Tianjin Medical Journal ›› 2024, Vol. 52 ›› Issue (2): 182-187.doi: 10.11958/20230235
• Clinical Research • Previous Articles Next Articles
JIANG Hongyang( ), FAN Shiwen, LIU Tielong, XIE Liping△()
), FAN Shiwen, LIU Tielong, XIE Liping△()
Received:2023-02-27
Revised:2023-04-03
Published:2024-02-15
Online:2024-01-26
Contact:
△ E-mail: JIANG Hongyang, FAN Shiwen, LIU Tielong, XIE Liping. Effect of individualized PEEP combined with regular lung recruitment maneuvers on atelectasis after laparoscopic radical resection of colorectal cancer in elderly patients[J]. Tianjin Medical Journal, 2024, 52(2): 182-187.
CLC Number:
| 组别 | n | 年龄/岁 | 性别(男/女) | BMI/(kg/m2) | 吸烟史 |
|---|---|---|---|---|---|
| 对照组 | 31 | 72(67,76) | 20/11 | 23.7±2.7 | 15/14/2 |
| 试验组 | 31 | 74(70,79) | 15/16 | 23.5±2.4 | 19/11/1 |
| Z、χ2或t | 1.637 | 1.640 | 0.345 | 1.243 |
Tab.1 Comparison of age, gender, BMI and smoking history between the two groups
| 组别 | n | 年龄/岁 | 性别(男/女) | BMI/(kg/m2) | 吸烟史 |
|---|---|---|---|---|---|
| 对照组 | 31 | 72(67,76) | 20/11 | 23.7±2.7 | 15/14/2 |
| 试验组 | 31 | 74(70,79) | 15/16 | 23.5±2.4 | 19/11/1 |
| Z、χ2或t | 1.637 | 1.640 | 0.345 | 1.243 |
| 组别 | n | 高血压 | 糖尿病 | FEV1/FVC | Hb/(g/L) | ASA分级(Ⅰ/Ⅱ/Ⅲ) | ARISCAT评分(26~44/>44) |
|---|---|---|---|---|---|---|---|
| 对照组 | 31 | 13(41.9) | 4(12.9) | 74.9±7.9 | 120.8±14.4 | 4/24/3 | 8/23 |
| 试验组 | 31 | 16(51.6) | 7(22.6) | 77.6±8.0 | 117.5±12.9 | 3/23/5 | 11/20 |
| Z、χ2或t | 0.583 | 0.995 | 1.316 | 0.939 | 0.728 | 0.683 |
Tab.2 Comparison of preoperative general data between the two groups
| 组别 | n | 高血压 | 糖尿病 | FEV1/FVC | Hb/(g/L) | ASA分级(Ⅰ/Ⅱ/Ⅲ) | ARISCAT评分(26~44/>44) |
|---|---|---|---|---|---|---|---|
| 对照组 | 31 | 13(41.9) | 4(12.9) | 74.9±7.9 | 120.8±14.4 | 4/24/3 | 8/23 |
| 试验组 | 31 | 16(51.6) | 7(22.6) | 77.6±8.0 | 117.5±12.9 | 3/23/5 | 11/20 |
| Z、χ2或t | 0.583 | 0.995 | 1.316 | 0.939 | 0.728 | 0.683 |
| 组别 | n | PEEP/ cmH2O | 气腹时间/ min | 手术时间/ min | 苏醒时间/ min | 手术类型 (直肠癌/结肠癌) | 输液量/ mL | 估计失血量/ mL | 尿量/ mL |
|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 31 | 9(8,10) | 162(137,185) | 201(183,221) | 13.9±3.5 | 16/15 | 2 000(1 600,2 300) | 150(100,150) | 350(200,550) |
| 试验组 | 31 | 9(7,10) | 180(145,209) | 211(180,238) | 13.4±3.5 | 13/18 | 2 000(1 500,2 500) | 150(100,200) | 420(200,620) |
| Z、χ2或t | 0.857 | 1.352 | 0.514 | 0.647 | 0.583 | 0.542 | 0.670 | 0.789 |
Tab.3 Comparison of intraoperative data between the two groups
| 组别 | n | PEEP/ cmH2O | 气腹时间/ min | 手术时间/ min | 苏醒时间/ min | 手术类型 (直肠癌/结肠癌) | 输液量/ mL | 估计失血量/ mL | 尿量/ mL |
