Tianjin Medical Journal ›› 2024, Vol. 52 ›› Issue (4): 416-421.doi: 10.11958/20230833
• Clinical Research • Previous Articles Next Articles
REN Yan( ), CHEN Shanping, ZHOU Lihua, WANG Lingxiao, GUAN Lijuan, YANG Yongxue△()
), CHEN Shanping, ZHOU Lihua, WANG Lingxiao, GUAN Lijuan, YANG Yongxue△()
Received:2023-06-19
Revised:2023-11-21
Published:2024-04-15
Online:2024-04-19
Contact:
△E-mail:REN Yan, CHEN Shanping, ZHOU Lihua, WANG Lingxiao, GUAN Lijuan, YANG Yongxue. The predictive value of laboratory frailty index for the risk of sepsis and septic shock in elderly CAP inpatients[J]. Tianjin Medical Journal, 2024, 52(4): 416-421.
CLC Number:
| 变量 | 低限值 | 高限值 | |
|---|---|---|---|
| 生命体征 | 腋温/℃ | 36 | 37 |
| 脉搏/(次/min) | 60 | 100 | |
| 呼吸频率/(次/min) | 12 | 20 | |
| 收缩压/mmHg | 90 | 140 | |
| 舒张压/mmHg | 60 | 90 | |
| 血常规 | 白细胞/(×109/L) | 3.7 | 9.6 |
| 血红蛋白/(g/L) | 110 | 172 | |
| 血小板/(×109/L) | 85 | 320 | |
| 单核细胞/(×109/L) | 0.10 | 0.97 | |
| 嗜酸性细胞/(×109/L) | 0.02 | 0.5 | |
| 嗜碱性细胞/(×109/L) | 0 | 0.1 | |
| 血生化 | 钠/(mmol/L) | 135 | 145 |
| 钾/(mmol/L) | 3.5 | 5.5 | |
| 镁/(mmol/L) | 0.78 | 1.03 | |
| 钙/(mmol/L) | 2.17 | 2.54 | |
| 磷/(mmol/L) | 0.81 | 1.45 | |
| 氯/(mmol/L) | 96 | 108 | |
| 总蛋白/(g/L) | 60 | 85 | |
| 球蛋白/(g/L) | 15 | 45 | |
| 白蛋白/(g/L) | 35 | 55 | |
| 总胆红素/(μmol/L) | 5.1 | 28 | |
| 直接胆红素/(μmol/L) | 0 | 10 | |
| 间接胆红素/(μmol/L) | 0 | 20 | |
| 乳酸脱氢酶/(U/L) | 109 | 245 | |
| 丙氨酸转氨酶/(U/L) | 0 | 45 | |
| 天冬氨酸转氨酶/(U/L) | 8 | 38 | |
| 碱性磷酸酶/(U/L) | 40 | 150 | |
| 谷氨酰转肽酶/(U/L) | 8 | 50 | |
| 腺苷脱氢酶/(U/L) | 4 | 22 | |
| 尿素氮/(mmol/L) | 2.7 | 8.2 | |
| 尿酸/(mmol/L) | 150(女)/ 210(男) | 360(女)/ 430(男) | |
| 肌酸激酶/(U/L) | 50 | 130 | |
| 氨基末端脑钠尿肽/(ng/L) | 0 | 120 | |
| 总胆固醇/(mmol/L) | 3.90 | 6.46 | |
| 甘油三酯/(mmol/L) | 0.34 | 2.30 | |
| 高密度脂蛋白胆固醇/(mmol/L) | 0.91 | 2.28 | |
| 低密度脂蛋白胆固醇/(mmol/L) | 0 | 3.82 | |
| 凝血功能 | 凝血酶原时间/s | 9 | 13 |
| 凝血酶时间/s | 14 | 21 | |
| 纤维蛋白原降解产物/(mg/L) | 0 | 5 |
Tab.1 Laboratory variables for the construction of FI-LAB
| 变量 | 低限值 | 高限值 | |
|---|---|---|---|
| 生命体征 | 腋温/℃ | 36 | 37 |
| 脉搏/(次/min) | 60 | 100 | |
| 呼吸频率/(次/min) | 12 | 20 | |
| 收缩压/mmHg | 90 | 140 | |
| 舒张压/mmHg | 60 | 90 | |
| 血常规 | 白细胞/(×109/L) | 3.7 | 9.6 |
| 血红蛋白/(g/L) | 110 | 172 | |
| 血小板/(×109/L) | 85 | 320 | |
| 单核细胞/(×109/L) | 0.10 | 0.97 | |
| 嗜酸性细胞/(×109/L) | 0.02 | 0.5 | |
| 嗜碱性细胞/(×109/L) | 0 | 0.1 | |
| 血生化 | 钠/(mmol/L) | 135 | 145 |
