天津医药 ›› 2024, Vol. 52 ›› Issue (11): 1177-1182.doi: 10.11958/20240546
喻萍1,2( ), 周敏2, 苏丹1,2,△()
), 周敏2, 苏丹1,2,△()
收稿日期:2024-05-07
修回日期:2024-07-26
出版日期:2024-11-15
发布日期:2024-11-12
通讯作者:
△E-mail:303483765@qq.com
作者简介:喻萍(1981),女,主治医师,主要从事妇科肿瘤方面研究。E-mail:基金资助:
YU Ping1,2(), ZHOU Min2, SU Dan1,2,△()
Received:2024-05-07
Revised:2024-07-26
Published:2024-11-15
Online:2024-11-12
Contact:
△E-mail:303483765@qq.com
喻萍, 周敏, 苏丹. 卵巢癌化疗耐药预测模型的建立及效果评价[J]. 天津医药, 2024, 52(11): 1177-1182.
YU Ping, ZHOU Min, SU Dan. Construction and validation of chemotherapy resistance prediction model for ovarian cancer[J]. Tianjin Medical Journal, 2024, 52(11): 1177-1182.
摘要:
目的 探讨卵巢癌患者术后化疗发生耐药的影响因素,构建预测模型并评价模型效能。方法 收集经肿瘤细胞减灭术及化疗的407例卵巢癌患者的临床资料,至随访终点根据是否复发分为复发组363例和未复发组44例,其中复发组根据化疗耐药将其分为耐药组59例和敏感组304例。使用单因素分析和Lasso回归筛选变量,建立Logistic模型,用R软件建立列线图并进行评价。结果 与未复发组比较,复发组年龄偏低,低分化比例及FIGO分期Ⅲ—Ⅳ期比例较高(P<0.05)。与敏感组比较,耐药组淋巴结增大、病理类型为非浆液性、FIGO分期Ⅲ—Ⅳ期比例、肿瘤组织免疫组化重组蛋白Ki-67(Ki-67)、蛋白53(P53)、血管内皮生长因子(VEGF)及肾母细胞瘤基因1(WT-1)阳性率较高,手术前后糖类抗原125(CA125)变化率、化疗前后罗马指数(绝经前)变化率及免疫组化蛋白16(P16)阳性率较低(P<0.05)。以Lasso回归筛选出的8个自变量进行Logistic回归,结果显示:术前全腹增强CT有淋巴结增大、病理类型为非浆液性、FIGO分期Ⅲ—Ⅳ期、免疫组化WT1、VEGF阳性,P16阴性是卵巢癌患者发生化疗耐药的独立危险因素。据此建立的列线图模型受试者工作特征曲线下面积为0.837(0.783~0.880),Hosmer-Lemeshow检验结果示模型拟合优度较好,校准曲线及临床决策曲线提示模型有较高的校准度及临床使用度。结论 根据临床数据成功构建了卵巢癌化疗耐药Logistic模型,据此建立的列线图预测模型可有效评估卵巢癌患者发生化疗耐药的风险。
中图分类号:
| 组别 | n | 年龄/岁 | BMI/(kg/m2) | 病理类型(A/B/C/D)# | ||
|---|---|---|---|---|---|---|
| 未复发组 | 44 | 57.7±8.1 | 24.4±3.6 | 33/4/3/4 | ||
| 复发组 | 363 | 52.8±9.6 | 23.6±3.3 | 283/21/32/27 | ||
| t或χ2 | 3.262** | 1.482 | 1.065 | |||
| 组别 | 组织学分级(高/中/低分化) | FIGO分期(Ⅰ/Ⅱ/Ⅲ/Ⅳ) | ||||
| 未复发组 | 23/6/15 | 11/14/18/1 | ||||
| 复发组 | 45/89/229 | 72/41/223/27 | ||||
| Z | 2.192* | 2.924** | ||||
表1 复发组和未复发组一般资料比较
Tab.1 Comparison of clinical variables between the recurrence group and the non-recurrence group
| 组别 | n | 年龄/岁 | BMI/(kg/m2) | 病理类型(A/B/C/D)# | ||
|---|---|---|---|---|---|---|
| 未复发组 | 44 | 57.7±8.1 | 24.4±3.6 | 33/4/3/4 | ||
| 复发组 | 363 | 52.8±9.6 | 23.6±3.3 | 283/21/32/27 | ||
| t或χ2 | 3.262** | 1.482 | 1.065 | |||
| 组别 | 组织学分级(高/中/低分化) | FIGO分期(Ⅰ/Ⅱ/Ⅲ/Ⅳ) | ||||
| 未复发组 | 23/6/15 | 11/14/18/1 | ||||
| 复发组 | 45/89/229 | 72/41/223/27 | ||||
