPD合并CO2潴留患者应用全身糖皮质激素的相关因素分析[J]. 中华危重病急救医学, 2020, 32(9):1061-1066. |
| JIAO W K, ZHANG W, ZHANG C H, et al. Clinical investigation on the related factors for the application of systemic glucocorticoids in patients with acute exacerbation of chronic obstructive pulmonary disease with carbon dioxide retention[J]. Chin Crit Care Med, 2020, 32(9):1061-1066. doi:10.3760/cma.j.cn121430-20200302-00203. | |
| [21] | LV M Y, QIANG L X, LI Z H, et al. The lower the eosinophils,the stronger the inflammatory response? The relationship of different levels of eosinophils with the degree of inflammation in acute exacerbation chronic obstructive pulmonary disease (AECOPD)[J]. J Thorac Dis, 2021, 13(1):232-243. doi:10.21037/jtd-20-2178. |
| [22] | GÜNAYDIN F E, GÜNLÜOĞLU G, KALKAN N, et al. The relationship between serum levels of surfactant protein D in COPD exacerbation severity and mortality[J]. Turk J Med Sci, 2019, 49(3):888-893. doi:10.3906/sag-1809-6. |
| [23] | HRISTOVA V A, WATSON A, CHAERKADY R, et al. Multiomics links global surfactant dysregulation with airflow obstruction and emphysema in COPD[J]. ERJ Open Res, 2023, 9(3):00378-2022. doi:10.1183/23120541.00378-2022. |
| [1] | 李斌, 谭振刚, 张华清. 基于息肉特征和血清学指标构建结直肠息肉复发风险预测模型及效能分析[J]. 天津医药, 2026, 54(3): 249-253. |
| [2] | 赵丽, 马秀丽, 刘毅, 朱毅. 全麻下腹腔镜胃癌根治术后谵妄发生的危险因素分析[J]. 天津医药, 2026, 54(3): 259-264. |
| [3] | 朱海燕, 王烨, 尹艳. 老年NSCLC患者术后胃肠功能紊乱的危险因素研究[J]. 天津医药, 2026, 54(3): 289-294. |
| [4] | 刘晓华, 韩婷婷, 高玉杰. 增强CT淋巴结边缘特征联合IPI对难治性弥漫大B细胞巴瘤的预测价值[J]. 天津医药, 2026, 54(3): 303-308. |
| [5] | 楚兴, 刘磊, 杨华, 陈宏. 胆总管结石并发急性胆源性胰腺炎的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 35-40. |
| [6] | 陈敏, 夏莉, 朱荣媛, 王欣雨, 季骏. 拔除第一前磨牙正畸治疗后牙龈内陷的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 57-63. |
| [7] | 李贺, 马胜山, 孙阳, 武栋泽, 李小飞. 关节镜肩袖修补术后再撕裂风险的影响因素及预测模型构建[J]. 天津医药, 2026, 54(1): 64-69. |
| [8] | 刘志远, 杨声飞, 钱释然, 邓忆莲, 黎东伟, 李君久. 胸乳入路腔镜甲状腺术后早期低钙血症的危险因素分析及预测模型构建[J]. 天津医药, 2025, 53(8): 826-830. |
| [9] | 刘鹏勇, 刘梦友, 周昱, 管海, 田振, 胡浩, 岳晓松, 关倩楠. 甲状腺全切术后并发永久性甲状旁腺功能减退的危险因素及列线图建立[J]. 天津医药, 2025, 53(8): 850-855. |
| [10] | 金吴娟, 倪刚, 黄欣宇, 王羊洋. 老年消化道出血患者不良预后的列线图预测模型的构建与验证[J]. 天津医药, 2025, 53(7): 694-699. |
| [11] | 陈英, 郭长英, 张静, 李娟, 陈丰毅. 基于术前肺动脉压评估心脏移植术后右心衰竭的发生风险[J]. 天津医药, 2025, 53(7): 751-755. |
| [12] | 张瀚文, 李强, 杨雪莲, 杨化兰, 江梅, 黄澍. 不同溶栓方案治疗不同特征超早期急性脑梗死的效果分析[J]. 天津医药, 2025, 53(7): 770-775. |
| [13] | 李婉婷, 刘弘扬, 桑婧, 阮育凤, 徐丽, 李冬梅. 老年下肢骨折患者术后发生急性心脑血管意外的影响因素分析[J]. 天津医药, 2025, 53(6): 648-653. |
| [14] | 王欣欣, 许慧, 吴晓. 妊娠期肝内胆汁淤积症合并GDM孕妇不良妊娠结局的影响因素及预测模型构建[J]. 天津医药, 2025, 53(5): 503-508. |
| [15] | 董丹, 陈立娟, 俞荷花. 急性胰腺炎并发低血压的危险因素分析及预测模型建立[J]. 天津医药, 2025, 53(5): 509-513. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||