天津医药 ›› 2024, Vol. 52 ›› Issue (11): 1202-1206.doi: 10.11958/20240522
顾芸芸1( ), 仲崇明1, 杨海燕2,△()
), 仲崇明1, 杨海燕2,△()
收稿日期:2024-04-28
修回日期:2024-07-26
出版日期:2024-11-15
发布日期:2024-11-12
通讯作者:
△E-mail:wby1023@126.com
作者简介:顾芸芸(1983),女,副主任技师,主要从事临床生物化学方面研究。E-mail:
GU Yunyun1(), ZHONG Chongming1, YANG Haiyan2,△()
Received:2024-04-28
Revised:2024-07-26
Published:2024-11-15
Online:2024-11-12
Contact:
△E-mail:wby1023@126.com
顾芸芸, 仲崇明, 杨海燕. 尿酸/白蛋白比值对慢性肾脏病患者并发冠心病的预测价值[J]. 天津医药, 2024, 52(11): 1202-1206.
GU Yunyun, ZHONG Chongming, YANG Haiyan. Predictive value of uric acid/albumin ratio for coronary heart disease in patients with chronic kidney disease[J]. Tianjin Medical Journal, 2024, 52(11): 1202-1206.
摘要:
目的 探讨慢性肾脏病(CKD)并发冠心病(CHD)患者尿酸(UA)/白蛋白(Alb)比值(UAR)的水平变化及临床意义。方法 175例CKD患者分为单纯CKD(对照)组94例和并发CHD(试验)组81例。比较2组血常规、血脂、肾功能及UAR差异。二元Logistic回归分析CKD并发CHD的影响因素。受试者工作特征(ROC)曲线分析各指标对CKD并发CHD的预测价值。结果 2组间白细胞计数(WBC)、单核细胞(Mon)、总胆固醇(TC)、甘油三酯(TG)、高密度脂蛋白胆固醇(HDL-C)、低密度脂蛋白胆固醇(LDL-C)的差异无统计学意义。试验组中性粒细胞(Neu)、红细胞分布宽度变异系数(RDW-CV)、尿素氮(BUN)、肌酐(Cr)、UA、UAR水平高于对照组(Ρ<0.05);淋巴细胞(Lym)、红细胞计数(RBC)、平均红细胞血红蛋白浓度(MCHC)、血小板计数(PLT)、估算肾小球滤过率(eGFR)、Alb水平低于对照组(Ρ<0.05)。二分类Logistic回归分析显示,较低水平的RBC、MCHC及较高水平的UAR是CKD并发CHD的独立危险因素。ROC曲线显示,RBC、MCHC、UAR单独检测中UAR曲线下面积(AUC)最大,为0.912(95%CI:0.870~0.953),敏感度0.901,特异度0.777,约登指数0.678,截断值10.935。三者联合检测AUC为0.987(95%CI:0.974~0.999),敏感度0.938,特异度0.979。结论 CKD患者血清UAR水平升高是预测冠心病发生的预测指标,UAR联合RBC和MCHC预测效能更高。
中图分类号:
| 组别 | n | 性别(男/女) | 年龄/岁 | BMI/(kg/m2) | 原发病因(a/b/c/d/e) |
|---|---|---|---|---|---|
| 对照组 | 94 | 45/49 | 48.83±15.96 | 23.23±2.60 | 26/23/17/15/13 |
| 试验组 | 81 | 50/31 | 51.94±15.70 | 23.11±2.20 | 24/20/15/12/10 |
| χ2或t | 3.366 | 1.294 | 0.333 | 0.174 |
表1 对照组与试验组基线资料比较
Tab.1 Comparison of baseline data between the control group and the experimental group
| 组别 | n | 性别(男/女) | 年龄/岁 | BMI/(kg/m2) | 原发病因(a/b/c/d/e) |
|---|---|---|---|---|---|
| 对照组 | 94 | 45/49 | 48.83±15.96 | 23.23±2.60 | 26/23/17/15/13 |
| 试验组 | 81 | 50/31 | 51.94±15.70 | 23.11±2.20 | 24/20/15/12/10 |
| χ2或t | 3.366 | 1.294 | 0.333 | 0.174 |
| 组别 | n | WBC/(×109/L) | Neu/(×109/L) | Lym/(×109/L) | |||||
|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 94 | 6.12(4.88,8.15) | 3.62(2.82,5.15) | 1.82(1.36,2.34) | |||||
| 试验组 | 81 | 6.21(5.02,8.61) | 4.42(3.45,6.10) | 1.10(0.71,1.51) | |||||
| Z | 0.600 | 2.758** | 6.427** | ||||||
| 组别 | Mon/(×109/L) | RBC/(×1012/L) | MCHC/(g/L) | ||||||
| 对照组 | 0.43(0.32,0.58) | 4.35±0.73 | 335.81±10.88 | ||||||