| Z | 2.192* | 2.924** | ||||
| 组别 | n | 年龄/岁 | BMI/(kg/m2) | 术前全腹增强CT | 手术相关 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 肿瘤最长径/cm | 腹腔积液 | 淋巴结增大 | 大网膜转移 | 手术时长/min | 术中出血量/mL | ||||||||||||
| 敏感组 | 304 | 52.3±10.1 | 23.6±3.2 | 9.2±5.6 | 181(59.5) | 100(32.9) | 178(58.6) | 270(210,354) | 500(300,800) | ||||||||
| 耐药组 | 59 | 53.1±9.4 | 23.6±3.5 | 7.8±4.4 | 29(49.2) | 31(52.5) | 30(50.8) | 290(205,350) | 580(350,800) | ||||||||
| t、χ2或Z | 0.516 | 0.020 | 1.530 | 2.186 | 8.270** | 1.199 | 0.456 | 0.265 | |||||||||
| 组别 | Hb降低值/(g/L) | 手术前后血肿瘤标志物变化率/% | |||||||||||||||
| AFP | CA125 | CA199 | CEA | HE4 | ROMA(绝经后) | ROMA(绝经前) | |||||||||||
| 敏感组 | 16.0±8.9 | 2.3±1.0 | 73.5±20.6 | 19.2(7.5,26.2) | 32.3±14.9 | 43.5±8.4 | 35.2(20.6,44.8) | 53.8±15.0 | |||||||||
| 耐药组 | 13.6±5.4 | 1.8±0.8 | 50.3±20.1 | 28.1(11.2,37.1) | 37.8±14.4 | 52.7±2.8 | 23.4(11.2,29.5) | 39.5±13.3 | |||||||||
| Z或t | 0.881 | 1.252 | 7.896** | 0.417 | 0.670 | 0.456 | 0.499 | 1.470 | |||||||||
表2 耐药组和敏感组一般资料比较
Tab.2 Comparison of clinical and surgical variables between the chemotherapy-resistant group and the chemotherapy-sensitive group
| 组别 | n | 年龄/岁 | BMI/(kg/m2) | 术前全腹增强CT | 手术相关 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 肿瘤最长径/cm | 腹腔积液 | 淋巴结增大 | 大网膜转移 | 手术时长/min | 术中出血量/mL | ||||||||||||
| 敏感组 | 304 | 52.3±10.1 | 23.6±3.2 | 9.2±5.6 | 181(59.5) | 100(32.9) | 178(58.6) | 270(210,354) | 500(300,800) | ||||||||
| 耐药组 | 59 | 53.1±9.4 | 23.6±3.5 | 7.8±4.4 | 29(49.2) | 31(52.5) | 30(50.8) | 290(205,350) | 580(350,800) | ||||||||
| t、χ2或Z | 0.516 | 0.020 | 1.530 | 2.186 | 8.270** | 1.199 | 0.456 | 0.265 | |||||||||
| 组别 | Hb降低值/(g/L) | 手术前后血肿瘤标志物变化率/% | |||||||||||||||
| AFP | CA125 | CA199 | CEA | HE4 | ROMA(绝经后) | ROMA(绝经前) | |||||||||||
| 敏感组 | 16.0±8.9 | 2.3±1.0 | 73.5±20.6 | 19.2(7.5,26.2) | 32.3±14.9 | 43.5±8.4 | 35.2(20.6,44.8) | 53.8±15.0 | |||||||||
| 耐药组 | 13.6±5.4 | 1.8±0.8 | 50.3±20.1 | 28.1(11.2,37.1) | 37.8±14.4 | 52.7±2.8 | 23.4(11.2,29.5) | 39.5±13.3 | |||||||||
| Z或t | 0.881 | 1.252 | 7.896** | 0.417 | 0.670 | 0.456 | 0.499 | 1.470 | |||||||||
