天津医药 ›› 2025, Vol. 53 ›› Issue (3): 287-292.doi: 10.11958/20241375
贾方( ), 李平, 李静, 尹路
), 李平, 李静, 尹路
收稿日期:2024-09-18
修回日期:2024-11-27
出版日期:2025-03-15
发布日期:2025-03-31
作者简介:贾方(1977),女,副主任医师,主要从事麻醉学的基础与临床方面研究。E-mail:
JIA Fang(), LI Ping, LI Jing, YIN Lu
Received:2024-09-18
Revised:2024-11-27
Published:2025-03-15
Online:2025-03-31
贾方, 李平, 李静, 尹路. 全膝关节置换术后神经认知功能障碍的影响因素及列线图模型的构建[J]. 天津医药, 2025, 53(3): 287-292.
JIA Fang, LI Ping, LI Jing, YIN Lu. Influencing factors of neurocognitive dysfunction after total knee arthroplasty and the construction of a nomogram model[J]. Tianjin Medical Journal, 2025, 53(3): 287-292.
摘要:
目的 探究全膝关节置换术(TKA)患者发生神经认知功能障碍(PND)的影响因素并构建列线图预测模型。方法 收集249例行TKA患者的临床资料并按照7∶3的比例将患者分为建模队列(n=174)和验证队列(n=75)。根据患者是否发生PND,将建模队列分为PND组(n=62)和非PND组(n=112),验证队列分为PND组(n=27)和非PND组(n=48)。分析TKA患者发生PND的影响因素,建立列线图预测模型并进行验证。结果 高衰弱评分、全身麻醉、单一镇痛方案、高疼痛视觉模拟评分(VAS)是PND的危险因素,高白蛋白和血红蛋白水平是PND的保护因素(均P<0.05)。构建列线图模型,预测建模队列和验证队列发生PND的曲线下面积(AUC)及其95%CI分别为0.875(0.824~0.925)、0.905(0.835~0.975);校准曲线分析结果发现,预测患者发生PND的风险和实际发生情况基本吻合,Hosmer-Lemeshow结果显示模型拟合较好;临床决策曲线结果显示该模型临床应用价值较高。结论 高衰弱评分、全身麻醉、单一镇痛方案、高VAS评分、低白蛋白和低血红蛋白水平可增加TKA患者发生PND的风险,本研究构建的列线图预测模型有助于临床识别PND高危人群。
中图分类号:
| 组别 | n | 性别 (男/女) | 年龄/岁 | BMI/ (kg/m2) | 呼吸系统 疾病(有/无) | 基础疾病 (有/无) | 衰弱 评分/分 | 术侧a | 手术 时间/min | 麻醉 时间/min | 术中 出血量/mL | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 建模队列 | 174 | 64/110 | 62.70±5.90 | 24.11±2.54 | 43/131 | 57/117 | 2.41±0.76 | 85/89 | 112.27±26.90 | 129.58±26.81 | 206.71±25.19 | |||||||||
| 验证队列 | 75 | 23/52 | 62.78±5.68 | 24.12±2.57 | 18/57 | 29/46 | 2.42±0.84 | 31/44 | 108.27±24.35 | 128.76±25.32 | 203.87±25.33 | |||||||||
| χ2或t | 0.862 | 0.090 | 0.016 | 0.014 | 0.809 | 0.103 | 1.190 | 1.108 | 0.225 | 0.888 | ||||||||||
| 组别 | 麻醉方式b | 镇痛方案c | VAS评分/分 | ALB/(g/L) | RBC/(×1012/L) | HB/(g/L) | WBC/(×109/L) | NEU/(×109/L) | LYM/(×109/L) | |||||||||||