|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 31 | 9(8,10) | 162(137,185) | 201(183,221) | 13.9±3.5 | 16/15 | 2 000(1 600,2 300) | 150(100,150) | 350(200,550) |
| 试验组 | 31 | 9(7,10) | 180(145,209) | 211(180,238) | 13.4±3.5 | 13/18 | 2 000(1 500,2 500) | 150(100,200) | 420(200,620) |
| Z、χ2或t | 0.857 | 1.352 | 0.514 | 0.647 | 0.583 | 0.542 | 0.670 | 0.789 |
| 组别 | n | T0 | T3 | T4 |
|---|---|---|---|---|
| 对照组 | 31 | 0(0,2) | 10(8,10) | 9(8,11) |
| 试验组 | 31 | 1(0,2) | 8(6,9) | 6(5,8) |
| Z | 0.238 | 3.481** | 3.962** |
Tab.4 Comparison of LUS at different time points between the two groups
| 组别 | n | T0 | T3 | T4 |
|---|---|---|---|---|
| 对照组 | 31 | 0(0,2) | 10(8,10) | 9(8,11) |
| 试验组 | 31 | 1(0,2) | 8(6,9) | 6(5,8) |
| Z | 0.238 | 3.481** | 3.962** |
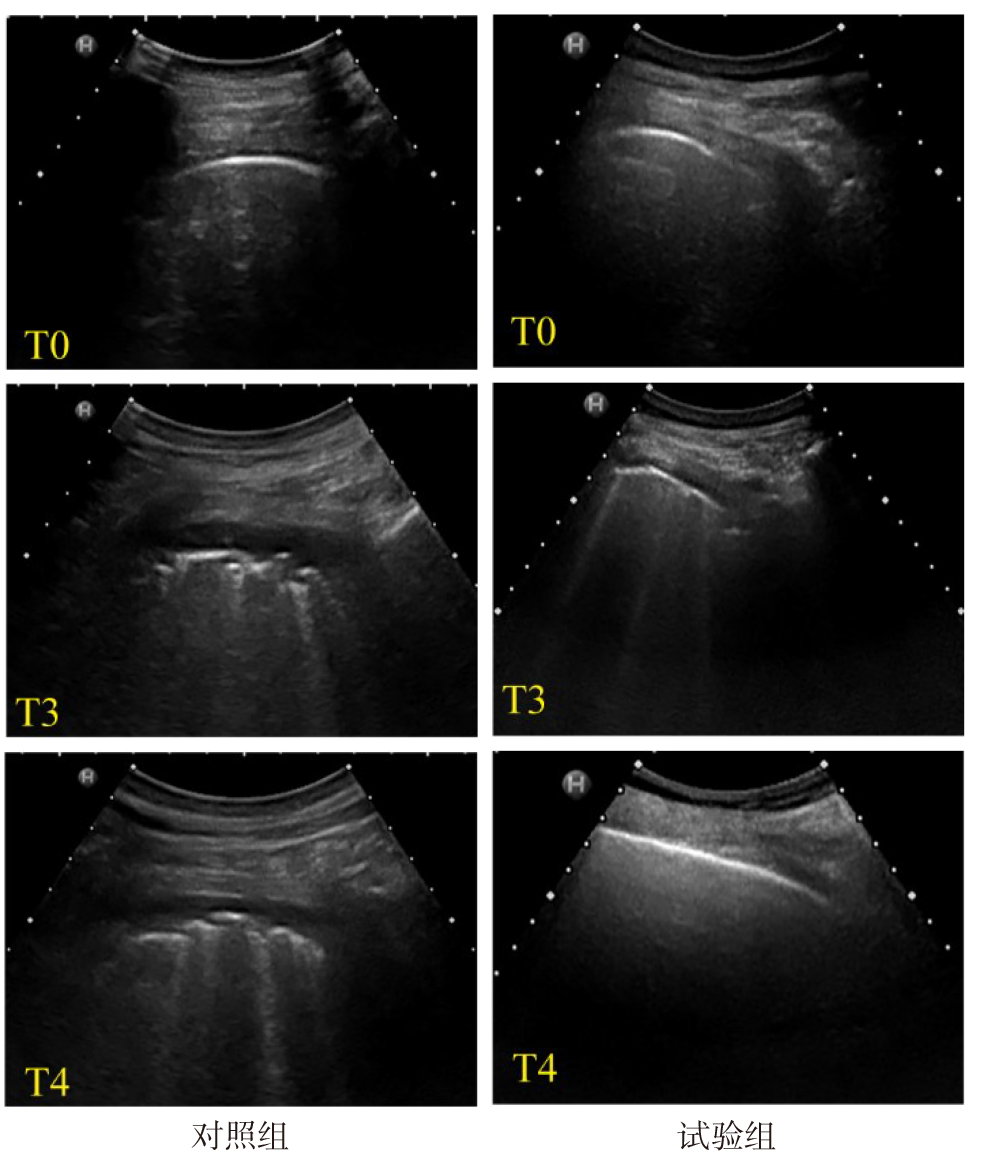
Fig.1 Lung ultrasound images of the posterior superior region of lung at different time points in the two groups
| 组别 | T1 | T2 | T3 |
|---|---|---|---|
| 对照组 | 24.9±3.9 | 22.4±3.3 | 35.5±7.7 |
| 试验组 | 24.1±3.6 | 24.2±3.8 | 39.7±6.7 |
| t | 0.894 | 2.033* | 2.273* |
Tab.5 Comparison of intraoperative Cdyn between the two groups
| 组别 | T1 | T2 | T3 |
|---|---|---|---|
| 对照组 | 24.9±3.9 | 22.4±3.3 | 35.5±7.7 |
| 试验组 | 24.1±3.6 | 24.2±3.8 | 39.7±6.7 |
| t | 0.894 | 2.033* | 2.273* |
| 组别 | T0 | T1 | |||
|---|---|---|---|---|---|
| 对照组 | 338.1±20.1 | 390.1±87.0 | |||
| 试验组 | 343.4±26.2 | 373.7±84.7 | |||
| t | 0.889 | 0.752 | |||
| 组别 | T2 | T3 | T4 | ||
| 对照组 | 392.5±64.1 | 398.8±54.0 | 329.1±22.4 | ||
| 试验组 | 435.9±69.3 | 462.6±57.5 | 338.9±30.3 | ||
| t | 2.560* | 4.508** | 1.444 | ||
Tab.6 Comparison of OI between the two groups
| 组别 | T0 | T1 | |||
|---|---|---|---|---|---|
| 对照组 | 338.1±20.1 | 390.1±87.0 | |||
| 试验组 | 343.4±26.2 | 373.7±84.7 | |||
| t | 0.889 | 0.752 | |||
| 组别 | T2 | T3 | T4 | ||
| 对照组 | 392.5±64.1 | 398.8±54.0 | 329.1±22.4 | ||
| 试验组 | 435.9±69.3 | 462.6±57.5 | 338.9±30.3 | ||
| t | 2.560* | 4.508** | 1.444 | ||
| 组别 | MAP/mmHg | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T4 | ||||||
| 对照组 | 90.1±9.1 | 85.8±9.7 | 87.1±8.8 | 89.6±7.8 | 91.2±9.2 | |||||
| 试验组 | 89.2±10.1 | 81.8±6.9 | 85.1±7.7 | 88.4±10.0 | 90.3±8.4 | |||||
| 组别 | HR/(次/min) | |||||||||
| T0 | T1 | T2 | T3 | T4 | ||||||
| 对照组 | 74.1±8.3 | 71.7±7.1 | 69.5±8.1 | 72.9±8.9 | 76.6±8.8 | |||||
| 试验组 | 77.0±10.6 | 72.1±10.0 | 69.2±9.2 | 74.0±8.8 | 79.2±10.5 | |||||
Tab.7 Comparison of MAP and HR between the two groups
| 组别 | MAP/mmHg | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T4 | ||||||