| 组别 | n | 病理类型(A/B/C/D) | 组织学分级(高/中/低分化) | FIGO分期(Ⅰ/Ⅱ/Ⅲ/Ⅳ) | 免疫组化阳性CDX2 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 敏感组 | 304 | 253/11/19/21 | 32/83/189 | 67/36/181/20 | 160 | ||||||||||||||
| 耐药组 | 59 | 30/10/13/6 | 13/6/40 | 5/5/42/7 | 35 | ||||||||||||||
| χ2或Z | 36.492** | 0.097 | 2.817** | 0.890 | |||||||||||||||
| 组别 | 免疫组化阳性 | ||||||||||||||||||
| CK | CK7 | CK20 | ER | Ki-67 | P16 | WT-1 | PAX-8 | PR | VEGF | Villin | P53 | ||||||||
| 敏感组 | 171(56.2) | 101(33.2) | 171(56.2) | 84(27.6) | 207(68.1) | 131(43.1) | 179(58.9) | 135(44.4) | 56(18.4) | 181(59.5) | 89(29.3) | 173(56.9) | |||||||
| 耐药组 | 23(39.0) | 16(27.1) | 23(39.0) | 17(28.8) | 50(84.7) | 16(27.1) | 46(78.0) | 22(37.3) | 12(20.3) | 45(76.3) | 22(37.3) | 42(71.2) | |||||||
| χ2 | 0.458 | 0.843 | 0.458 | 0.034 | 6.628* | 5.232* | 7.637** | 1.020 | 0.119 | 5.887* | 1.494 | 4.172* | |||||||
表3 耐药组和敏感组的病理资料比较
Tab.3 Comparison of pathological characteristics between the chemotherapy-resistant group and the chemotherapy-sensitive group
| 组别 | n | 病理类型(A/B/C/D) | 组织学分级(高/中/低分化) | FIGO分期(Ⅰ/Ⅱ/Ⅲ/Ⅳ) | 免疫组化阳性CDX2 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 敏感组 | 304 | 253/11/19/21 | 32/83/189 | 67/36/181/20 | 160 | ||||||||||||||
| 耐药组 | 59 | 30/10/13/6 | 13/6/40 | 5/5/42/7 | 35 | ||||||||||||||
| χ2或Z | 36.492** | 0.097 | 2.817** | 0.890 | |||||||||||||||
| 组别 | 免疫组化阳性 | ||||||||||||||||||
| CK | CK7 | CK20 | ER | Ki-67 | P16 | WT-1 | PAX-8 | PR | VEGF | Villin | P53 | ||||||||
| 敏感组 | 171(56.2) | 101(33.2) | 171(56.2) | 84(27.6) | 207(68.1) | 131(43.1) | 179(58.9) | 135(44.4) | 56(18.4) | 181(59.5) | 89(29.3) | 173(56.9) | |||||||
| 耐药组 | 23(39.0) | 16(27.1) | 23(39.0) | 17(28.8) | 50(84.7) | 16(27.1) | 46(78.0) | 22(37.3) | 12(20.3) | 45(76.3) | 22(37.3) | 42(71.2) | |||||||
| χ2 | 0.458 | 0.843 | 0.458 | 0.034 | 6.628* | 5.232* | 7.637** | 1.020 | 0.119 | 5.887* | 1.494 | 4.172* | |||||||
| 组别 | n | 化疗前后血清肿瘤标志物变化率/% | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AFP | CA125 | CA199 | CEA | HE4 | ROMA(绝经后) | ROMA(绝经前) | ||||||
| 敏感组 | 304 | 9.6(1.2,26.9) | 49.3±37.7 | 13.5(7.5,19.2) | 40.5±15.6 | 5.5(3.2,7.8) | 60.0±14.7 | 49.1(34.5,76.3) | ||||
| 耐药组 | 59 | 15.2(9.3,18.5) | 49.9±37.8 | 31.8(17.9,49.4) | 48.2±11.6 | 10.4(5.6,18.4) | 57.1±14.8 | 31.3(19.7,50.5) | ||||