| 建模队列 | 83/91 | 82/92 | 5.51±2.09 | 39.40±4.16 | 4.32±0.51 | 115.51±18.54 | 6.75±1.60 | 4.19±1.23 | 2.05±0.98 | |||||||||||
| 验证队列 | 34/41 | 38/37 | 5.55±1.86 | 39.17±4.49 | 4.38±0.46 | 114.22±16.93 | 6.74±1.63 | 4.27±1.16 | 2.07±0.94 | |||||||||||
| t | 0.118 | 0.263 | 0.126 | 0.393 | 0.886 | 0.515 | 0.053 | 0.445 | 0.219 | |||||||||||
表1 建模队列与验证队列基线资料对比
Tab.1 Comparison of baseline data between modeling queue and verification queue
| 组别 | n | 性别 (男/女) | 年龄/岁 | BMI/ (kg/m2) | 呼吸系统 疾病(有/无) | 基础疾病 (有/无) | 衰弱 评分/分 | 术侧a | 手术 时间/min | 麻醉 时间/min | 术中 出血量/mL | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 建模队列 | 174 | 64/110 | 62.70±5.90 | 24.11±2.54 | 43/131 | 57/117 | 2.41±0.76 | 85/89 | 112.27±26.90 | 129.58±26.81 | 206.71±25.19 | |||||||||
| 验证队列 | 75 | 23/52 | 62.78±5.68 | 24.12±2.57 | 18/57 | 29/46 | 2.42±0.84 | 31/44 | 108.27±24.35 | 128.76±25.32 | 203.87±25.33 | |||||||||
| χ2或t | 0.862 | 0.090 | 0.016 | 0.014 | 0.809 | 0.103 | 1.190 | 1.108 | 0.225 | 0.888 | ||||||||||
| 组别 | 麻醉方式b | 镇痛方案c | VAS评分/分 | ALB/(g/L) | RBC/(×1012/L) | HB/(g/L) | WBC/(×109/L) | NEU/(×109/L) | LYM/(×109/L) | |||||||||||
| 建模队列 | 83/91 | 82/92 | 5.51±2.09 | 39.40±4.16 | 4.32±0.51 | 115.51±18.54 | 6.75±1.60 | 4.19±1.23 | 2.05±0.98 | |||||||||||
| 验证队列 | 34/41 | 38/37 | 5.55±1.86 | 39.17±4.49 | 4.38±0.46 | 114.22±16.93 | 6.74±1.63 | 4.27±1.16 | 2.07±0.94 | |||||||||||
| t | 0.118 | 0.263 | 0.126 | 0.393 | 0.886 | 0.515 | 0.053 | 0.445 | 0.219 | |||||||||||
| 组别 | n | 性别 (男/女) | 年龄/ 岁 | BMI/(kg/m2) | 呼吸系统 疾病(有/无) | 基础疾病 (有/无) | 衰弱 评分/分 | 术侧a | 手术 时间/min | 麻醉 时间/min | 术中 出血量/mL | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非PND组 | 112 | 43/69 | 62.38±5.33 | 23.89±2.39 | 32/80 | 33/79 | 2.18±0.63 | 58/54 | 110.84±26.57 | 127.55±25.76 | 208.33±26.45 | ||||||||
