天津医药 ›› 2024, Vol. 52 ›› Issue (3): 306-310.doi: 10.11958/20231021
张丽冉( ), 赵延华△()
), 赵延华△()
收稿日期:2023-07-09
修回日期:2023-10-10
出版日期:2024-03-15
发布日期:2024-03-13
通讯作者:
△E-mail:作者简介:张丽冉(1998),女,硕士在读,主要从事子痫前期预测及发病机制方面研究。E-mail:基金资助:
ZHANG Liran(), ZHAO Yanhua△()
Received:2023-07-09
Revised:2023-10-10
Published:2024-03-15
Online:2024-03-13
Contact:
△E-mail: 张丽冉, 赵延华. MP妊高征监测系统联合PLGF和PI对子痫前期的预测价值[J]. 天津医药, 2024, 52(3): 306-310.
ZHANG Liran, ZHAO Yanhua. The predictive value of MP hypertension monitoring system combined with PLGF and PI for preeclampsia[J]. Tianjin Medical Journal, 2024, 52(3): 306-310.
摘要:
目的 通过妊娠高血压综合征监测系统测定妊高征风险评级和胎盘生长因子(PLGF)水平,以及胎儿颈项透明层厚度(NT)检查时测得的子宫动脉搏动指数(PI)的联合应用,建立对子痫前期的临床预测模型。方法 选择子痫前期患者24例作为病例组,随机抽取同期有良好妊娠结局的孕妇95例作为对照组,收集2组在孕11~14周免疫荧光定量检测法测定的血清PLGF水平,子宫动脉PI,孕11~20周MP妊高征监测系统风险评级(MP风险)及其他相关数据,记录产前体质量指数(BMI)、年龄、孕次、分娩方式、新生儿出生体质量及Apgar评分。结果 单因素Logistic回归分析结果显示,BMI、年龄、PI、MP风险、PLGF是出现不良结局的影响因素。多因素回归分析结果显示高PI、MP中高风险和PLGF<12是影响出现不良结局的独立危险因素,建立的PE预测模型为logit(P)=-15.767+0.020×PI+0.072×MP风险+0.181×PLGF,ROC曲线下面积(AUC)为0.883,特异度为0.816,敏感度为0.846。结论 联合PI、MP风险、PLGF建立子痫前期临床预测模型具有一定的价值,且其联合预测价值高于单独应用。
中图分类号:
| 组别 | n | BMI/(kg/m2) | 年龄/岁 | 孕次/次 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 95 | 24.65(22.46,27.12) | 31.00(29.50,34.00) | 2(1,3) | |||||||
| 病例组 | 24 | 25.93(24.20,27.85) | 34.00(31.00,37.00) | 3(1,4) | |||||||
| Z | 2.102* | 3.184** | 1.743 | ||||||||
| 组别 | 外周阻力/PRU | 血液黏度/CP | 左RI | ||||||||
| 对照组 | 4.50(3.93,4.85) | 1.07(0.76,1.59) | 0.78(0.72,0.82) | ||||||||
| 病例组 | 4.57(4.22,4.78) | 1.25(0.96,1.82) | 0.78(0.74,0.84) | ||||||||
| Z | 1.712 | 0.825 | 0.735 | ||||||||
| 组别 | 左S/D | 右RI | |||||||||
| 对照组 | 4.60(3.60,5.70) | 0.77(0.73,0.83) | |||||||||
| 病例组 | 4.60(3.80,6.35) | 0.79(0.71,0.85) | |||||||||
| Z | 0.617 | 0.701 | |||||||||
| 组别 | 右S/D | PI | |||||||||
| 对照组 | 4.30(3.70,5.90) | 1.80±0.42 | |||||||||
| 病例组 | 4.65(3.40,6.73) | 2.18±0.51 | |||||||||
| Z或t | 0.779 | 4.764* | |||||||||
表1 2组基本情况比较
Tab.1 Comparison of basic information between the case group and the control group
| 组别 | n | BMI/(kg/m2) | 年龄/岁 | 孕次/次 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 95 | 24.65(22.46,27.12) | 31.00(29.50,34.00) | 2(1,3) | |||||||