| Z或t | 1.125 | 0.059 | 0.046 | 0.406 | 0.194 | 0.261 | 2.256** | |||||
| 组别 | 化疗疗程/个 | 化疗不良反应 | ||||||||||
| 骨髓抑制 | 肝肾功损害 | 胃肠道反应 | ||||||||||
| 敏感组 | 7.3±2.7 | 88(28.9) | 63(20.7) | 94(30.9) | ||||||||
| 耐药组 | 7.0±3.9 | 16(27.1) | 9(15.3) | 17(28.8) | ||||||||
| χ2或t | 0.847 | 0.081 | 0.930 | 0.103 | ||||||||
表4 耐药组和敏感组化疗相关临床指标及不良反应比较
Tab.4 Comparison of variables of chemotherapy and adverse reactions between the chemotherapy-resistant group and the chemotherapy-sensitive groups
| 组别 | n | 化疗前后血清肿瘤标志物变化率/% | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AFP | CA125 | CA199 | CEA | HE4 | ROMA(绝经后) | ROMA(绝经前) | ||||||
| 敏感组 | 304 | 9.6(1.2,26.9) | 49.3±37.7 | 13.5(7.5,19.2) | 40.5±15.6 | 5.5(3.2,7.8) | 60.0±14.7 | 49.1(34.5,76.3) | ||||
| 耐药组 | 59 | 15.2(9.3,18.5) | 49.9±37.8 | 31.8(17.9,49.4) | 48.2±11.6 | 10.4(5.6,18.4) | 57.1±14.8 | 31.3(19.7,50.5) | ||||
| Z或t | 1.125 | 0.059 | 0.046 | 0.406 | 0.194 | 0.261 | 2.256** | |||||
| 组别 | 化疗疗程/个 | 化疗不良反应 | ||||||||||
| 骨髓抑制 | 肝肾功损害 | 胃肠道反应 | ||||||||||
| 敏感组 | 7.3±2.7 | 88(28.9) | 63(20.7) | 94(30.9) | ||||||||
| 耐药组 | 7.0±3.9 | 16(27.1) | 9(15.3) | 17(28.8) | ||||||||
| χ2或t | 0.847 | 0.081 | 0.930 | 0.103 | ||||||||
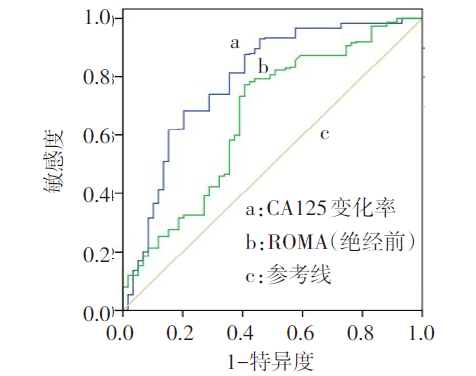
图1 手术前后CA125变化率和化疗前后ROMA(绝经前)变化率预测卵巢癌化疗铂耐药的ROC曲线
Fig.1 ROC curves of change rates of CA125 before and after surgery and the change rates of ROMA (premenopausal) before and after chemotherapy
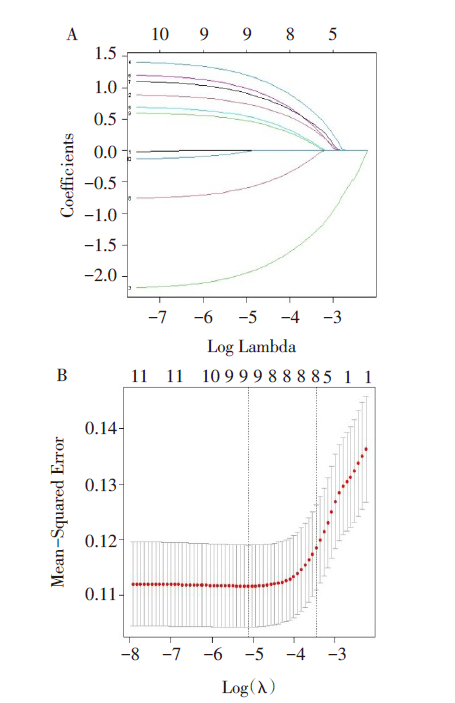
图2 卵巢癌化疗耐药发生的危险因素筛选 A:预测因子系数平面图;B:Lasso回归模型交叉验证图。
Fig.2 Screening of risk factors for chemo-resistance of ovarian cancer
| 临床特征 | β | SE | Waldχ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| 淋巴结增大 | 0.888 | 0.340 | 6.832 | 0.009 | 2.431 | 1.249~4.734 |
| 病理类型 | -2.207 | 0.386 | 32.769 | 0.001 | 0.110 | 0.052~0.234 |
| FIGO分期 | 1.433 | 0.446 | 10.299 | 0.001 | 4.189 | 1.747~10.049 |
| Ki-67 | 0.723 | 0.479 | 2.277 | 0.131 | 2.060 | 0.806~5.269 |
| WT-1 | 1.209 | 0.385 | 9.872 | 0.002 | 3.352 | 1.576~7.128 |
| VEGF | 1.102 | 0.428 | 6.628 | 0.010 | 3.011 | 1.301~6.970 |
| P16 | -0.778 | 0.367 | 4.499 | 0.034 | 0.460 | 0.224~0.943 |
| P53 | 0.622 | 0.357 | 3.036 | 0.081 | 1.863 | 0.925~3.749 |