| PND组 | 62 | 21/41 | 63.27±6.82 | 24.52±2.76 | 11/51 | 24/38 | 2.85±0.81 | 27/35 | 114.86±27.50 | 133.24±28.45 | 204.52±22.74 | ||||||||
| χ2或t | 0.351 | 0.953 | 1.571 | 2.516 | 1.549 | 6.087** | 1.084 | 0.944 | 1.346 | 0.953 | |||||||||
| 组别 | 麻醉方式b | 镇痛方案c | VAS评分/分 | ALB/(g/L) | RBC/(×1012/L) | HB/(g/L) | WBC/(×109/L) | NEU/(×109/L) | LYM/(×109/L) | ||||||||||
| 非PND组 | 44/68 | 45/67 | 5.16±1.84 | 40.65±3.84 | 4.27±0.49 | 118.09±17.99 | 6.71±1.54 | 4.20±1.23 | 1.99±0.89 | ||||||||||
| PND组 | 39/23 | 37/25 | 6.15±2.38 | 37.15±3.77 | 4.41±0.54 | 110.84±18.76 | 6.82±1.70 | 4.18±1.25 | 2.16±1.13 | ||||||||||
| χ2或t | 8.923** | 6.089* | 3.080* | 5.798** | 1.761 | 2.505* | 0.469 | 0.055 | 1.092 | ||||||||||
表2 建模队列PND组和非PND组一般资料对比
Tab.2 Comparison of general data between the PDN group and the non-PND group in modeling queue
| 组别 | n | 性别 (男/女) | 年龄/ 岁 | BMI/(kg/m2) | 呼吸系统 疾病(有/无) | 基础疾病 (有/无) | 衰弱 评分/分 | 术侧a | 手术 时间/min | 麻醉 时间/min | 术中 出血量/mL | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非PND组 | 112 | 43/69 | 62.38±5.33 | 23.89±2.39 | 32/80 | 33/79 | 2.18±0.63 | 58/54 | 110.84±26.57 | 127.55±25.76 | 208.33±26.45 | ||||||||
| PND组 | 62 | 21/41 | 63.27±6.82 | 24.52±2.76 | 11/51 | 24/38 | 2.85±0.81 | 27/35 | 114.86±27.50 | 133.24±28.45 | 204.52±22.74 | ||||||||
| χ2或t | 0.351 | 0.953 | 1.571 | 2.516 | 1.549 | 6.087** | 1.084 | 0.944 | 1.346 | 0.953 | |||||||||
| 组别 | 麻醉方式b | 镇痛方案c | VAS评分/分 | ALB/(g/L) | RBC/(×1012/L) | HB/(g/L) | WBC/(×109/L) | NEU/(×109/L) | LYM/(×109/L) | ||||||||||
| 非PND组 | 44/68 | 45/67 | 5.16±1.84 | 40.65±3.84 | 4.27±0.49 | 118.09±17.99 | 6.71±1.54 | 4.20±1.23 | 1.99±0.89 | ||||||||||
| PND组 | 39/23 | 37/25 | 6.15±2.38 | 37.15±3.77 | 4.41±0.54 | 110.84±18.76 | 6.82±1.70 | 4.18±1.25 | 2.16±1.13 | ||||||||||