| 病例组 | 24 | 25.93(24.20,27.85) | 34.00(31.00,37.00) | 3(1,4) | |||||||
| Z | 2.102* | 3.184** | 1.743 | ||||||||
| 组别 | 外周阻力/PRU | 血液黏度/CP | 左RI | ||||||||
| 对照组 | 4.50(3.93,4.85) | 1.07(0.76,1.59) | 0.78(0.72,0.82) | ||||||||
| 病例组 | 4.57(4.22,4.78) | 1.25(0.96,1.82) | 0.78(0.74,0.84) | ||||||||
| Z | 1.712 | 0.825 | 0.735 | ||||||||
| 组别 | 左S/D | 右RI | |||||||||
| 对照组 | 4.60(3.60,5.70) | 0.77(0.73,0.83) | |||||||||
| 病例组 | 4.60(3.80,6.35) | 0.79(0.71,0.85) | |||||||||
| Z | 0.617 | 0.701 | |||||||||
| 组别 | 右S/D | PI | |||||||||
| 对照组 | 4.30(3.70,5.90) | 1.80±0.42 | |||||||||
| 病例组 | 4.65(3.40,6.73) | 2.18±0.51 | |||||||||
| Z或t | 0.779 | 4.764* | |||||||||
| 组别 | n | PLGF(ng/L) | MP风险 | ||
|---|---|---|---|---|---|
| <12 | ≥12 | 低风险 | 中高风险 | ||
| 对照组 | 95 | 11(11.6) | 84(88.4) | 72(75.8) | 23(24.2) |
| 病例组 | 24 | 15(52.5) | 9(37.5) | 13(54.2) | 11(45.8) |
| χ2 | 9.207** | 4.389* | |||
表2 2组检查指标比较 例(%)
Tab.2 Comparison of examination indicators between the case group and the control group
| 组别 | n | PLGF(ng/L) | MP风险 | ||
|---|---|---|---|---|---|
| <12 | ≥12 | 低风险 | 中高风险 | ||
| 对照组 | 95 | 11(11.6) | 84(88.4) | 72(75.8) | 23(24.2) |
| 病例组 | 24 | 15(52.5) | 9(37.5) | 13(54.2) | 11(45.8) |
| χ2 | 9.207** | 4.389* | |||
| 组别 | n | 分娩方式 | 新生儿出生体质量/g | ||||
|---|---|---|---|---|---|---|---|
| 顺产 | 剖宫产 | ||||||
| 对照组 | 95 | 40(42.1) | 55(57.9) | 3 192.78±468.38 | |||
| 病例组 | 24 | 1(4.2) | 23(95.8) | 2 194.76±848.12 | |||
| χ2、Z或t' | 12.211** | 7.765** | |||||
| 组别 | Apgar评分/分 | ||||||
| 1 min | 5 min | 10 min | |||||
| 对照组 | 10.0(10.0,10.0) | 10.0(10.0,10.0) | 10.0(10.0,10.0) | ||||
| 病例组 | 10.0(8.0,10.0) | 10.0(9.0,10.0) | 10.0(10.0,10.0) | ||||
| χ2、Z或t' | 3.939** | 3.553** | 4.030** | ||||
表3 2组预后相关指标比较
Tab.3 Comparison of prognostic indicators between the case group and the control group
| 组别 | n | 分娩方式 | 新生儿出生体质量/g | ||||
|---|---|---|---|---|---|---|---|
| 顺产 | 剖宫产 | ||||||
| 对照组 | 95 | 40(42.1) | 55(57.9) | 3 192.78±468.38 | |||
| 病例组 | 24 | 1(4.2) | 23(95.8) | 2 194.76±848.12 | |||
| χ2、Z或t' | 12.211** | 7.765** | |||||
| 组别 | Apgar评分/分 | ||||||
| 1 min | 5 min | 10 min | |||||
| 对照组 | 10.0(10.0,10.0) | 10.0(10.0,10.0) | 10.0(10.0,10.0) | ||||