| 常数项 | -3.849 | 0.668 | 33.208 | 0.001 | 0.021 | — |
表5 卵巢癌化疗耐药预测模型的多因素Logistic回归
Tab.5 Multifactorial Logistic regression for chemotherapy resistance prediction model in ovarian cancer
| 临床特征 | β | SE | Waldχ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| 淋巴结增大 | 0.888 | 0.340 | 6.832 | 0.009 | 2.431 | 1.249~4.734 |
| 病理类型 | -2.207 | 0.386 | 32.769 | 0.001 | 0.110 | 0.052~0.234 |
| FIGO分期 | 1.433 | 0.446 | 10.299 | 0.001 | 4.189 | 1.747~10.049 |
| Ki-67 | 0.723 | 0.479 | 2.277 | 0.131 | 2.060 | 0.806~5.269 |
| WT-1 | 1.209 | 0.385 | 9.872 | 0.002 | 3.352 | 1.576~7.128 |
| VEGF | 1.102 | 0.428 | 6.628 | 0.010 | 3.011 | 1.301~6.970 |
| P16 | -0.778 | 0.367 | 4.499 | 0.034 | 0.460 | 0.224~0.943 |
| P53 | 0.622 | 0.357 | 3.036 | 0.081 | 1.863 | 0.925~3.749 |
| 常数项 | -3.849 | 0.668 | 33.208 | 0.001 | 0.021 | — |
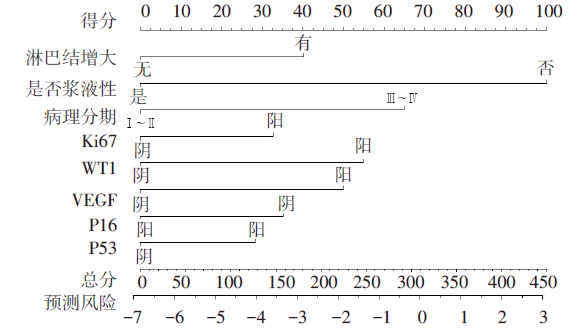
图3 卵巢癌化疗耐药的二元Logistic回归列线图预测模型
Fig.3 Nomogram of binary Logistic regression analysis for predicting the chemotherapy resistance of ovarian cancer
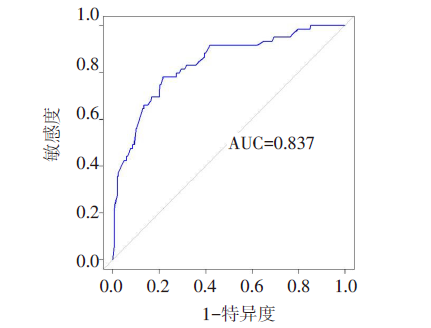
图4 卵巢癌患者发生化疗耐药预测模型的ROC曲线
Fig.4 ROC curve analysis of the prediction model for ovarian cancer patients with chemo-resistance
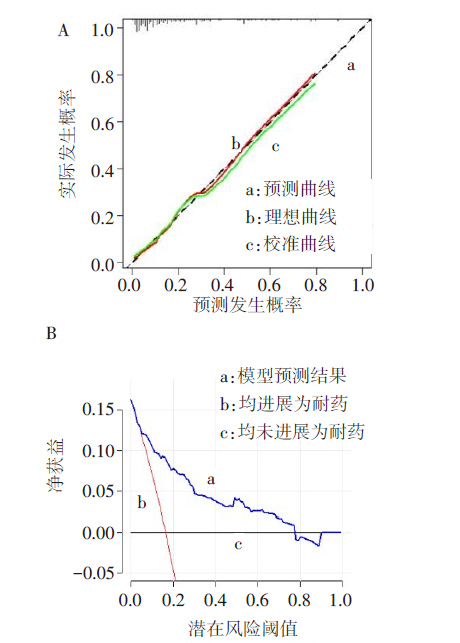
图5 卵巢癌患者发生化疗耐药预测模型的校准曲线和DCA曲线 A:校准曲线;B:DCA曲线。
Fig.5 Calibration curve and DCA curve of a nomogram model predicting chemo-resistance of ovarian cancer
| [1] | 李少儒, 李燕, 刘珊, 等. LncRNA SNHG11通过抑制miR-184/CARM1信号轴促进卵巢癌生长[J]. 天津医药, 2023, 51(6):561-567. |
| LI S R, LI Y, LIU S, et al. Influences of lncRNA SNHG11 on proliferation, apoptosis, migration and invasion of ovarian cancer cells by regulating miR-184/CARM1 signaling axis[J]. Tianjin Med J, 2023, 51(6):561-567. doi:10.11958/20221256. | |
| [2] | 钱瑜华, 高燕, 张艳. 卵巢癌化疗耐药机制及治疗药物的研究进展[J]. 医学综述, 2022, 28(5):929-933. |
| QIAN Y H, GAO Y, ZHANG Y. Research progress of drug resistance mechanism and therapeutic drugs in ovarian cancer[J]. Medical Recapitulate, 2022, 28(5):929-933. doi:10.3969/j.issn.1006-2084.2022.05.017. | |
| [3] | 林世鑫, 高军. 黄酮类化合物抗卵巢癌化疗耐药的作用进展[J]. 天津医药, 2020, 48(10):1010-1014. |
| LIN S X, GAO J. Progress in the effect of flavonoids on drug resistance in ovarian cancer[J]. Tianjin Med J, 2020, 48(10):1010-1014. doi:10.11958/20200130. | |