| 钾/(mmol/L) | 3.5 | 5.5 | |
| 镁/(mmol/L) | 0.78 | 1.03 | |
| 钙/(mmol/L) | 2.17 | 2.54 | |
| 磷/(mmol/L) | 0.81 | 1.45 | |
| 氯/(mmol/L) | 96 | 108 | |
| 总蛋白/(g/L) | 60 | 85 | |
| 球蛋白/(g/L) | 15 | 45 | |
| 白蛋白/(g/L) | 35 | 55 | |
| 总胆红素/(μmol/L) | 5.1 | 28 | |
| 直接胆红素/(μmol/L) | 0 | 10 | |
| 间接胆红素/(μmol/L) | 0 | 20 | |
| 乳酸脱氢酶/(U/L) | 109 | 245 | |
| 丙氨酸转氨酶/(U/L) | 0 | 45 | |
| 天冬氨酸转氨酶/(U/L) | 8 | 38 | |
| 碱性磷酸酶/(U/L) | 40 | 150 | |
| 谷氨酰转肽酶/(U/L) | 8 | 50 | |
| 腺苷脱氢酶/(U/L) | 4 | 22 | |
| 尿素氮/(mmol/L) | 2.7 | 8.2 | |
| 尿酸/(mmol/L) | 150(女)/ 210(男) | 360(女)/ 430(男) | |
| 肌酸激酶/(U/L) | 50 | 130 | |
| 氨基末端脑钠尿肽/(ng/L) | 0 | 120 | |
| 总胆固醇/(mmol/L) | 3.90 | 6.46 | |
| 甘油三酯/(mmol/L) | 0.34 | 2.30 | |
| 高密度脂蛋白胆固醇/(mmol/L) | 0.91 | 2.28 | |
| 低密度脂蛋白胆固醇/(mmol/L) | 0 | 3.82 | |
| 凝血功能 | 凝血酶原时间/s | 9 | 13 |
| 凝血酶时间/s | 14 | 21 | |
| 纤维蛋白原降解产物/(mg/L) | 0 | 5 |
| 组别 | n | 年龄 | 男性 | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 65~74岁 | 75~84岁 | ≥85岁 | ||||||||||||||||||||||
| 非衰弱组 | 386 | 191(49.5) | 156(40.4) | 39(10.1) | 227(58.8) | |||||||||||||||||||
| 衰弱组 | 116 | 60(51.7) | 31(26.7) | 25(21.6) | 75(64.7) | |||||||||||||||||||
| χ2 | 13.747** | 1.272 | ||||||||||||||||||||||
| 组别 | 在婚 | 吸烟 | 饮酒 | 肿瘤 | 慢性肝病 | |||||||||||||||||||
| 非衰弱组 | 372(96.4) | 192(49.7) | 123(31.9) | 16(4.1) | 39(10.1) | |||||||||||||||||||
| 衰弱组 | 107(92.2) | 60(51.7) | 41(35.3) | 22(19.0) | 13(11.2) | |||||||||||||||||||
| χ2 | 3.483 | 0.140 | 0.419 | 28.001** | 0.117 | |||||||||||||||||||
| 组别 | CHF | 脑卒中史 | 慢性肾病 | COPD | 糖尿病 | |||||||||||||||||||
| 非衰弱组 | 39(10.1) | 27(8.0) | 31(8.0) | 279(72.3) | 84(21.8) | |||||||||||||||||||
| 衰弱组 | 24(38.1) | 10(10.8) | 14(31.1) | 54(46.6) | 35(30.2) | |||||||||||||||||||
| χ2 | 9.108** | 0.345 | 1.782 | 26.438** | 3.489 | |||||||||||||||||||
| 组别 | 高血压 | 发热 | 精神状态改变 | 胸水 | ||||||||||||||||||||
| 非衰弱组 | 150(38.9) | 28(7.3) | 19(4.9) | 85(22.0) | ||||||||||||||||||||
| 衰弱组 | 49(42.2) | 27(23.3) | 30(25.9) | 69(59.5) | ||||||||||||||||||||
| χ2 | 0.426 | 23.470** | 44.402** | 58.862** | ||||||||||||||||||||
| 组别 | CURB-65评分/分 | 脓毒症 | 脓毒性休克 | 死亡 | ||||||||||||||||||||
| 非衰弱组 | 2(1,2) | 42(10.9) | 15(3.9) | 10(2.6) | ||||||||||||||||||||
| 衰弱组 | 2(2,3) | 73(62.9) | 36(31.0) | 11(9.5) | ||||||||||||||||||||
| χ2或Z | 8.601** | 136.831** | 72.027** | 10.570** | ||||||||||||||||||||
Tab.2 Comparison of baseline data between two groups