| 病例组 | 10.0(8.0,10.0) | 10.0(9.0,10.0) | 10.0(10.0,10.0) | ||||
| χ2、Z或t' | 3.939** | 3.553** | 4.030** | ||||
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| BMI | 0.136 | 0.065 | 4.378 | 0.036 | 1.145(1.009~1.301) |
| 年龄 | 0.175 | 0.056 | 9.766 | 0.002 | 1.192(1.068~1.330) |
| 血液黏度 | 0.336 | 0.311 | 1.167 | 0.280 | 1.399(0.760~2.574) |
| 外周阻力 | 0.435 | 0.355 | 1.501 | 0.220 | 1.545(0.770~3.098) |
| 左RI | 0.992 | 2.229 | 0.198 | 0.656 | 2.698(0.034~213.143) |
| 左SD | 0.043 | 0.101 | 0.181 | 0.668 | 1.044(0.857~1.272) |
| 右RI | 1.006 | 2.069 | 0.236 | 0.625 | 2.734(0.047~157.780) |
| 右SD | 0.110 | 0.086 | 1.636 | 0.201 | 1.117(0.943~1.323) |
| PI | 1.964 | 0.463 | 17.994 | <0.001 | 7.115(2.872~17.630) |
| MP风险 | 1.106 | 0.327 | 11.440 | 0.001 | 3.021(1.591~5.737) |
| PLGF | 3.347 | 0.503 | 44.277 | <0.001 | 28.409(10.591~76.206) |
表4 影响PE发病的单因素Logistic回归分析
Tab.4 Single Logistic regression analysis of factor influencing the incidence of PE
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| BMI | 0.136 | 0.065 | 4.378 | 0.036 | 1.145(1.009~1.301) |
| 年龄 | 0.175 | 0.056 | 9.766 | 0.002 | 1.192(1.068~1.330) |
| 血液黏度 | 0.336 | 0.311 | 1.167 | 0.280 | 1.399(0.760~2.574) |
| 外周阻力 | 0.435 | 0.355 | 1.501 | 0.220 | 1.545(0.770~3.098) |
| 左RI | 0.992 | 2.229 | 0.198 | 0.656 | 2.698(0.034~213.143) |
| 左SD | 0.043 | 0.101 | 0.181 | 0.668 | 1.044(0.857~1.272) |
| 右RI | 1.006 | 2.069 | 0.236 | 0.625 | 2.734(0.047~157.780) |
| 右SD | 0.110 | 0.086 | 1.636 | 0.201 | 1.117(0.943~1.323) |
| PI | 1.964 | 0.463 | 17.994 | <0.001 | 7.115(2.872~17.630) |
| MP风险 | 1.106 | 0.327 | 11.440 | 0.001 | 3.021(1.591~5.737) |
| PLGF | 3.347 | 0.503 | 44.277 | <0.001 | 28.409(10.591~76.206) |
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| 年龄 | 0.195 | 0.237 | 0.680 | 0.410 | 1.216(0.764~1.933) |
| BMI | 0.108 | 0.110 | 0.963 | 0.327 | 1.114(0.898~1.382) |
| PI | 0.020 | 0.009 | 4.998 | 0.025 | 1.020(1.002~1.038) |
| MP | 0.072 | 0.034 | 4.559 | 0.033 | 1.075(1.006~1.148) |
| PLGF | 0.181 | 0.078 | 5.364 | 0.021 | 1.198(1.028~1.396) |
| 常数项 | -15.767 | 5.673 | 7.725 | 0.005 | <0.001 |
表5 影响PE发病的多因素Logistic回归分析