| 试验组 | 0.42(0.30,0.62) | 3.08±0.77 | 329.58±12.93 | ||||||
| Z或t | 0.441 | 11.176** | 3.459** | ||||||
| 组别 | RDW-CV/% | PLT/(×109/L) | |||||||
| 对照组 | 12.30(12.00,13.02) | 221(188,268) | |||||||
| 试验组 | 13.50(12.55,14.95) | 179(150,230) | |||||||
| Z | 5.957** | 3.410** | |||||||
表2 对照组和试验组血液指标比较
Tab. 2 Comparison of blood indexes between the control group and the experimental group
| 组别 | n | WBC/(×109/L) | Neu/(×109/L) | Lym/(×109/L) | |||||
|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 94 | 6.12(4.88,8.15) | 3.62(2.82,5.15) | 1.82(1.36,2.34) | |||||
| 试验组 | 81 | 6.21(5.02,8.61) | 4.42(3.45,6.10) | 1.10(0.71,1.51) | |||||
| Z | 0.600 | 2.758** | 6.427** | ||||||
| 组别 | Mon/(×109/L) | RBC/(×1012/L) | MCHC/(g/L) | ||||||
| 对照组 | 0.43(0.32,0.58) | 4.35±0.73 | 335.81±10.88 | ||||||
| 试验组 | 0.42(0.30,0.62) | 3.08±0.77 | 329.58±12.93 | ||||||
| Z或t | 0.441 | 11.176** | 3.459** | ||||||
| 组别 | RDW-CV/% | PLT/(×109/L) | |||||||
| 对照组 | 12.30(12.00,13.02) | 221(188,268) | |||||||
| 试验组 | 13.50(12.55,14.95) | 179(150,230) | |||||||
| Z | 5.957** | 3.410** | |||||||
| 组别 | n | TC/ (mmol/L) | TG/ (mmol/L) | HDL-C/ (mmol/L) | LDL-C/ (mmol/L) |
|---|---|---|---|---|---|
| 对照组 | 94 | 4.2(3.5,4.8) | 1.5(1.1,2.0) | 1.2±0.2 | 2.4(1.9,2.8) |
| 试验组 | 81 | 4.3(3.8,5.2) | 1.4(1.0,2.0) | 1.2±0.4 | 2.5(2.1,3.0) |
| t或Z | 1.689 | 0.952 | 0.122 | 1.795 |
表3 对照组和试验组血脂指标比较
Tab.3 Comparison of blood lipid indexes between the control group and the experimental group
| 组别 | n | TC/ (mmol/L) | TG/ (mmol/L) | HDL-C/ (mmol/L) | LDL-C/ (mmol/L) |
|---|---|---|---|---|---|
| 对照组 | 94 | 4.2(3.5,4.8) | 1.5(1.1,2.0) | 1.2±0.2 | 2.4(1.9,2.8) |
| 试验组 | 81 | 4.3(3.8,5.2) | 1.4(1.0,2.0) | 1.2±0.4 | 2.5(2.1,3.0) |
| t或Z | 1.689 | 0.952 | 0.122 | 1.795 |
| 组别 | n | BUN/(mmol/L) | Cr/(μmol/L) | ||
|---|---|---|---|---|---|
| 对照组 | 94 | 15.16(13.68,16.67) | 355.85(249.75,452.30) | ||
| 试验组 | 81 | 27.00(19.02,35.41) | 478.00(336.50,711.35) | ||
| Z | 7.125** | 5.029** | |||
| 组别 | UA/(μmol/L) | eGFR/[mL/(min·1.73 m2)] | |||
| 对照组 | 364.50(291.32,391.25) | 43.87(29.80,51.47) | |||
| 试验组 | 470.00(395.50,605.50) | 23.69(15.07,32.14) | |||
| Z | 7.900** | 7.432** | |||
表4 对照组和试验组肾功能指标比较
Tab.4 Comparison of renal function indexes between the control group and the experimental group
| 组别 | n | BUN/(mmol/L) | Cr/(μmol/L) | ||
|---|---|---|---|---|---|
| 对照组 | 94 | 15.16(13.68,16.67) | 355.85(249.75,452.30) | ||