| χ2或t | 8.923** | 6.089* | 3.080* | 5.798** | 1.761 | 2.505* | 0.469 | 0.055 | 1.092 | ||||||||||
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| 衰弱评分 | 1.322 | 0.314 | 17.743 | <0.001 | 3.752 (2.028~6.943) |
| 麻醉方式 | 1.082 | 0.425 | 6.474 | 0.011 | 2.949 (1.282~6.785) |
| 镇痛方案 | 1.092 | 0.442 | 6.109 | 0.013 | 2.980 (1.254~7.083) |
| VAS评分 | 0.262 | 0.101 | 6.723 | 0.010 | 1.300 (1.066~1.584) |
| ALB | -0.214 | 0.057 | 13.941 | <0.001 | 0.807 (0.721~0.903) |
| HB | -0.036 | 0.012 | 8.491 | 0.004 | 0.964 (0.941~0.988) |
| 常数项 | 5.961 | 2.694 | 4.897 | 0.027 | 388.178 |
表3 多因素回归分析TKA患者发生PND的影响因素
Tab.3 Multivariate regression analysis of influencing factors of PND in TKA patients
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| 衰弱评分 | 1.322 | 0.314 | 17.743 | <0.001 | 3.752 (2.028~6.943) |
| 麻醉方式 | 1.082 | 0.425 | 6.474 | 0.011 | 2.949 (1.282~6.785) |
| 镇痛方案 | 1.092 | 0.442 | 6.109 | 0.013 | 2.980 (1.254~7.083) |
| VAS评分 | 0.262 | 0.101 | 6.723 | 0.010 | 1.300 (1.066~1.584) |
| ALB | -0.214 | 0.057 | 13.941 | <0.001 | 0.807 (0.721~0.903) |
| HB | -0.036 | 0.012 | 8.491 | 0.004 | 0.964 (0.941~0.988) |
| 常数项 | 5.961 | 2.694 | 4.897 | 0.027 | 388.178 |
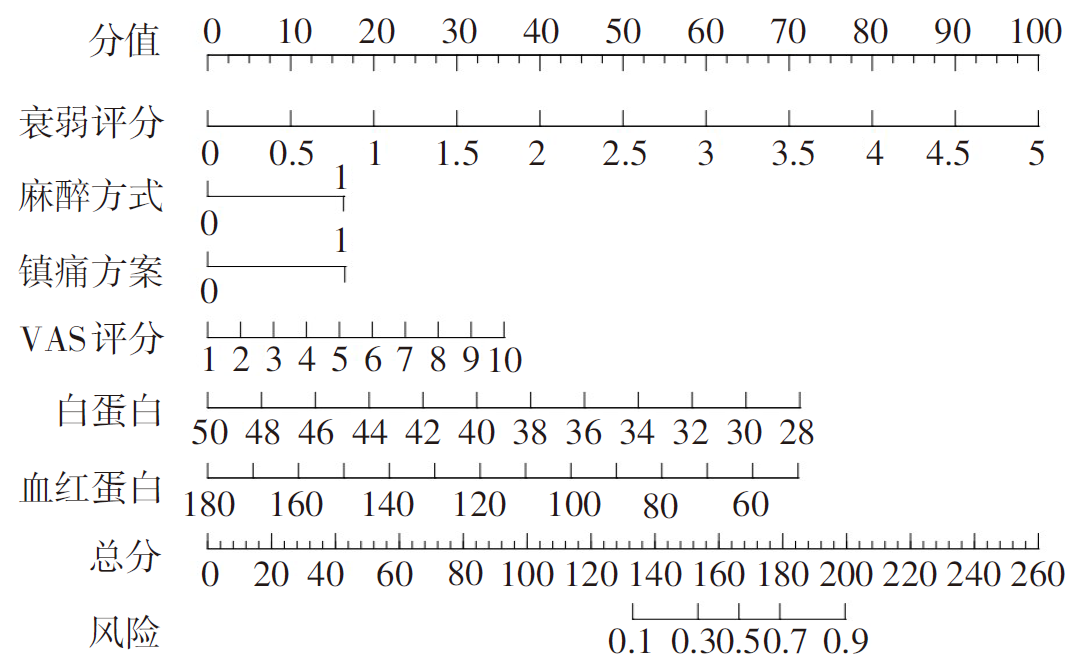
图1 预测TKA患者发生PND的列线图模型
Fig.1 Linechart model for predicting PND in TKA patients
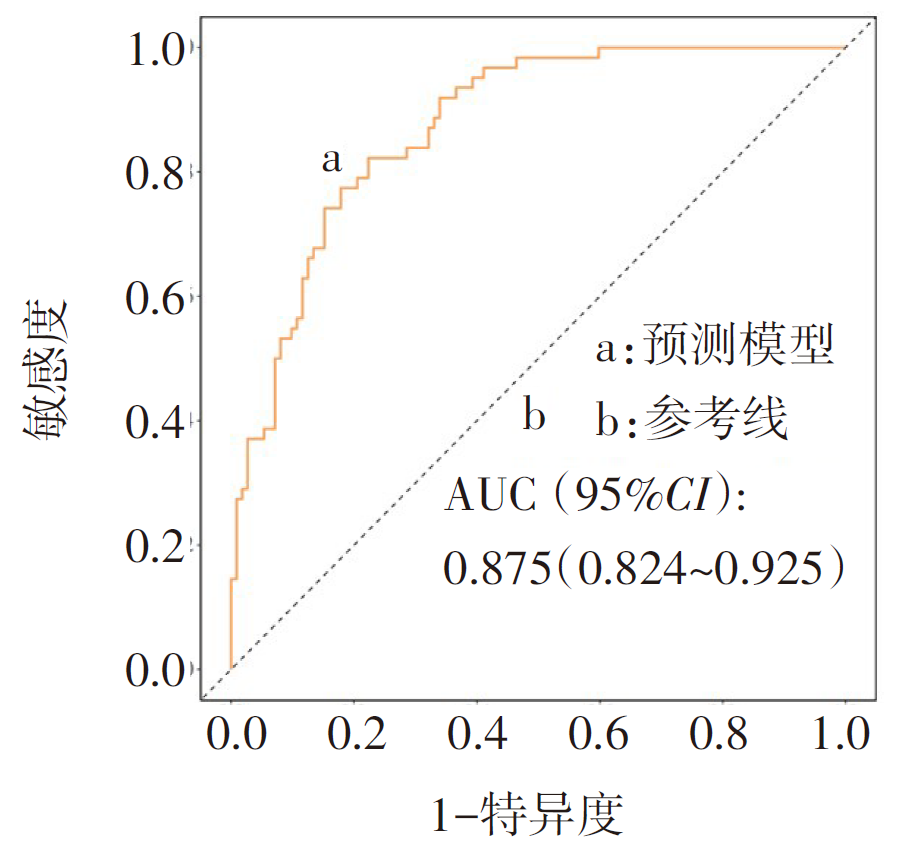
图2 建模队列ROC曲线
Fig.2 Modeling the ROC curve of the queue
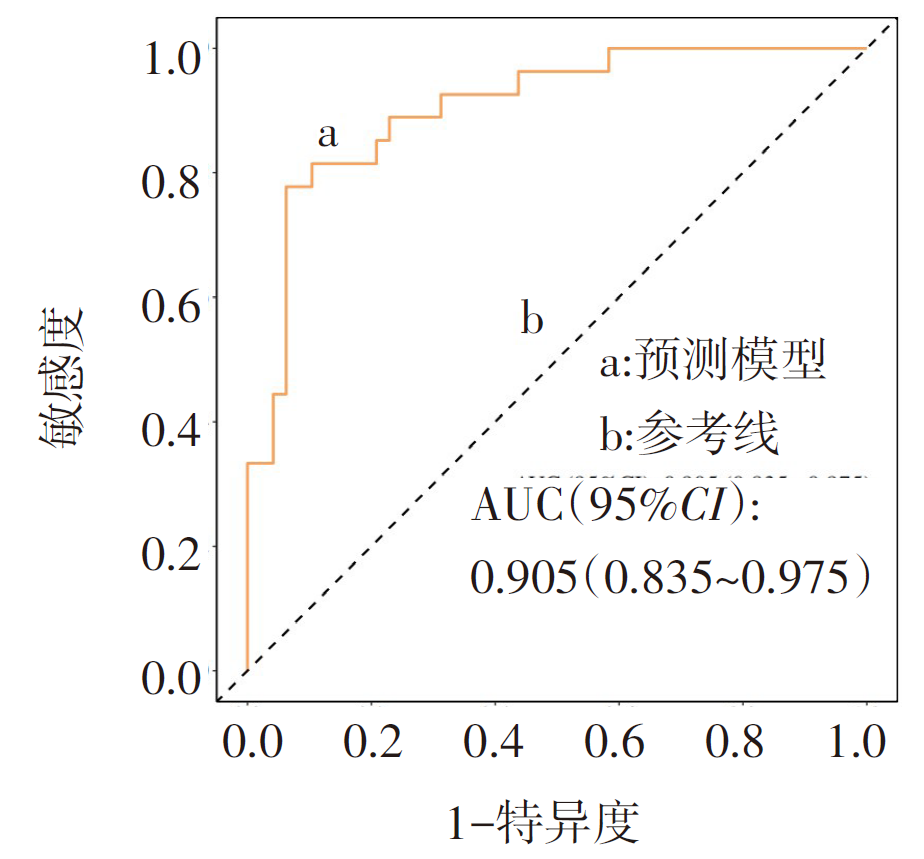
图3 验证队列ROC曲线
Fig.3 Verifying the ROC curve of the queue
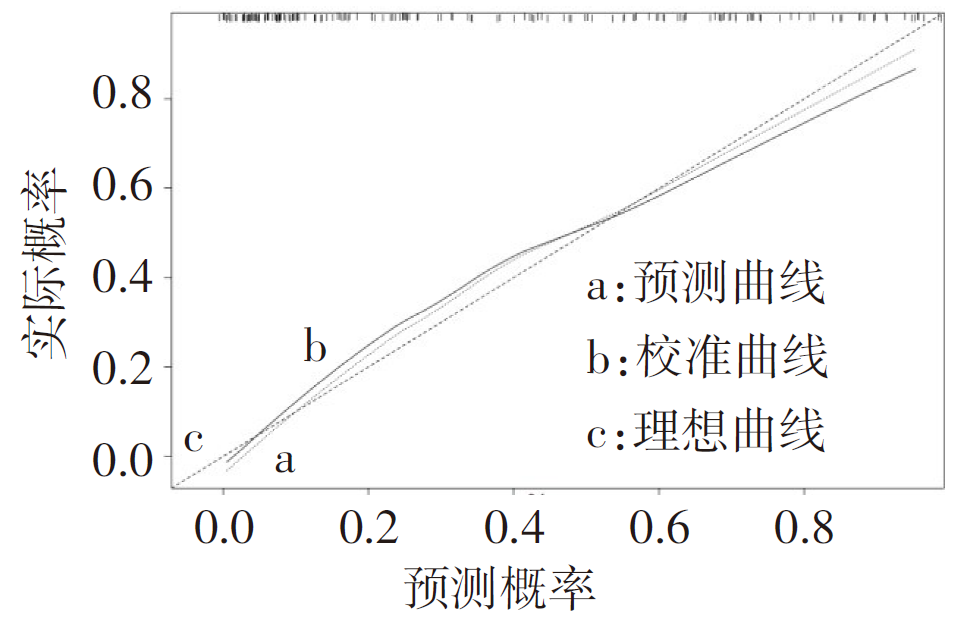
图4 建模队列校准曲线
Fig.4 Modeling the queue calibration curve
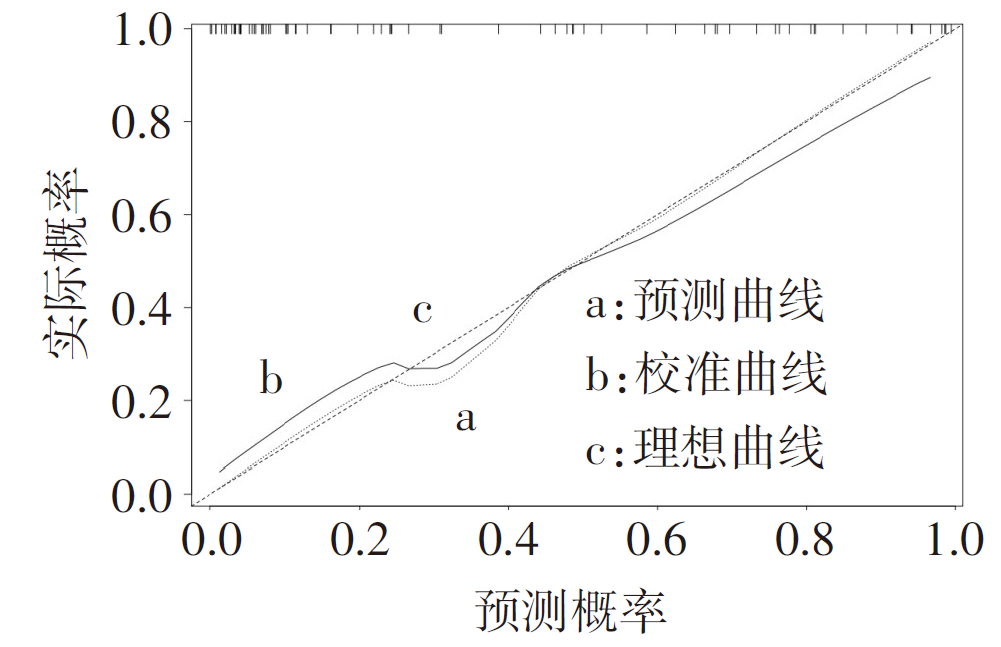
图5 验证队列校准曲线
Fig.5 Verifying the queue calibration curve
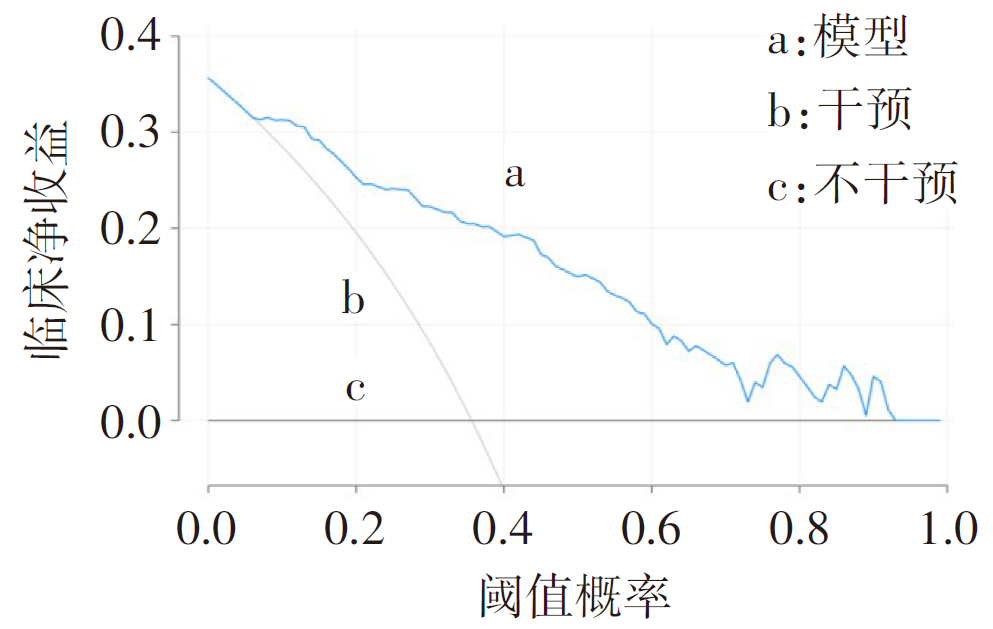
图6 建模队列决策分析曲线
Fig.6 Modeling queue decision analysis curve