Tab.5 Logistic regression of multiple factors influencing the incidence of PE
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| 年龄 | 0.195 | 0.237 | 0.680 | 0.410 | 1.216(0.764~1.933) |
| BMI | 0.108 | 0.110 | 0.963 | 0.327 | 1.114(0.898~1.382) |
| PI | 0.020 | 0.009 | 4.998 | 0.025 | 1.020(1.002~1.038) |
| MP | 0.072 | 0.034 | 4.559 | 0.033 | 1.075(1.006~1.148) |
| PLGF | 0.181 | 0.078 | 5.364 | 0.021 | 1.198(1.028~1.396) |
| 常数项 | -15.767 | 5.673 | 7.725 | 0.005 | <0.001 |
| 指标 | AUC(95%CI) | P | 特异度 | 敏感度 | 约登指数 |
|---|---|---|---|---|---|
| Logistic回归模型 | 0.883(0.787~0.978) | <0.001 | 0.816 | 0.846 | 0.662 |
| MP风险+PLGF | 0.797(0.661~0.934) | <0.001 | 0.640 | 0.846 | 0.486 |
| MP风险+PI | 0.777(0.626~0.929) | 0.001 | 0.763 | 0.769 | 0.532 |
| PLGF+PI | 0.836(0.681~0.991) | <0.001 | 0.965 | 0.769 | 0.734 |
| MP风险 | 0.684(0.530~0.838) | 0.030 | 0.675 | 0.692 | 0.367 |
| PLGF | 0.670(0.489~0.852) | 0.045 | 0.956 | 0.385 | 0.341 |
| PI | 0.693(0.507~0.879) | 0.023 | 0.965 | 0.462 | 0.427 |
表6 各相关因素及Logistic回归模型的预测效能
Tab.6 The predictive efficiency of Logistic regression model and relevant factors
| 指标 | AUC(95%CI) | P | 特异度 | 敏感度 | 约登指数 |
|---|---|---|---|---|---|
| Logistic回归模型 | 0.883(0.787~0.978) | <0.001 | 0.816 | 0.846 | 0.662 |
| MP风险+PLGF | 0.797(0.661~0.934) | <0.001 | 0.640 | 0.846 | 0.486 |
| MP风险+PI | 0.777(0.626~0.929) | 0.001 | 0.763 | 0.769 | 0.532 |
| PLGF+PI | 0.836(0.681~0.991) | <0.001 | 0.965 | 0.769 | 0.734 |
| MP风险 | 0.684(0.530~0.838) | 0.030 | 0.675 | 0.692 | 0.367 |
| PLGF | 0.670(0.489~0.852) | 0.045 | 0.956 | 0.385 | 0.341 |
| PI | 0.693(0.507~0.879) | 0.023 | 0.965 | 0.462 | 0.427 |
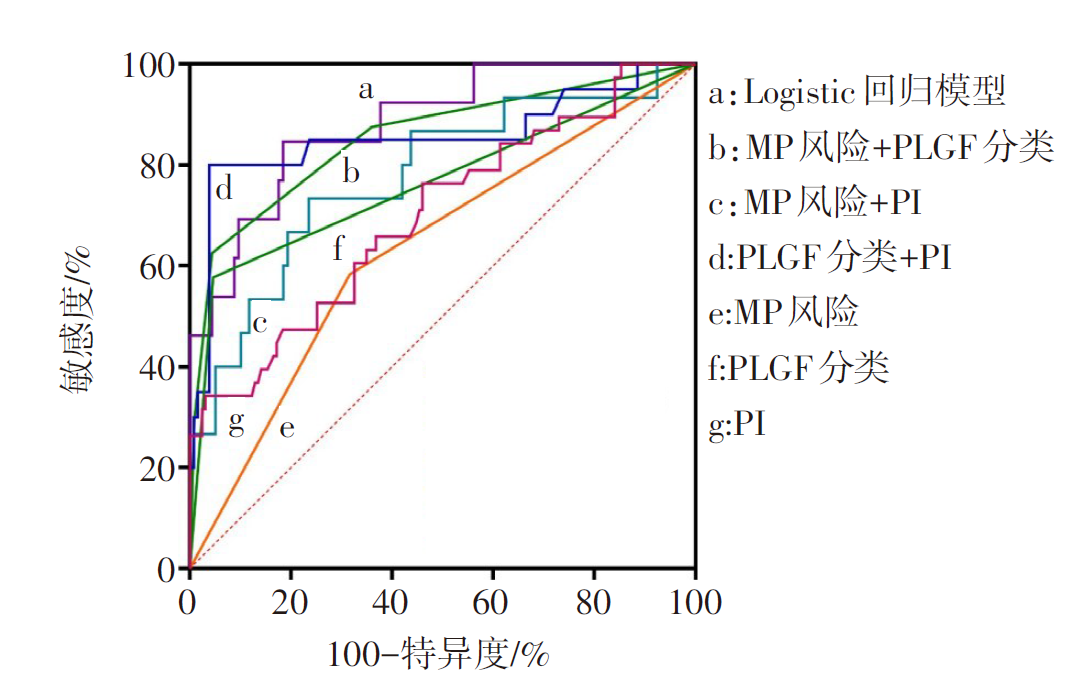
图1 孕妇发生PE风险的ROC曲线
Fig.1 ROC curve of risk of PE in pregnant women
| [1] | POON L C, SHENNAN A, HYETT J A, et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia:A pragmatic guide for first-trimester screening and prevention[J]. Int J Gynaecol Obstet, 2019, 145(Suppl 1):1-33. doi:10.1002/ijgo.12802. |
| [2] | KASSAN M, WECKER A, KADOWITZ P, et al. CD4+CD25+Foxp3 regulatory T cells and vascular dysfunction in hypertension[J]. J Hypertens, 2013, 31(10):1939-1943. doi:10.1097/HJH.0b013e328362feb7. |