| 试验组 | 81 | 27.00(19.02,35.41) | 478.00(336.50,711.35) | ||
| Z | 7.125** | 5.029** | |||
| 组别 | UA/(μmol/L) | eGFR/[mL/(min·1.73 m2)] | |||
| 对照组 | 364.50(291.32,391.25) | 43.87(29.80,51.47) | |||
| 试验组 | 470.00(395.50,605.50) | 23.69(15.07,32.14) | |||
| Z | 7.900** | 7.432** | |||
| 组别 | n | Alb/(g/L) | UAR |
|---|---|---|---|
| 对照组 | 94 | 36.81±5.25 | 9.24(7.89,10.84) |
| 试验组 | 81 | 30.82±4.24 | 16.07(12.17,20.07) |
| t或Z | 8.209** | 9.378** |
表5 对照组和试验组Alb、UAR水平比较$\bar{x} \pm s$
Tab.5 Comparison of Alb and UAR levels between the control group and the experimental group
| 组别 | n | Alb/(g/L) | UAR |
|---|---|---|---|
| 对照组 | 94 | 36.81±5.25 | 9.24(7.89,10.84) |
| 试验组 | 81 | 30.82±4.24 | 16.07(12.17,20.07) |
| t或Z | 8.209** | 9.378** |
| 指标 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| Neu | 0.331 | 0.206 | 2.573 | 0.109 | 1.392(0.929~2.085) |
| Lym | -1.254 | 0.755 | 2.759 | 0.097 | 0.285(0.065~1.253) |
| RBC | -2.896 | 1.125 | 6.626 | 0.010 | 0.055(0.006~0.501) |
| MCHC | -0.162 | 0.062 | 6.796 | 0.009 | 0.850(0.753~0.961) |
| RDW-CV | 0.313 | 0.550 | 0.324 | 0.569 | 1.367(0.465~4.017) |
| PLT | 0.002 | 0.009 | 0.072 | 0.789 | 1.002(0.985~1.019) |
| BUN | 0.109 | 0.068 | 2.586 | 0.108 | 1.116(0.976~1.275) |
| Cr | 0.002 | 0.002 | 0.479 | 0.489 | 1.002(0.997~1.006) |
| eGFR | -0.061 | 0.033 | 3.473 | 0.062 | 0.941(0.882~1.003) |
| Alb | -0.301 | 0.169 | 3.177 | 0.075 | 0.740(0.531~1.030) |
| UAR | 0.804 | 0.260 | 9.551 | 0.002 | 2.234(1.342~3.718) |
| 常数项 | 59.364 | 26.324 | 5.085 | 0.024 | 0.000 |
表6 CKD患者并发CHD的影响因素分析
Tab.6 Logistic analysis of influencing factors of CHD in patients with CKD
| 指标 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| Neu | 0.331 | 0.206 | 2.573 | 0.109 | 1.392(0.929~2.085) |
| Lym | -1.254 | 0.755 | 2.759 | 0.097 | 0.285(0.065~1.253) |
| RBC | -2.896 | 1.125 | 6.626 | 0.010 | 0.055(0.006~0.501) |
| MCHC | -0.162 | 0.062 | 6.796 | 0.009 | 0.850(0.753~0.961) |
| RDW-CV | 0.313 | 0.550 | 0.324 | 0.569 | 1.367(0.465~4.017) |
| PLT | 0.002 | 0.009 | 0.072 | 0.789 | 1.002(0.985~1.019) |
| BUN | 0.109 | 0.068 | 2.586 | 0.108 | 1.116(0.976~1.275) |
| Cr | 0.002 | 0.002 | 0.479 | 0.489 | 1.002(0.997~1.006) |
| eGFR | -0.061 | 0.033 | 3.473 | 0.062 | 0.941(0.882~1.003) |
| Alb | -0.301 | 0.169 | 3.177 | 0.075 | 0.740(0.531~1.030) |
| UAR | 0.804 | 0.260 | 9.551 | 0.002 | 2.234(1.342~3.718) |