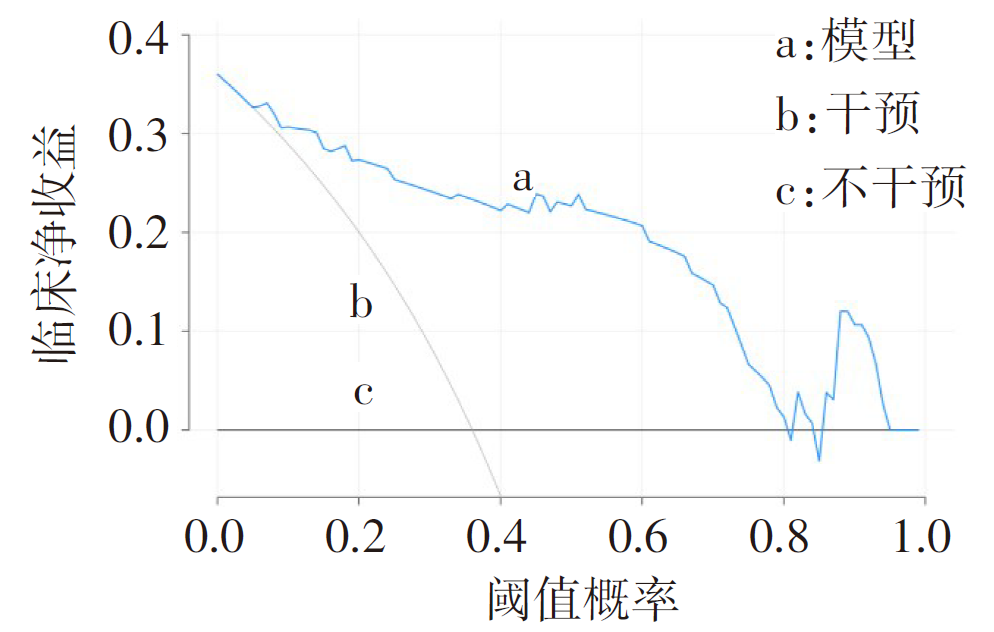
图7 验证队列决策分析曲线
Fig.7 Verifying queue decision analysis curve
| [1] | CUI A, LI H, WANG D, et al. Global,regional prevalence,incidence and risk factors of knee osteoarthritis in population-based studies[J]. EClinicalMedicine, 2020,29-30:100587. doi:10.1016/j.eclinm.2020.100587. |
| [2] | SAFFARINI M, HIRSCHMANN M T, BONNIN M. Personalisation and customisation in total knee arthroplasty:the paradox of custom knee implants[J]. Knee Surg Sports Traumatol Arthrosc, 2023, 31(4):1193-1195. doi:10.1007/s00167-023-07385-0. |
| [3] | LIU S, XV L, WU X, et al. Potential value of preoperative fasting blood glucose levels in the identification of postoperative delirium in non-diabetic older patients undergoing total hip replacement:the perioperative neurocognitive disorder and biomarker lifestyle study[J]. Front Psychiatry, 2022, 13:941048. doi:10.3389/fpsyt.2022.941048. |
| [4] | 申远. 麻醉与围手术期神经认知功能障碍[J]. 老年医学与保健, 2023, 29(4):669-673. |
| SHEN Y. Neurocognitive dysfunction during anesthesia and perioperative period[J]. Geriatrics and Health Care, 2023, 29(4):669-673. doi:10.3969/j.issn.1008-8296.2023.04.003. | |
| [5] | 刘健慧, 胡佳勇, 杜雪. 围手术期神经认知功能障碍的现状与未来[J]. 同济大学学报(医学版), 2020, 41(1):9-18. |
| LIU J H, HU J Y, DU X. Current situation and future of neurocognitive dysfunction in perioperative period[J]. Journal of Tongji University(Medical Edition), 2020, 41(1):9-18. doi:10.16118/j.1008-0392.2020.01.003. | |
| [6] | EVERED L, ATKINS K, SILBERT B, et al. Acute peri-operative neurocognitive disorders:a narrative review[J]. Anaesthesia, 2022,77 Suppl 1:34-42. doi:10.1111/anae.15613. |
| [7] | KITSIS P, ZISIMOU T, GKIATAS I, et al. Postoperative delirium and postoperative cognitive dysfunction in patients with elective hip or knee arthroplasty:a narrative review of the literature[J]. Life(Basel), 2022, 12(2):314. doi:10.3390/life12020314. |