| 组别 | n | 年龄 | 男性 | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 65~74岁 | 75~84岁 | ≥85岁 | ||||||||||||||||||||||
| 非衰弱组 | 386 | 191(49.5) | 156(40.4) | 39(10.1) | 227(58.8) | |||||||||||||||||||
| 衰弱组 | 116 | 60(51.7) | 31(26.7) | 25(21.6) | 75(64.7) | |||||||||||||||||||
| χ2 | 13.747** | 1.272 | ||||||||||||||||||||||
| 组别 | 在婚 | 吸烟 | 饮酒 | 肿瘤 | 慢性肝病 | |||||||||||||||||||
| 非衰弱组 | 372(96.4) | 192(49.7) | 123(31.9) | 16(4.1) | 39(10.1) | |||||||||||||||||||
| 衰弱组 | 107(92.2) | 60(51.7) | 41(35.3) | 22(19.0) | 13(11.2) | |||||||||||||||||||
| χ2 | 3.483 | 0.140 | 0.419 | 28.001** | 0.117 | |||||||||||||||||||
| 组别 | CHF | 脑卒中史 | 慢性肾病 | COPD | 糖尿病 | |||||||||||||||||||
| 非衰弱组 | 39(10.1) | 27(8.0) | 31(8.0) | 279(72.3) | 84(21.8) | |||||||||||||||||||
| 衰弱组 | 24(38.1) | 10(10.8) | 14(31.1) | 54(46.6) | 35(30.2) | |||||||||||||||||||
| χ2 | 9.108** | 0.345 | 1.782 | 26.438** | 3.489 | |||||||||||||||||||
| 组别 | 高血压 | 发热 | 精神状态改变 | 胸水 | ||||||||||||||||||||
| 非衰弱组 | 150(38.9) | 28(7.3) | 19(4.9) | 85(22.0) | ||||||||||||||||||||
| 衰弱组 | 49(42.2) | 27(23.3) | 30(25.9) | 69(59.5) | ||||||||||||||||||||
| χ2 | 0.426 | 23.470** | 44.402** | 58.862** | ||||||||||||||||||||
| 组别 | CURB-65评分/分 | 脓毒症 | 脓毒性休克 | 死亡 | ||||||||||||||||||||
| 非衰弱组 | 2(1,2) | 42(10.9) | 15(3.9) | 10(2.6) | ||||||||||||||||||||
| 衰弱组 | 2(2,3) | 73(62.9) | 36(31.0) | 11(9.5) | ||||||||||||||||||||
| χ2或Z | 8.601** | 136.831** | 72.027** | 10.570** | ||||||||||||||||||||
| 变量 | 脓毒症 | 脓毒性休克 | ||
|---|---|---|---|---|
| 未调整RR(95%CI) | P | 未调整RR(95%CI) | P | |
| 年龄 | 1.010(0.987~1.034) | 0.388 | 0.988(0.950~1.029) | 0.568 |
| 女性 | 0.805(0.573~1.131) | 0.211 | 0.755(0.434~1.314) | 0.320 |
| 吸烟史 | 1.202(0.870~1.660) | 0.264 | 0.954(0.567~1.605) | 0.859 |
| 饮酒史 | 1.058(0.754~1.483) | 0.745 | 1.124(0.653~1.935) | 0.673 |
| 肿瘤 | 2.417(1.679~3.479) | <0.001 | 3.757(2.154~6.552) | <0.001 |
| CHF | 2.243(1.606~3.132) | <0.001 | 1.916(1.038~3.537) | 0.038 |
| 脑卒中史 | 2.180(1.474~3.224) | <0.001 | 3.065(1.674~5.612) | <0.001 |
| 慢性肾脏疾病 | 1.183(0.708~1.977) | 0.521 | 1.616(0.774~3.374) | 0.202 |
| 慢性肝脏疾病 | 0.915(0.527~1.588) | 0.753 | 0.541(0.175~1.675) | 0.287 |
| 糖尿病 | 1.527(1.095~2.130) | 0.013 | 2.076(1.231~3.504) | 0.006 |
| 高血压 | 1.599(1.162~2.199) | 0.004 | 1.349(0.802~2.269) | 0.259 |
| COPD | 0.419(0.305~0.575) | <0.001 | 0.254(0.146~0.441) | <0.001 |