| 对照组 | 90.1±9.1 | 85.8±9.7 | 87.1±8.8 | 89.6±7.8 | 91.2±9.2 | |||||
| 试验组 | 89.2±10.1 | 81.8±6.9 | 85.1±7.7 | 88.4±10.0 | 90.3±8.4 | |||||
| 组别 | HR/(次/min) | |||||||||
| T0 | T1 | T2 | T3 | T4 | ||||||
| 对照组 | 74.1±8.3 | 71.7±7.1 | 69.5±8.1 | 72.9±8.9 | 76.6±8.8 | |||||
| 试验组 | 77.0±10.6 | 72.1±10.0 | 69.2±9.2 | 74.0±8.8 | 79.2±10.5 | |||||
| 组别 | n | 肺复张期间 低血压 | 术中血管活性药 总体使用 | PACU中低氧 饱和事件 |
|---|---|---|---|---|
| 对照组 | 31 | 2(6.5) | 17(54.8) | 10(32.3) |
| 试验组 | 31 | 6(19.4) | 20(64.5) | 3(9.7) |
| χ2 | 1.292 | 0.603 | 4.769* |
Tab.8 Comparison of the incidence of hypotension during RM, the overall use of vasoactive drugs during operation and the incidence of hypoxia saturation events in PACU between the two groups
| 组别 | n | 肺复张期间 低血压 | 术中血管活性药 总体使用 | PACU中低氧 饱和事件 |
|---|---|---|---|---|
| 对照组 | 31 | 2(6.5) | 17(54.8) | 10(32.3) |
| 试验组 | 31 | 6(19.4) | 20(64.5) | 3(9.7) |
| χ2 | 1.292 | 0.603 | 4.769* |
| 组别 | 咳嗽并咳痰 | 术后低氧血症 | 肺炎 | 肺不张 | 胸腔积液 |
|---|---|---|---|---|---|
| 对照组 | 10(32.3) | 2(6.5) | 1(3.2) | 4(12.9) | 5(16.1) |
| 试验组 | 13(41.9) | 0 | 0 | 2(6.5) | 2(6.5) |
| χ2或P | 0.622 | 0.517 | 0.999▲ | 0.185 | 0.644 |
Tab.9 Comparison of POPC within 7 days after surgery between the two groups
| 组别 | 咳嗽并咳痰 | 术后低氧血症 | 肺炎 | 肺不张 | 胸腔积液 |
|---|---|---|---|---|---|
| 对照组 | 10(32.3) | 2(6.5) | 1(3.2) | 4(12.9) | 5(16.1) |
| 试验组 | 13(41.9) | 0 | 0 | 2(6.5) | 2(6.5) |
| χ2或P | 0.622 | 0.517 | 0.999▲ | 0.185 | 0.644 |
| [1] | ZENG C, LAGIER D, LEE J W, et al. Perioperative pulmonary atelectasis:Part I. biology and mechanisms[J]. Anesthesiology(Philadelphia), 2022, 136(1):181. doi:10.1097/ALN.0000000000003943. |
| [2] | SHONO A, KATAYAMA N, FUJIHARA T, et al. Positive end-expiratory pressure and distribution of ventilation in pneumoperitoneum combined with steep trendelenburg position[J]. Anesthesiology, 2020, 132(3):476-490. doi:10.1097/ALN.0000000000003062. |
| [3] | LAGIER D, ZENG C, FERNANDEZ-BUSTAMANTE A, et al. Perioperative pulmonary atelectasis:Part II. clinical implications[J]. Anesthesiology, 2022, 136(1):206-236. doi:10.1097/ALN.0000000000004009. |
| [4] | FERNANDEZ-BUSTAMANTE A, FRENDL G, SPRUNG J, et al. Postoperative pulmonary complications,early mortality,and hospital stay following noncardiothoracic surgery:a multicenter study by the perioperative research network investigators[J]. JAMA Surg, 2017, 152(2):157-166. doi:10.1001/jamasurg.2016.4065. |
| [5] | 中华医学会麻醉学分会“围术期肺保护性通气策略临床应用专家共识”工作小组. 围术期肺保护性通气策略临床应用专家共识[J]. 中华麻醉学杂志, 2020, 40(5):513-519. |