| [8] | HORVATH B, KLOESEL B, TODD M M, et al. The evolution,current value,and future of the American Society of Anesthesiologists Physical Status Classification System[J]. Anesthesiology, 2021, 135(5):904-919. doi: 10.1097/ALN.0000000000003947. |
| [9] | JIA X, WANG Z, HUANG F, et al. A comparison of the Mini-Mental State Examination (MMSE) with the Montreal Cognitive Assessment (MoCA) for mild cognitive impairment screening in Chinese middle-aged and older population:a cross-sectional study[J]. BMC Psychiatry, 2021, 21(1):485. doi:10.1186/s12888-021-03495-6. |
| [10] | DEVI J. The scales of functional assessment of Activities of Daily Living in geriatrics[J]. Age Ageing, 2018, 47(4):500-502. doi:10.1093/ageing/afy050. |
| [11] | 景冬梅, 沈冲, 莫永珍, 等. 中文版衰弱量表在老年衰弱评价中的信效度研究[J]. 护士进修杂志, 2021, 36(9):784-788. |
| JING D M, SHEN C, MO Y Z, et al. Study on the reliability and validity of Chinese version of asthenia scale in the evaluation of senile asthenia[J]. Journal of Nurse Training, 2021, 36(9):784-788. doi:10.16821/j.cnki.hsjx.2021.09.004. | |
| [12] | 孙兵, 车晓明. 视觉模拟评分法(VAS)[J]. 中华神经外科杂志, 2012, 28(6):645. |
| SUN B, CHE X M. Visual analogue scale(VAS)[J]. Chinese Journal of Neurosurgery, 2012, 28(6):645. | |
| [13] | QEVA E, SOLLAZZO C, BILOTTA F. Insulin signaling in the central nervous system,a possible pathophysiological mechanism of anesthesia-induced delayed neurocognitive recovery/postoperative neurocognitive disorder:a narrative review[J]. Expert Rev Neurother, 2022, 22(10):839-847. doi:10.1080/14737175.2022.2144234. |
| [14] | YUAN Y, PENG C, BURR J A, et al. Frailty,cognitive impairment,and depressive symptoms in Chinese older adults:an eight-year multi-trajectory analysis[J]. BMC Geriatr, 2023, 23(1):843. doi:10.1186/s12877-023-04554-1. |