| 衰弱 | 5.784(4.209~7.948) | <0.001 | 7.986(4.537~14.058) | <0.001 |
| FI-LAB | 1.073(1.063~1.083) | <0.001 | 1.088(1.071~1.105) | <0.001 |
| 发热 | 1.923(1.327~2.786) | 0.018 | 2.780(1.582~4.887) | <0.001 |
| 精神状态改变 | 5.319(4.187~6.756) | <0.001 | 8.889(5.594~14.126) | <0.001 |
| 胸水 | 2.938(2.141~4.030) | <0.001 | 3.503(2.063~5.946) | <0.001 |
Tab.3 Univariate analysis of influencing factors of sepsis/septic shock in elderly patients with CAP
| 变量 | 脓毒症 | 脓毒性休克 | ||
|---|---|---|---|---|
| 未调整RR(95%CI) | P | 未调整RR(95%CI) | P | |
| 年龄 | 1.010(0.987~1.034) | 0.388 | 0.988(0.950~1.029) | 0.568 |
| 女性 | 0.805(0.573~1.131) | 0.211 | 0.755(0.434~1.314) | 0.320 |
| 吸烟史 | 1.202(0.870~1.660) | 0.264 | 0.954(0.567~1.605) | 0.859 |
| 饮酒史 | 1.058(0.754~1.483) | 0.745 | 1.124(0.653~1.935) | 0.673 |
| 肿瘤 | 2.417(1.679~3.479) | <0.001 | 3.757(2.154~6.552) | <0.001 |
| CHF | 2.243(1.606~3.132) | <0.001 | 1.916(1.038~3.537) | 0.038 |
| 脑卒中史 | 2.180(1.474~3.224) | <0.001 | 3.065(1.674~5.612) | <0.001 |
| 慢性肾脏疾病 | 1.183(0.708~1.977) | 0.521 | 1.616(0.774~3.374) | 0.202 |
| 慢性肝脏疾病 | 0.915(0.527~1.588) | 0.753 | 0.541(0.175~1.675) | 0.287 |
| 糖尿病 | 1.527(1.095~2.130) | 0.013 | 2.076(1.231~3.504) | 0.006 |
| 高血压 | 1.599(1.162~2.199) | 0.004 | 1.349(0.802~2.269) | 0.259 |
| COPD | 0.419(0.305~0.575) | <0.001 | 0.254(0.146~0.441) | <0.001 |
| 衰弱 | 5.784(4.209~7.948) | <0.001 | 7.986(4.537~14.058) | <0.001 |
| FI-LAB | 1.073(1.063~1.083) | <0.001 | 1.088(1.071~1.105) | <0.001 |
| 发热 | 1.923(1.327~2.786) | 0.018 | 2.780(1.582~4.887) | <0.001 |
| 精神状态改变 | 5.319(4.187~6.756) | <0.001 | 8.889(5.594~14.126) | <0.001 |
| 胸水 | 2.938(2.141~4.030) | <0.001 | 3.503(2.063~5.946) | <0.001 |
| 变量 | 模型1 | 模型2 | ||
|---|---|---|---|---|
| aRR(95%CI) | P | aRR(95%CI) | P | |
| 脓毒症 | ||||
| 衰弱/FI-LAB | 3.392(2.306~4.989) | <0.001 | 1.059(1.046~1.072) | <0.001 |
| 精神状态改变 | 2.412(1.744~3.335) | <0.001 | 2.016(1.461~2.781) | <0.001 |
| CHF | 1.552(1.099~2.192) | 0.013 | ||
| 脑卒中史 | 1.572(1.007~2.453) | 0.047 | ||
| 胸水 | 1.364(1.029~1.810) | 0.031 | ||
| 脓毒性休克 | ||||
| 衰弱/FI-LAB | 3.374(1.692~6.730) | 0.001 | 1.062(1.040~1.084) | <0.001 |
| 精神状态改变 | 3.500(1.964~6.236) | <0.001 | 2.789(1.584~4.912) | <0.001 |
Tab.4 Multivariate analysis of influencing factors of sepsis/septic shock in elderly patients with CAP
| 变量 | 模型1 | 模型2 | ||
|---|---|---|---|---|