| 常数项 | 59.364 | 26.324 | 5.085 | 0.024 | 0.000 |
| 预测因子 | AUC | AUC 95%CI | 敏感度 | 特异度 | 约登指数 | 截断值 |
|---|---|---|---|---|---|---|
| RBC | 0.882 | 0.832~0.932 | 0.809 | 0.852 | 0.661 | 3.845×1012/L |
| MCHC | 0.650 | 0.568~0.732 | 0.564 | 0.704 | 0.268 | 336.500 g/L |
| UAR | 0.912 | 0.870~0.953 | 0.901 | 0.777 | 0.678 | 10.935 |
| 三者联合 | 0.987 | 0.974~0.999 | 0.938 | 0.979 | 0.917 | — |
表7 RBC、MCHC、UAR及三者联合预测CKD发生CHD的诊断价值
Tab.7 The diagnostic value of RBC, MCHC, UAR and their combination in prediction of CHD in CKD
| 预测因子 | AUC | AUC 95%CI | 敏感度 | 特异度 | 约登指数 | 截断值 |
|---|---|---|---|---|---|---|
| RBC | 0.882 | 0.832~0.932 | 0.809 | 0.852 | 0.661 | 3.845×1012/L |
| MCHC | 0.650 | 0.568~0.732 | 0.564 | 0.704 | 0.268 | 336.500 g/L |
| UAR | 0.912 | 0.870~0.953 | 0.901 | 0.777 | 0.678 | 10.935 |
| 三者联合 | 0.987 | 0.974~0.999 | 0.938 | 0.979 | 0.917 | — |
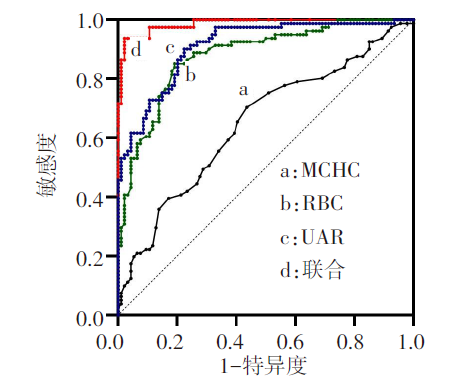
图1 RBC、MCHC、UAR及三者联合预测CKD发生CHD的ROC曲线
Fig.1 ROC curve analysis of RBC, MCHC, UAR and their combination in prediction of CHD in CKD
| [1] | SARNAK M J, AMANN K, BANGALORE S, et al. Chronic kidney disease and coronary artery disease:JACC state-of-the-art review[J]. J Am Coll Cardiol, 2019, 74(14):1823-1838. doi:10.1016/j.jacc.2019.08.1017. |
| [2] | WANG Y N, MA S X, CHEN Y Y, et al. Chronic kidney disease:Biomarker diagnosis to therapeutic targets[J]. Clin Chim Acta, 2019, 499:54-63. doi:10.1016/j.cca.2019.08.030. |
| [3] | KIMURA Y, TSUKUI D, KONO H. Uric acid in inflammation and the pathogenesis of atherosclerosis[J]. Int J Mol Sci, 2021, 22(22):12394. doi:10.3390/ijms222212394. |
| [4] | WAHEED Y, YANG F, SUN D. Role of asymptomatic hyperuricemia in the progression of chronic kidney disease and cardiovascular disease[J]. Korean J Intern Med, 2021, 36(6):1281-1293. doi:10.3904/kjim.2020.340. |
| [5] | 王俊伟, 苏悦, 聂秀玲, 等. 原发性高血压患者血压变异性与高尿酸血症的关系[J]. 天津医药, 2022, 50(12):1297-1301. |
| WANG J, SU Y, NIE X L, et al. Relationship between blood pressure variability and hyperuricemia in patients with essential hypertension[J]. Tianjin Med J, 2022, 50(12):1297-1301. doi:10.11958/20220971. | |
| [6] | 王建雄, 李春君, 张莉, 等. 成人血清尿酸水平与肾功能异常的关系[J]. 天津医药, 2023, 51(1):62-68. |
| WANG J X, LI C J, ZHANG L, et al. Relationship between serum uric acid level and abnormal renal function in adults[J]. Tianjin Med J, 2023, 51(1):62-68. doi:10.11958/20220663. | |