| [15] | GRACIE T J, CAUFIELD-NOLL C, WANG N Y, et al. The association of preoperative frailty and postoperative delirium:a meta-analysis[J]. Anesth Analg, 2021, 133(2):314-323. doi:10.1213/ANE.0000000000005609. |
| [16] | WARD D D, RANSON J M, WALLACE L, et al. Frailty,lifestyle,genetics and dementia risk[J]. J Neurol Neurosurg Psychiatry, 2022, 93(4):343-350. doi:10.1136/jnnp-2021-327396. |
| [17] | GRICOURT Y, CUVILLON P. Epidural analgesia combined with general anaesthesia to prevent cognitive dysfunction:more than a single strategy?[J]. Anaesth Crit Care Pain Med, 2022, 41(5):101136. doi:10.1016/j.accpm.2022.101136. |
| [18] | 靳洪震, 王岩, 柏豪豪, 等. 全膝关节置换术治疗膝骨关节炎围手术期研究进展[J]. 中国中西医结合外科杂志, 2024, 30(1):144-149. |
| JIN H Z, WANG Y, BO H H, et al. Research progress of total knee arthroplasty for knee osteoarthritis in perioperative period[J]. Chinese Journal of Surgery of Integrated Traditional and Western Medicine, 2024, 30(1):144-149. doi:10.3969/j.issn.1007-6948.2024.01.029 | |
| [19] | KIM J W, BYUN M S, LEE J H, et al. Serum albumin and beta-amyloid deposition in the human brain[J]. Neurology, 2020, 95(7):e815-e826. doi:10.1212/WNL.0000000000010005. |
| [20] | KOMURCU O, DOST B, OZDEMIR E, et al. Red blood cell transfusion and hemoglobin level on neurological outcome in the first 24 hours of traumatic brain injury[J]. Am J Emerg Med, 2022, 59:74-78. doi:10.1016/j.ajem.2022.06.058. |
| [21] | WANG J, WANG C, LI X, et al. Association of anemia with cognitive function and dementia among older adults:the role of inflammation[J]. J Alzheimers Dis, 2023, 96(1):125-134. doi:10.3233/JAD-230483. |