| aRR(95%CI) | P | aRR(95%CI) | P | |
| 脓毒症 | ||||
| 衰弱/FI-LAB | 3.392(2.306~4.989) | <0.001 | 1.059(1.046~1.072) | <0.001 |
| 精神状态改变 | 2.412(1.744~3.335) | <0.001 | 2.016(1.461~2.781) | <0.001 |
| CHF | 1.552(1.099~2.192) | 0.013 | ||
| 脑卒中史 | 1.572(1.007~2.453) | 0.047 | ||
| 胸水 | 1.364(1.029~1.810) | 0.031 | ||
| 脓毒性休克 | ||||
| 衰弱/FI-LAB | 3.374(1.692~6.730) | 0.001 | 1.062(1.040~1.084) | <0.001 |
| 精神状态改变 | 3.500(1.964~6.236) | <0.001 | 2.789(1.584~4.912) | <0.001 |
| 结局 | AUC | AUC 95%CI | 敏感度/% | 特异度/% | 截断值 |
|---|---|---|---|---|---|
| 脓毒症 | 0.865 | 0.824~0.905 | 79.1 | 78.0 | 0.28 |
| 脓毒性休克 | 0.850 | 0.795~0.906 | 93.3 | 62.7 | 0.42 |
Tab.5 Diagnostic efficacy of FI-LAB in predicting sepsis/septic shock
| 结局 | AUC | AUC 95%CI | 敏感度/% | 特异度/% | 截断值 |
|---|---|---|---|---|---|
| 脓毒症 | 0.865 | 0.824~0.905 | 79.1 | 78.0 | 0.28 |
| 脓毒性休克 | 0.850 | 0.795~0.906 | 93.3 | 62.7 | 0.42 |
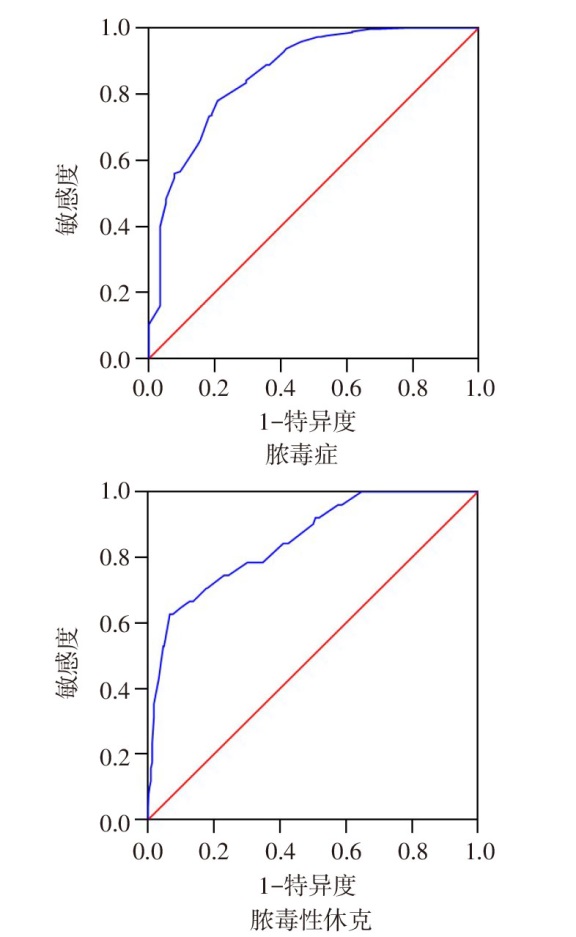
Fig.1 The area of ROC curve of FI-LAB for predicting CAP-associated sepsis /septic shock in elderly inpatients with CAP
| [1] | 宋凯, 湛立娜, 章静, 等. 脓毒症肺损伤相关信号转导通路研究进展[J]. 中国中西医结合外科杂志, 2023, 29(6):854-858. |
| SONG K, ZHAN L N, ZHANG J, et al. Research progress on signal transduction pathways related to sepsis induced lung injury[J]. Chinese Journal of Integrated Traditional Chinese and Western Medicine Surgery, 2023, 29(6):854-858. doi:10.3969/j.issn.1007-6948.2023.06.026. | |
| [2] | CILLÓNIZ C, DOMINEDÓ C, IELPO A, et al. Risk and prognostic factors in very old patients with sepsis secondary to community-acquired pneumonia[J]. J Clin Med, 2019, 8(7):961. doi:10.3390/jcm8070961. |
| [3] | CLEGG A, YOUNG J, ILIFFE S, et al. Frailty in elderly people[J]. Lancet, 2013, 381(9868):752-762. doi:10.1016/s0140-6736(12)62167-9. |
| [4] | WANG Y, ZHANG R, SHEN Y, et al. Prediction of chemotherapy adverse reactions and mortality in older patients with primary lung cancer through frailty index based on routine laboratory data[J]. Clin Interv Aging, 2019, 14:1187-1197. doi:10.2147/CIA.S201873. |
| [5] | HOWLETT S E, ROCKWOOD M R, MITNITSKI A, et al. Standard laboratory tests to identify older adults at increased risk of death[J]. BMC Med, 2014, 12:171. doi:10.1186/s12916-014-0171-9. |