| [7] | MANOLIS A A, MANOLIS T A, MELITA H, et al. Low serum albumin:a neglected predictor in patients with cardiovascular disease[J]. Eur J Intern Med, 2022, 102:24-39. doi:10.1016/j.ejim.2022.05.004. |
| [8] | KALKAN S, CAGAN EFE S, KARAGÖZ A, et al. A new predictor of mortality in ST-Elevation myocardial infarction:the uric acid albumin ratio[J]. Angiology, 2022, 73(5):461-469. doi:10.1177/00033197211066362. |
| [9] | LI S, CHEN H, ZHOU L, et al. The uric acid to albumin ratio:a novel predictor of long-term cardiac mortality in patients with unstable angina pectoris after percutaneous coronary intervention[J]. Scand J Clin Lab Invest Suppl, 2022, 82(4):304-310. doi:10.1080/00365513.2022.2084698. |
| [10] | STEVENS P E, LEVIN A, Kidney Disease:Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease:synopsis of the kidney disease:improving global outcomes 2012 clinical practice guideline[J]. Ann Intern Med, 2013, 158(11):825-830. doi:10.7326/0003-4819-158-11-201306040-00007. |
| [11] | KNUUTI J, WIJNS W, SARASTE A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes[J]. Eur Heart J,2020, 41(3):407-477. doi:10.1093/eurheartj/ehz425. |
| [12] | LUO J, ZHOU Y, SONG Y, et al. Association between the neutrophil-to-lymphocyte ratio and in-hospital mortality in patients with chronic kidney disease and coronary artery disease in the intensive care unit[J]. Eur J Med Res, 2024, 29(1):260. doi:10.1186/s40001-024-01850-3. |
| [13] | YANG Y, LI G, ZHANG R. Correlation analysis of acute coronary syndrome with serum IL-18,MMP-9,hs-CRP,and plasma FIB[J]. Biomed Res Int, 2022,2022:5984184. doi:10.1155/2022/5984184. |
| [14] | DZIEDZIC E A, GASIOR J S, TUZIMEK A, et al. Investigation of the associations of novel inflammatory biomarkers-systemic inflammatory index (SⅡ) and systemic inflammatory response index (SIRI)-with the severity of coronary artery disease and acute coronary syndrome occurrence[J]. Int J Mol Sci, 2022, 23(17):9553. doi:10.3390/ijms23179553. |
| [15] | SHAYA G E, LEUCKER T M, JONES S R, et al. Coronary heart disease risk:low-density lipoprotein and beyond[J]. Trends Cardiovasc Med, 2022, 32(4):181-194. doi:10.1016/j.tcm.2021.04.002. |
| [16] | HAN K, LU Q, ZHU WJ, et al. Correlations of degree of coronary artery stenosis with blood lipid,CRP,Hcy,GGT,SCD36 and fibrinogen levels in elderly patients with coronary heart disease[J]. Eur Rev Med Pharmacol Sci, 2019, 23(21):9582-9589. doi:10.26355/eurrev_201911_19453. |