| [3] | NEVERS T, KALKUNTE S, SHARMA S. Uterine regulatory T cells,IL-10 and hypertension[J]. Am J Reprod Immunol, 2011, 66(Suppl 1):88-92. doi:10.1111/j.1600-0897.2011.01040.x. |
| [4] | Matsubara K, Matsubara Y, Uchikura Y, et al. HMGAl is a potential driver of preeclampsia pathogenesis by interference with extravillous trophoblasts invasion[J]. Biomolecules, 2021, 11(6):822. doi:10.3390/biom11060822. |
| [5] | 岳巾晶, 曾莹, 郭晓珮, 等. miR-155通过调控PKG1影响滋养细胞生物学功能并参与子痫前期的机制探讨[J]. 天津医药, 2023, 51(9):928-934. |
| YUE J J, ZENG Y, GUO X P, et al. MiR-155 affects the biological functions of trophoblastic cells through regulating cGMP-dependent kinase 1 and is involved in the mechanism of preeclampsia[J]. Tianjin Med J, 2023, 51(9):928-934. doi:10.11958/20221869. | |
| [6] | 韩贞艳, 关红琼. 子痫前期患者的胎盘环状RNA表达谱及与病情的相关性[J]. 天津医药, 2023, 51(5):513-517. |
| HAN Z Y, GUAN H Q. The expression profile of circular RNA in placenta of patients with preeclampsia and its correlation with the patient’s condition[J]. Tianjin Med J, 2023, 51(5):513-517. doi:10.11958/20221313. | |
| [7] | 鲁超, 汪俊丽. 血清白蛋白、 前白蛋白、血红蛋白及尿液β2-微球蛋白对不同类型子痫前期的预测价值[J]. 临床与病理杂志, 2022, 42(6):1355-1362. |
| LU C, WANG J L. Predictive value of serum albumin,prealbumin,hemoglobin and urine β2-microglobulin in different types of preeclampsia[J]. International Journal of Pathology and Clinical Medicine, 2022, 42(6):1355-1362. doi:10.3978/j.issn.2095-6959.2022.06.014. | |
| [8] | 鲍瀛, 张凤美, 张蝶. 胎盘生长因子在临床疾病诊断中的研究进展[J]. 吉林医学, 2022, 43(4):1087-1089. |
| BAO Y, ZHANG F M, ZHANG D. Research progress of placental growth factor in clinical[J]. Jilin Medical Journal, 2022, 43(4):1087-1089. doi:10.3969/j.issn.1004-0412.2022.04.089. | |
| [9] | 陈佳, 郭静, 韩悦, 等. 联合检测妊娠早中期孕妇血清PAPP-A、PLGF及子宫动脉血流参数预测子痫前期的临床意义[J]. 解放军医药杂志, 2021, 33(2):60-64. |
| CHEN J, GUO J, HAN Y, et al. Clinical significance of combined detection of serum PAPP-A,PLGF and uterine artery blood flow parame-ters in pregnant women in early and mid-pregnancy in prediction of preeclampsia[J]. Medical & Pharmaceutical Journal of Chinese People's Liberation Army, 2021, 33(2):60-64. doi:10.3969/j.issn.2095-140X.2021.02.014. | |