| [6] | SAPP D G, CORMIER B M, ROCKWOOD K, et al. The frailty index based on laboratory test data as a tool to investigate the impact of frailty on health outcomes:a systematic review and meta-analysis[J]. Age Ageing, 2023, 52(1):afac309. doi:10.1093/ageing/afac309. |
| [7] | GU J J, LIU Q, ZHENG L J. A frailty assessment tool to predict in-hospital mortality in patients with acute exacerbations of chronic obstructive pulmonary disease[J]. Int J Chron Obstruct Pulmon Dis, 2021, 16:1093-1100. doi:10.2147/COPD.S300980. |
| [8] | HUANG S, WANG Y, CHEN L, et al. Use of a frailty index based upon routine laboratory data to predict complication and mortality in older community-acquired pneumonia patients[J]. Arch Gerontol Geriatr, 2022, 101:104692. doi:10.1016/j.archger.2022.104692. |
| [9] | 中华医学会呼吸病学分会. 中国成人社区获得性肺炎诊断和治疗指南(2016年版)[J]. 中华结核和呼吸杂志, 2016, 39(4):253-279. |
| Chinese Medical Association Respiratory Society. Guidelines for the diagnosis and treatment of community-acquired pneumonia in Chinese adults(2016 edition)[J]. Chin J Tuberc Respir Dis, 2016, 39(4):253-279. doi:10.3760/cma.j.issn.1001-0939.2016.04.005. | |
| [10] | ZAN Y M, ZHENG T P, WANG Y, et al. Combining a frailty index based on laboratory data and pneumonia severity assessments to predict in-hospital outcomes in older adults with community-acquired pneumonia[J]. J Nutr Health Aging, 2023, 27(4):270-276. doi:10.1007/s12603-023-1905-1. |
| [11] | IWAI-SAITO K, SHOBUGAWA Y, AIDA J, et al. Frailty is associated with susceptibility and severity of pneumonia in older adults (A JAGES multilevel cross-sectional study)[J]. Sci Rep, 2021, 11(1):7966. doi:10.1038/s41598-021-86854-3. |
| [12] | 齐丽, 田永红. 维生素D与社区获得性肺炎病情程度的相关性研究[J]. 天津医药, 2018, 46(11):1189-1192. |
| QI L, TIAN Y H. Association between vitamin D levels and the severity of community-acquired pneumonia[J]. Tianjin Med J, 2018, 46(11):1189-1192. doi:10.11958/20180961. | |
| [13] | KUNDI H, WADHERA R K, STROM J B, et al. Association of frailty with 30-day outcomes for acute myocardial infarction,heart Failure,and pneumonia among elderly adults[J]. JAMA Cardiol, 2019, 4(11):1084-1091. doi:10.1001/jamacardio.2019.3511. |
| [14] | DARVALL J N, BELLOMO R, BAILEY M, et al. Frailty and outcomes from pneumonia in critical illness:a population-based cohort study[J]. Br J Anaesth, 2020, 125(5):730-738. doi:10.1016/j.bja.2020.07.049. |