| [4] | 赵玲, 刘历, 王海燕, 等. 基于CT-PCI与临床指标构建预测晚期上皮性卵巢癌减瘤术结局的列线图模型[J]. 中国医学计算机成像杂志, 2023, 29(3):283-289. |
| ZHAO L, LIU L, WANG H Y, et al. Construction of nomogram model to predict the outcome of debulking surgery for advanced epithelial ovarian cancer based on CT peritoneal cancer index and clinical indicators[J]. Chin Comput Med Imag, 2023, 29(3):283-289. doi:10.19627/j.cnki.cn31-1700/th.2023.03.018. | |
| [5] | ARMSTRONG DK, ALVAREZ RD, BACKES FJ, et al. NCCN guidelines(R) insights:ovarian cancer,version 3.2022[J]. J Natl Compr Canc Netw, 2022, 20(9):972-980. doi:10.6004/jnccn.2022.0047. |
| [6] | BASCH E, BECKER C, ROGAK LJ, et al. Composite grading algorithm for the national cancer institute's patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE)[J]. Clin Trials, 2021, 18(1):104-114. doi:10.1177/1740774520975120. |
| [7] | GONZÁLEZ-MARTÍN A, HARTER P, LEARY A, et al. Newly diagnosed and relapsed epithelial ovarian cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up[J]. Ann Oncol, 2023, 34(10):833-848. doi:10.1016/j.annonc.2023.07.011. |
| [8] | BUECHEL M, HERZOG T J, WESTIN S N, et al. Treatment of patients with recurrent epithelial ovarian cancer for whom platinum is still an option[J]. Ann Oncol, 2019, 30(5):721-732. doi:10.1093/annonc/mdz104. |
| [9] | LUVERO D, PLOTTI F, ALOISIA A, et al. Ovarian cancer relapse: From the latest scientific evidence to the best practice[J]. Crit Rev Oncol Hematol, 2019, 140:28-38. doi:10.1016/j.critrevonc.2019.05.014. |
| [10] | MA G, ZENG S, ZHAO Y, et al. Development and validation of a nomogram to predict cancer-specific survival of mucinous epithelial ovarian cancer after cytoreductive surgery[J]. J Ovarian Res, 2023, 16(1):120. doi:10.1186/s13048-023-01213-2. |
| [11] | SAID S A, BRETVELD R W, KOFFIJBERG H, et al. Clinicopathologic predictors of early relapse in advanced epithelial ovarian cancer: development of prediction models using nationwide data[J]. Cancer Epidemiol, 2021,75:102008. doi:10.1016/j.canep.2021.102008. |
| [12] | 朱艳红, 蔡玉洁, 葛银. 上皮性卵巢癌术后复发的相关影响因素分析[J]. 实用癌症杂志, 2022, 37(1):117-119. |