| [17] | 黄建槐, 陈安珉, 陈蕴, 等. 中性粒细胞/淋巴细胞比值、血尿酸与维持性血液透析患者心血管事件的关系[J]. 徐州医科大学学报, 2023, 43(5):313-318. |
| HUANG J H, CHEN A M, CHEN Y, et al. Relationship among neutrophil-to-lymphocyte ratio,serum uric acid and cardiovascular events in patient with maintenance hemodialysis[J]. J Xuzhou Med Univ, 2023, 43(5): 313-318. doi:10.3969/j.Issn.2096-3882.2023.05.001. | |
| [18] | 李娟. 血小板/淋巴细胞比值与慢性肾衰竭腹膜透析患者心脑血管事件的关系[D]. 南昌: 南昌大学, 2021. |
| LI J. The association of platelet to lymphocyte ratio with cardiovascular and cerebrovascular events in peritoneal dialysis patients with chronic renal failure[D]. Nanchang: Nanchang University, 2021. doi:10.27232/d.cnki.gnchu.2021.000629. | |
| [19] | JIANG H, LI J, YU K, et al. Associations of estimated glomerular filtration rate and blood urea nitrogen with incident coronary heart disease:the Dongfeng-Tongji Cohort Study[J]. Sci Rep, 2017, 7(1):9987. doi:10.1038/s41598-017-09591-6. |
| [20] | LU Y A, FAN P C, LEE C C, et al. Red cell distribution width associated with adverse cardiovascular outcomes in patients with chronic kidney disease[J]. BMC Nephrol, 2017, 18(1):361-368. doi:10.1186/s12882-017-0766-4. |
| [21] | LAFFIN L, BAKRIS G L. Intersection between chronic kidney disease and cardiovascular disease[J]. Curr Cardiol Rep, 2021, 23(9):117-127. doi:10.1007/s11886-021-01546-8. |
| [22] | SONODA H, TAKASE H, DOHI Y, et al. Uric acid levels predict future development of chronic kidney disease[J]. Am J Nephrol, 2011, 33(4):352-357. doi:10.1159/000326848. |
| [23] | YUICHI S, ATSUSHI T, KOICHI N, et al. Uric acid and cardiovascular disease:a clinical review[J]. J Cardiol, 2020, 78(1):51-57. doi:10.1016/j.jjcc.2020.12.01. |
| [24] | 吴聪. 腹膜透析患者血尿酸与心血管事件的分层分析[D]. 南昌: 南昌大学, 2020. |
| WU C. Stratified analysis of serum uric acid and cardiovascular events in peritoneal dialysis patients[D]. Nanchang: Nanchang University, 2020. doi:10.27232/d.cnki.gnchu.2020.000642. | |
| [25] | 尹敏, 顾玉程, 王瑞芳, 等. 慢性肾脏病非透析患者血尿酸水平与心血管疾病的相关性分析[J]. 中国实验诊断学, 2022, 26(2):218-221. |
| YIN M, GU Y C, WANG R F, et al. Correlation analysis of blood uric acid level and cardiovascular disease in non-dialysis patients with chronic kidney disease[J]. Chinese Experimental Diagnostics, 2022, 26(2):218-221. doi:10.3969/j.issn.1007-4287.2022.02.017. | |
| [26] | 邱珊芳, 滕杰, 沈波, 等. 透析前血尿酸水平与腹膜透析患者全因死亡的相关性分析[J]. 中国临床医学, 2020, 27(5):815-821. |