| [15] | YAMADA K, IWATA K, TACHIKAWA R, et al. Impact of physical frailty on the clinical outcomes of older patients hospitalized for pneumonia[J]. Geriatr Gerontol Int, 2021, 21(10):926-931. doi:10.1111/ggi.14262. |
| [16] | CILLÓNIZ C, DOMINEDÒ C, PERICÀS J M, et al. Community-acquired pneumonia in critically ill very old patients: a growing problem[J]. Eur Respir Rev, 2020, 29(155):190126. doi:10.1183/16000617.0126-2019. |
| [17] | GULLIFORD M C, CHARLTON J, WINTER J R, et al. Probability of sepsis after infection consultations in primary care in the United Kingdom in 2002-2017:population-based cohort study and decision analytic model[J]. PLoS Med, 2020, 17(7):e1003202. doi:10.1371/journal.pmed.1003202. |
| [18] | FERNANDO S M, GUO K H, LUKASIK M, et al. Frailty and associated prognosis among older emergency department patients with suspected infection:a prospective,observational cohort study[J]. CJEM, 2020, 22(5):687-691. doi:10.1017/cem.2020.377. |
| [19] | QUINTON L J, WALKEY A J, MIZGERD J P. Integrative physiology of pneumonia[J]. Physiol Rev, 2018, 98(3):1417-1464. doi:10.1152/physrev.00032.2017. |
| [20] | VERONESE N, STUBBS B, NOALE M, et al. Adherence to a mediterranean diet is associated with lower incidence of frailty:a longitudinal cohort study[J]. Clin Nutr, 2018, 37(5):1492-1497. doi:10.1016/j.clnu.2017.08.028. |
| [21] | CRUZ-JENTOFT A J, BAHAT G, BAUER J, et al. Sarcopenia:revised European consensus on definition and diagnosis[J]. Age Ageing, 2019, 48(1):16-31. doi:10.1093/ageing/afy169. |
| [22] | VETRANO D L, TRIOLO F, MAGGI S, et al. Fostering healthy aging:the interdependency of infections,immunity and frailty[J]. Ageing Res Rev, 2021, 69:101351. doi:10.1016/j.arr.2021.101351. |
| [23] | PRINA E, RANZANI O T, TORRES A. Community-acquired pneumonia[J]. Lancet, 2015, 386(9998):1097-1108. doi:10.1016/S0140-6736(15)60733-4. |
| [24] | BLODGETT J M, THEOU O, HOWLETT S E, et al. A frailty index from common clinical and laboratory tests predicts increased risk of death across the life course[J]. Geroscience, 2017, 39(4):447-455. doi:10.1007/s11357-017-9993-7. |
| [25] | KANE A E, KELLER K M, HEINZE-MILNE S, et al. A murine frailty index based on clinical and laboratory measurements:links between frailty and pro-inflammatory cytokines differ in a sex-specific manner[J]. J Gerontol A Biol Sci Med Sci, 2019, 74(3):275-282. doi:10.1093/gerona/gly117. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||