| Chinese society of anesthesiology task force on clinical application of perioperative lung-protective ventilation strategies. Expert consensus on clinical application of perioperative lung-protective ventilation strategies[J]. Chin J Anesthesiol, 2020, 40(5):513-519. doi:10.3760/cma.j.cn131073.20200402.00501. | |
| [6] | YOUNG C C, HARRIS E M, VACCHIANO C, et al. Lung-protective ventilation for the surgical patient:International expert panel-based consensus recommendations[J]. Br J Anaesth, 2019, 123(6):898-913. doi:10.1016/j.bja.2019.08.017. |
| [7] | ZHOU L, LI H, LI M, et al. Individualized positive end-expiratory pressure guided by respiratory mechanics during anesthesia for the prevention of postoperative pulmonary complications:a systematic review and meta-analysis[J]. J Clin Monit Comput, 2023, 37(2):365-377. doi:10.1007/s10877-022-00960-9. |
| [8] | MONASTESSE A, GIRARD F, MASSICOTTE N, et al. Lung ultrasonography for the assessment of perioperative atelectasis:a pilot feasibility study[J]. Anesth Analg, 2017, 124(2):494-504. doi:10.1213/ANE.0000000000001603. |
| [9] | MINI G, RAY B R, ANAND R K, et al. Effect of driving pressure-guided positive end-expiratory pressure (PEEP) titration on postoperative lung atelectasis in adult patients undergoing elective major abdominal surgery:a randomized controlled trial[J]. Surgery, 2021, 170(1):277-283. doi:10.1016/j.surg.2021.01.047. |
| [10] | ÖSTBERG E, THORISSON A, ENLUND M, et al. Positive end-expiratory pressure alone minimizes atelectasis formation in nonabdominal surgery:a randomized controlled trial[J]. Anesthesiology, 2018, 128(6):1117-1124. doi:10.1097/ALN.0000000000002134. |
| [11] | UKERE A, MARZ A, WODACK K H, et al. Perioperative assessment of regional ventilation during changing body positions and ventilation conditions by electrical impedance tomography[J]. Br J Anaesth, 2016, 117(2):228-235. doi:10.1093/bja/aew188. |
| [12] | O'GARA B, TALMOR D. Perioperative lung protective ventilation[J]. BMJ, 2018, 362:k3030. doi:10.1136/bmj.k3030. |
| [13] | GÉNÉREUX V, CHASSÉ M, GIRARD F, et al. Effects of positive end-expiratory pressure/recruitment manoeuvres compared with zero end-expiratory pressure on atelectasis during open gynaecological surgery as assessed by ultrasonography:a randomised controlled trial[J]. Br J Anaesth, 2020, 124(1):101-109. doi:10.1016/j.bja.2019.09.040. |
| [14] | FRASSANITO L, SONNINO C, PITONI S, et al. Lung ultrasound to monitor the development of pulmonary atelectasis in gynecologic oncologic surgery[J]. Minerva Anestesiol, 2020, 86(12):1287-1295. doi:10.23736/S0375-9393.20.14687-X. |