| [10] | MACDOMNALD T M, WALKER S P, HANNAN N J, et al. Clinical tools and biomarkers to predict preeclampsia[J]. EBio Medicine, 2022, 75:103780. doi:10.1016/j.ebiom.2021.103780. |
| [11] | 沈新丽. 联合检测妊娠早中期孕妇血清β-hCG、PAPP-A、sFlt-1及PLGF对预测子痫前期的意义[J]. 中国妇幼保健, 2018, 33(15):3412-3415. |
| SHEN X L. Joint detection of serum from pregnant women in the early and middle stages of pregnancy β- The significance of hCG,PAPP-A,sFlt-1,and PLGF in predicting preeclampsia[J]. Maternal & Child Health Care of China, 2018, 33(15):3412-3415. doi:10.7620/zgfybj.j.issn.1001-4411.2018.15.16. | |
| [12] | CHAEMSAITHONG P, SAHOTA D S, POON L C. First trimester preeclampsia screening and prediction[J]. Am J Obstet Gynecol, 2022, 226(2S):S1071-S1097.e2. doi:10.1016/j.ajog.2020.07.020. |
| [13] | 褚翠雯, 陈爱萍, 李坤. 超声子宫动脉血流指标评估子痫前期孕妇母胎循环及与妊娠结局的相关性[J]. 中国计划生育学杂志, 2022, 30(7):1569-1573. |
| CHU C W, CHEN A P, LI K. Maternal and fetal circulation situation evaluated by the uterine artery blood flow indexes of ultrasonography and their cor-relation with the pregnancy outcomes[J]. Chinese Journal of Family Planning, 2022, 30(7):1569-1573. doi:10.3969/j.issn.1004-8189.2022.07.023. | |
| [14] | 蔡莉娜, 刘剑波, 吴树彪, 等. 可溶性血管内皮生长因子受体-1/胎盘生长因子与子宫动脉搏动指数联合预测子痫前期的临床价值研究[J]. 中国全科医学, 2018, 21(7):827-830. |
| CAI L N, LIU J B, WU S B, et al. Predicative value of sFlt-1/PLGF ratio and uterine artery pi for preeclampsia[J]. Chinese General Practice, 2018, 21(7):827-830. doi:10.3969/j.issn.1007-9572.2018.07.015. | |
| [15] | PEDROSO M A, PALMER K R, HODGES R J, et al. Uterine artery doppler in screening for preeclampsia and fetal growth restriction[J]. Rev Bras Ginecol Obstet, 2018, 40(5):287-293. doi:10.1055/s-0038-1660777. |
| [16] | 王勇, 李传刚. 微小RNA-18a联合子宫动脉血流参数对早发型子痫前期的预测价值[J]. 天津医药, 2021, 49(12):1311-1315. |
| WANG Y, LI C G. The predictive value of microRNA-18a combined with uterine artery blood flow parameters for early-onset preeclampsia[J]. Tianjin Med J, 2021, 49(12):1311-1315. | |
| [17] | 张秀丽, 何宏舸, 王伟伟, 等. MP妊高征监测系统在妊娠期高血压疾病预测及预防中的应用价值[J]. 临床医学, 2022, 42(4):15-17. |
| ZHANG X L, HE H G, WANG W W, et al. Clinical application of MP pregnancy induced hypertension monitoring system in prediction and prevention of pregnancy induced hypertension[J]. Clinical Medicine, 2022, 42(4):15-17. doi:10.19528/j.issn.1003-3548.2022.04.005. | |