| QIU S F, TENG J, SHEN B, et al. Correlation analysis between predialysis blood uric acid level and all-cause death in peritoneal dialysis patients[J]. Chinese Journal of Clinical Medicine, 2020, 27(5):815-821. doi:10.12025/j.issn.1008-6358.2020.20192078. | |
| [27] | POLAT N, OYLUMLU M, IŞIK M A, et al. Prognostic significance of serum albumin in patients with acute coronary syndrome[J]. Angiology, 2020, 71(10):903-908. doi:10.1177/0003319720941747. |
| [28] | SELÇUK M, ÇINAR T, ŞAYLIK F, et al. Predictive value of uric acid/albumin ratio for the prediction of new-onset atrial fibrillation in patients with ST-Elevation myocardial infarction[J]. Rev Invest Clin, 2022, 74(3):156-164. doi:10.24875/RIC.22000072. |
| [29] | ÇAKMAK E O, BAYAM E, ÇELIK M, et al. Uric acid-to-albumin ratio:a novel marker for the extent of coronary artery disease in patients with Non-ST-Elevated myocardial infarction[J]. Pulse(Basel), 2021, 8(3/4):99-107. doi:10.1159/000514533. |
| [1] | 刘俊芬, 郭宝珠, 程志华, 卫志锋, 刘圣君. 尿酸、脂联素与水肿指数对腹膜透析患者主要不良心血管事件的预测价值[J]. 天津医药, 2026, 54(3): 274-278. |
| [2] | 邬文伟, 丘妙玲, 朱海坤, 罗荣. 乙醛脱氢酶2基因多态性在冠心病中的研究进展[J]. 天津医药, 2026, 54(1): 108-112. |
| [3] | 李霖, 李丹阳, 崔岩. 糖尿病肾病合并心脏自主神经病变随机森林模型的构建及验证[J]. 天津医药, 2026, 54(1): 41-45. |
| [4] | 林鑫星, 蒋艳红, 胡顺明, 王加亮, 刘晨路, 徐速. 血清铜/锌、血乳酸/白蛋白比值联合粪便钙卫蛋白评估溃疡性结肠炎病情及治疗结局的研究[J]. 天津医药, 2026, 54(1): 78-83. |
| [5] | 孔翠文, 路延双, 孙丽萍, 于芬芬. LncRNA SNHG14靶向miR-30a-5p对高糖诱导的足细胞损伤的影响[J]. 天津医药, 2025, 53(9): 903-909. |
| [6] | 马良, 胡立影, 石羽, 赵永安, 孙雅斯, 孙广东. 不同血压水平糖尿病肾病患者黄斑区视网膜厚度特征分析[J]. 天津医药, 2025, 53(9): 923-926. |
| [7] | 徐培璐, 乔建民, 李静, 刘建荣, 陈树军, 季春鹏. 心外膜脂肪厚度联合血清ADAM10、STIM1对冠心病的诊断价值[J]. 天津医药, 2025, 53(9): 963-966. |
| [8] | 焦爱菊, 朱若兰, 张春花, 李文瑞, 孙霞, 赵玮婧, 任宝龙. 血清Lp-PLA2、Hcy联合WMH对脑小血管病患者认知障碍的预测价值[J]. 天津医药, 2025, 53(8): 846-849. |
| [9] | 刘丽, 侯健, 张巧玲, 杨宏秀, 袁宝军. C1q、MBL、C5a与2型糖尿病肾脏病进程及肾小管损伤的相关性[J]. 天津医药, 2025, 53(6): 603-609. |
| [10] | 沙亚娟, 赵莹琰, 李海燕. 那不勒斯预后评分和预后营养指数对子宫内膜癌患者术后复发的预测价值[J]. 天津医药, 2025, 53(6): 634-639. |
| [11] | 周美娟, 缪小祥. 帕金森病患者血清miR-214-3p、miR-124-3p表达水平与病情严重程度的关系及其早期诊断价值[J]. 天津医药, 2025, 53(5): 498-502. |
| [12] | 王欣欣, 许慧, 吴晓. 妊娠期肝内胆汁淤积症合并GDM孕妇不良妊娠结局的影响因素及预测模型构建[J]. 天津医药, 2025, 53(5): 503-508. |
| [13] | 胡卓, 谢松波, 游诗伟. 序贯器官衰竭评分联合Clara细胞蛋白和血管生成素-2对脓毒症所致ARDS的预测价值[J]. 天津医药, 2025, 53(5): 519-522. |
| [14] | 宋志新, 叶建军, 杨道武. 交通创伤患者继发创伤性凝血功能障碍的危险因素分析[J]. 天津医药, 2025, 53(4): 416-419. |
| [15] | 李冰心, 许军英, 张雅茹, 周小兵. 冬虫夏草通过调控AMPK/mTOR通路保护高糖诱导的足细胞损伤[J]. 天津医药, 2025, 53(3): 225-229. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||