| ZHU Y H, CAI Y J, GE Y. Analysis of related factors of postoperative recurrence of epithelial ovarian cancer[J]. The Practical Journal of Cancer, 2022, 37(1):117-119. doi:10.3969/j.issn.1001-5930.2022.01.034. | |
| [13] | HEITZ F, HARTER P, ATASEVEN B, et al. Stage-and histologic subtype-dependent frequency of lymph node metastases in patients with epithelial ovarian cancer undergoing systematic pelvic and paraaortic lymphadenectomy[J]. Ann Surg Oncol, 2018, 25(7):2053-2059. doi:10.1245/s10434-018-6412-y. |
| [14] | PEREZ-FIDALGO J A, ORTEGA B, SIMON S, et al. NOTCH signalling in ovarian cancer angiogenesis[J]. Ann Transl Med, 2020, 8(24):1705. doi:10.21037/atm-20-4497. |
| [15] | DAVIS A, TINKER A V, FRIEDLANDER M. "Platinum resistant" ovarian cancer: what is it, who to treat and how to measure benefit?[J]. Gynecol Oncol, 2014, 133(3):624-631. doi:10.1016/j.ygyno.2014.02.038. |
| [16] | FU Y, WANG X, PAN Z, et al. Clinical outcomes and prognostic factors of patients with epithelial ovarian cancer subjected to first-line treatment:a retrospective study of 251 cases[J]. Front Med, 2014, 8(1):91-95. doi:10.1007/s11684-014-0305-7. |
| [17] | 蒋琴, 徐杰, 严科. 卵巢癌铂耐药复发相关临床因素研究[J]. 中国临床医生杂志, 2021, 49(11):1287-1290. |
| JIANG Q, XU J, YAN K. Study on the clinical factors of recurrence of platinum resistance in ovarian cancer[J]. China Clinical Journal, 2021, 49(11):1287-1290. doi:10.3969/j.issn.2095-8552.2021.11.008. | |
| [18] | GRABOWSKI J P, MARTINEZ VILA C, RICHTER R, et al. Ki67 expression as a predictor of chemotherapy outcome in low-grade serous ovarian cancer[J]. Int J Gynecol Cancer, 2020, 30(4):498-503. doi:10.1136/ijgc-2019-000976. |
| [19] | LI J, POI M J, TSAI M D. Regulatory mechanisms of tumor suppressor P16(INK4A) and their relevance to cancer[J]. Biochemistry, 2011, 50(25):5566-5582. doi:10.1021/bi200642e. |
| [20] | COLLOCA G, VENTURINO A, GOVERNATO I. CA125-related tumor cell kinetics variables after chemotherapy in advanced ovarian cancer:a systematic review[J]. Clin Transl Oncol, 2016, 18(8):813-824. doi:10.1007/s12094-015-1441-5. |
| [21] | SONG Y J. Prediction of optimal debulking surgery in ovarian cancer[J]. Gland Surg, 2021, 10(3):1173-1181. doi:10.21037/gs-2019-ursoc-08. |