| [18] | REDMAN C W G. The six stages of pre-eclampsia[J]. Pregnancy Hypertens, 2014, 4:246. doi:10.1016/j.preghy.2014.04.020. |
| [19] | AVORGBEDOR F, SILVA S, MCCOY T P, et al. Hypertension and infant outcomes: North Carolina pregnancy risks assessment monitoring system data[J]. Pregnancy Hypertens, 2022, 28:189-193. doi:10.1016/j.preghy.2022.05.004. |
| [20] | 李晶, 范卓然, 张俊农, 等. 早产型子痫前期及慢性高血压并发子痫前期患者的临床特征及TyG指数对比研究[J]. 天津医药, 2023, 51(2):190-193. |
| LI J, FAN Z R, ZHANG J N, et al. Comparative study on clinical characteristics and TyG index in patients with premature preeclampsia and chronic hypertension complicated with preeclampsia[J]. Tianjin Med J, 2023, 51(2):190-193. doi:10.11958/20220717. | |
| [21] | 任玉洁. 血清PLGF、SFLT-1、MAP及UAPI对预测子痫前期的临床应用价值[J]. 现代诊断与治疗, 2022, 33(3):320-323. |
| REN Y J. Clinical Application value of serum PLGF,SFLT-1,MAP and UAPI in predicting preeclampsia[J]. Modern Diagnosis & Treatment, 2022, 33(3):320-323. | |
| [22] | 孙文静, 胡孟彩, 崔世红, 等. 妊娠相关血浆蛋白A、胎盘生长因子联合胆红素对子痫前期的预测价值[J]. 中外医学研究, 2021, 19(4):74-77. |
| SUN W J, HU M C, CUI S H, et al. Predictive value of PAPP-A,PLGF and bilirubin in preeclampsia[J]. Chinese and Foreign Medical Research, 2021, 19(4):74-77. doi:10.14033/j.cnki.cfmr.2021.04.025. | |
| [23] | 杨冬梅. 胎盘生长因子在早期妊娠中的研究进展[J]. 天津医科大学学报, 2022, 28(3):339-342. |
| YANG D M. Research progress on placental growth factor in early pregnancy[J]. Journal of Tianjin Medical University, 2022, 28(3):339-342. | |
| [24] | 刘景雁, 郭永华, 肖保军, 等. 孕早期子宫动脉测量预测孕中晚期妊娠期高血压价值[J]. 中国计划生育学杂志, 2022, 30(6):1357-1359,1364. |
| LIU J Y, GUO Y H, XIAO B J, et al. Value of uterine artery measurement of pregnant women during the first trimester of pregnancy for predicting their gesta-tional hypertension occurrence during the second and third trimester of pregnancy[J]. Chinese Journal of Family Planning, 2022, 30(6):1357-1359,1364. doi:10.3969/j.issn.1004-8189.2022.06.031. | |
| [25] | VELAUTHAR L, PLANA M N, KALIDINDI M, et al. First trimester uterine artery Doppler and adverse pregnancy outcome:a meta-analysis involving 55,974 women[J]. Ultrasound Obstet Gynecol, 2014, 43(5):500-507. doi:10.1002/uog.13275. |