| [22] | SUN S, WEN Y, LI Y. Serum albumin,cognitive function,motor impairment,and survival prognosis in Parkinson disease[J]. Medicine (Baltimore), 2022, 101(37):e30324. doi:10.1097/MD.0000000000030324. |
| [23] | RONG X, DING Z C, YU H D, et al. Risk factors of postoperative delirium in the knee and hip replacement patients:a systematic review and meta-analysis[J]. J Orthop Surg Res, 2021, 16(1):76. doi:10.1186/s13018-020-02127-1. |
| [1] | 李斌, 谭振刚, 张华清. 基于息肉特征和血清学指标构建结直肠息肉复发风险预测模型及效能分析[J]. 天津医药, 2026, 54(3): 249-253. |
| [2] | 朱海燕, 王烨, 尹艳. 老年NSCLC患者术后胃肠功能紊乱的危险因素研究[J]. 天津医药, 2026, 54(3): 289-294. |
| [3] | 刘晓华, 韩婷婷, 高玉杰. 增强CT淋巴结边缘特征联合IPI对难治性弥漫大B细胞巴瘤的预测价值[J]. 天津医药, 2026, 54(3): 303-308. |
| [4] | 陈丽, 陈楠. COPD进展为Ⅱ型呼吸衰竭预警模型的建立与验证[J]. 天津医药, 2026, 54(2): 189-195. |
| [5] | 楚兴, 刘磊, 杨华, 陈宏. 胆总管结石并发急性胆源性胰腺炎的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 35-40. |
| [6] | 程云, 夏明农, 张帆, 李凤. 小儿热性惊厥发展为癫痫的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 52-57. |
| [7] | 陈敏, 夏莉, 朱荣媛, 王欣雨, 季骏. 拔除第一前磨牙正畸治疗后牙龈内陷的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 57-63. |
| [8] | 李贺, 马胜山, 孙阳, 武栋泽, 李小飞. 关节镜肩袖修补术后再撕裂风险的影响因素及预测模型构建[J]. 天津医药, 2026, 54(1): 64-69. |
| [9] | 蔡淼, 梁爽, 刘洋. 儿童肺炎住院时间延长预测模型的构建及临床应用价值[J]. 天津医药, 2025, 53(9): 976-980. |
| [10] | 刘志远, 杨声飞, 钱释然, 邓忆莲, 黎东伟, 李君久. 胸乳入路腔镜甲状腺术后早期低钙血症的危险因素分析及预测模型构建[J]. 天津医药, 2025, 53(8): 826-830. |
| [11] | 刘鹏勇, 刘梦友, 周昱, 管海, 田振, 胡浩, 岳晓松, 关倩楠. 甲状腺全切术后并发永久性甲状旁腺功能减退的危险因素及列线图建立[J]. 天津医药, 2025, 53(8): 850-855. |
| [12] | 金吴娟, 倪刚, 黄欣宇, 王羊洋. 老年消化道出血患者不良预后的列线图预测模型的构建与验证[J]. 天津医药, 2025, 53(7): 694-699. |
| [13] | 陈英, 郭长英, 张静, 李娟, 陈丰毅. 基于术前肺动脉压评估心脏移植术后右心衰竭的发生风险[J]. 天津医药, 2025, 53(7): 751-755. |
| [14] | 李婉婷, 刘弘扬, 桑婧, 阮育凤, 徐丽, 李冬梅. 老年下肢骨折患者术后发生急性心脑血管意外的影响因素分析[J]. 天津医药, 2025, 53(6): 648-653. |
| [15] | 王欣欣, 许慧, 吴晓. 妊娠期肝内胆汁淤积症合并GDM孕妇不良妊娠结局的影响因素及预测模型构建[J]. 天津医药, 2025, 53(5): 503-508. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||