| [22] | ŠPACIR PRSKALO Z, BULIĆ P, LANGER S, et al. Proofs for implementation of higher HE4 and ROMA index cut-off values in ovarian cancer preoperative stratification[J]. J Obstet Gynaecol, 2019, 39(2):195-201. doi:10.1080/01443615.2018.1476471. |
| [23] | BACALBASA N, DIMA S, BALESCU I, et al. Results of primary cytoreductive surgery in advanced-stage epithelial ovarian cancer: a single-center experience[J]. Anticancer Res, 2015, 35(7):4099-4104. |
| [24] | PARASHKEVOVA A, SEHOULI J, RICHTER R, et al. Preoperative CA-125 value as a predictive factor for postoperative outcome in first relapse of platinum-sensitive serous ovarian cancer[J]. Anticancer Res, 2018, 38(8):4865-4870. doi:10.21873/anticanres.12799. |
| [1] | 姜天佑, 李敏, 孙碧文, 李越洋, 邢丽静, 田晨. Let-7b诱导白血病相关巨噬细胞复极抑制AML的发展[J]. 天津医药, 2026, 54(3): 225-231. |
| [2] | 李斌, 谭振刚, 张华清. 基于息肉特征和血清学指标构建结直肠息肉复发风险预测模型及效能分析[J]. 天津医药, 2026, 54(3): 249-253. |
| [3] | 宋铁军, 林宁宁, 杨悦漪, 王亚斐. 光动力疗法联合超分子水杨酸治疗中重度痤疮患者的疗效分析[J]. 天津医药, 2026, 54(3): 254-258. |
| [4] | 赵丽, 马秀丽, 刘毅, 朱毅. 全麻下腹腔镜胃癌根治术后谵妄发生的危险因素分析[J]. 天津医药, 2026, 54(3): 259-264. |
| [5] | 朱海燕, 王烨, 尹艳. 老年NSCLC患者术后胃肠功能紊乱的危险因素研究[J]. 天津医药, 2026, 54(3): 289-294. |
| [6] | 李明, 金建华, 吴建亭, 王君辉, 许俊. 个性化腰垫与体膜联合固定对宫颈癌放疗患者摆位精度及稳定性的影响[J]. 天津医药, 2026, 54(3): 299-302. |
| [7] | 刘晓华, 韩婷婷, 高玉杰. 增强CT淋巴结边缘特征联合IPI对难治性弥漫大B细胞巴瘤的预测价值[J]. 天津医药, 2026, 54(3): 303-308. |
| [8] | 苏雅, 张东伟, 宇明慧, 王春花, 吴月月. 复方苦参注射液联合靶向和免疫治疗对晚期肝癌的疗效观察[J]. 天津医药, 2026, 54(3): 324-328. |
| [9] | 王喆, 邱林, 马贲. 番茄来源胞外囊泡样颗粒对口腔鳞状细胞癌的作用效果研究[J]. 天津医药, 2026, 54(2): 145-150. |
| [10] | 陈丽, 陈楠. COPD进展为Ⅱ型呼吸衰竭预警模型的建立与验证[J]. 天津医药, 2026, 54(2): 189-195. |
| [11] | 冯昊, 郭晓双, 任晓静, 李明. 吴茱萸汤联合甲磺酸多拉司琼治疗化疗所致呕吐的疗效分析[J]. 天津医药, 2026, 54(2): 201-205. |
| [12] | 庄瑞玲, 杨杰, 陈艳欣, 张雲. 基于转录组与代谢组学联合分析谷氨酰胺合成酶在慢性髓系白血病耐药中的作用机制[J]. 天津医药, 2026, 54(1): 1-7. |
| [13] | 楚兴, 刘磊, 杨华, 陈宏. 胆总管结石并发急性胆源性胰腺炎的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 35-40. |
| [14] | 杨怡, 朵鸿, 杨亚男, 刘云, 梁凤仪, 杨雪琴. 基于肿瘤标志物的实体瘤疗效评价标准在晚期卵巢癌疗效评估中的价值[J]. 天津医药, 2026, 54(1): 46-51. |
| [15] | 程云, 夏明农, 张帆, 李凤. 小儿热性惊厥发展为癫痫的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 52-57. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||