| [15] | 刘彬彬, 温晓晖, 唐小芳, 等. 全麻人工气腹下老年患者肺不张发生的特点及其与膈肌抑制程度的关系[J]. 中华麻醉学杂志, 2021, 41(6):670-673. |
| LIU B B, WEN X H, TANG X F, et al. Characteristics of atelectasis and its relationship with degree of diaphragm inhibition in elderly patients with artificial pneumoperitoneum under general anesthesia[J]. Chin J Anesthesiol, 2021, 41(6):670-673. doi:10.3760/cma.j.cn131073.20201221.00608. | |
| [16] | JO Y Y, LEE K C, CHANG Y J, et al. Effects of an alveolar recruitment maneuver during lung protective ventilation on postoperative pulmonary complications in elderly patients undergoing laparoscopy[J]. Clin Interv Aging, 2020, 15:1461-1469. doi:10.2147/CIA.S264987. |
| [17] | GARCÍA-FERNÁNDEZ J, ROMERO A, BLANCO A, et al. Recruitment manoeuvres in anaesthesia:How many more excuses are there not to use them?[J]. Rev Esp Anestesiol Reanim (Engl Ed), 2018, 65(4):209-217. doi:10.1016/j.redar.2017.12.006. |
| [18] | WEI K, MIN S, CAO J, et al. Repeated alveolar recruitment maneuvers with and without positive end-expiratory pressure during bariatric surgery:a randomized trial[J]. Minerva Anestesiol, 2018, 84(4):463-472. doi:10.23736/S0375-9393.17.11897-3. |
| [19] | JUNG K, KIM S, KIM B J, et al. Comparison of positive end-expiratory pressure versus tidal volume-induced ventilator-driven alveolar recruitment maneuver in robotic prostatectomy:a randomized controlled study[J]. J Clin Med, 2021, 10(17):3921. doi:10.3390/jcm10173921. |
| [20] | SEVERAC M, CHIALI W, SEVERAC F, et al. Alveolar recruitment manoeuvre results in improved pulmonary function in obese patients undergoing bariatric surgery:a randomised trial[J]. Anaesth Crit Care Pain Med, 2021, 40(3):100775. doi:10.1016/j.accpm.2020.09.011. |
| [21] | ACOSTA C M, SARA T, CARPINELLA M, et al. Lung recruitment prevents collapse during laparoscopy in children:a randomised controlled trial[J]. Eur J Anaesthesiol, 2018, 35(8):573-580. doi:10.1097/EJA.0000000000000761. |
| [22] | COSTA L A, HAJJAR L A, VOLPE M S, et al. Effect of intensive vs moderate alveolar recruitment strategies added to lung-protective ventilation on postoperative pulmonary complications:a randomized clinical trial[J]. JAMA, 2017, 317(14):1422-1432. doi:10.1001/jama.2017.2297. |
| [23] | CUI Y, CAO R, LI G, et al. The effect of lung recruitment maneuvers on post-operative pulmonary complications for patients undergoing general anesthesia:a meta-analysis[J]. PLoS One, 2019, 14(5):e217405. doi:10.1371/journal.pone.0217405. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||