| [26] | 宋岚, 尤佳. 动态血压监测联合妊高征预测系统在妊娠期高血压疾病管理中的应用效果[J]. 临床医学研究与实践, 2019, 4(7):123-124. |
| SONG L, YOU J. Application effect of ambulatory blood pressure monitoring combined with pregnancy induced hypertension prediction system in the management of pregnancy induced hypertension[J]. Clinical Research and Practice, 2019, 4(7):123-124. doi:10.19347/j.cnki.2096-1413.201907051. | |
| [27] | 朱爱玲, 张东红, 王俊霞. MP妊娠高血压综合征监测系统13200例临床观察[J]. 实用医学杂志, 2013, 29(20):3358-3360. |
| ZHU A L, ZHANG D H, WANG J X. Clinical observation on 13200 cases of MP pregnancy induced hypertension syndrome monitoring system[J]. The Journal of Practical Medicine, 2013, 29(20):3358-3360. doi:10.3969/j.issn.1006-5725.2013.20.035. |
| [1] | 陈丽, 陈楠. COPD进展为Ⅱ型呼吸衰竭预警模型的建立与验证[J]. 天津医药, 2026, 54(2): 189-195. |
| [2] | 程云, 夏明农, 张帆, 李凤. 小儿热性惊厥发展为癫痫的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 52-57. |
| [3] | 蔡淼, 梁爽, 刘洋. 儿童肺炎住院时间延长预测模型的构建及临床应用价值[J]. 天津医药, 2025, 53(9): 976-980. |
| [4] | 贾薇, 田志. Furin启动子甲基化水平与社区非糖尿病人群血压的相关性[J]. 天津医药, 2025, 53(9): 987-992. |
| [5] | 金吴娟, 倪刚, 黄欣宇, 王羊洋. 老年消化道出血患者不良预后的列线图预测模型的构建与验证[J]. 天津医药, 2025, 53(7): 694-699. |
| [6] | 陈英, 郭长英, 张静, 李娟, 陈丰毅. 基于术前肺动脉压评估心脏移植术后右心衰竭的发生风险[J]. 天津医药, 2025, 53(7): 751-755. |
| [7] | 吴宾, 杨自更, 金玲, 张婧, 韦红梅, 蔡冰冰, 魏玉英. miRNA-381-3p/MuRF1轴对低氧性肺动脉高压小鼠心肺损伤的影响[J]. 天津医药, 2025, 53(6): 571-577. |
| [8] | 李建林, 孙思进, 王大力. Ⅰ—Ⅱ期非小细胞肺癌胸腔镜术后心肺并发症的影响因素及预测模型构建[J]. 天津医药, 2025, 53(6): 583-588. |
| [9] | 高岩, 马伟, 张瑜, 李蕾. 艾司氯胺酮对小儿四肢骨折术后辅助镇痛效果及预测模型构建[J]. 天津医药, 2025, 53(5): 483-487. |
| [10] | 王欣欣, 许慧, 吴晓. 妊娠期肝内胆汁淤积症合并GDM孕妇不良妊娠结局的影响因素及预测模型构建[J]. 天津医药, 2025, 53(5): 503-508. |
| [11] | 董丹, 陈立娟, 俞荷花. 急性胰腺炎并发低血压的危险因素分析及预测模型建立[J]. 天津医药, 2025, 53(5): 509-513. |
| [12] | 刘艳丽, 徐文付, 房红娟. 支气管哮喘患儿小气道功能障碍预测模型的构建与验证[J]. 天津医药, 2025, 53(3): 277-282. |
| [13] | 贾方, 李平, 李静, 尹路. 全膝关节置换术后神经认知功能障碍的影响因素及列线图模型的构建[J]. 天津医药, 2025, 53(3): 287-292. |
| [14] | 谷小娜, 陈新春, 寇永妹, 吉国强. 唐山市路北区2020—2024年儿童代谢综合征的分布特征及危险因素分析[J]. 天津医药, 2025, 53(3): 307-311. |
| [15] | 吴宾, 杨自更, 张婧, 李书红, 余凤, 王嘉玮, 李彩玲. 柚皮素对低氧性肺动脉高压大鼠右心室重塑的影响[J]. 天津医药, 2025, 53(2): 129-134. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||