Tianjin Medical Journal ›› 2025, Vol. 53 ›› Issue (9): 993-999.doi: 10.11958/20251926
• New Technology • Previous Articles Next Articles
NIU Shulin1( ), WANG Zhouming1, LIU Mingyu1, GUAN Xin1, LI Mengqi2, TIAN Yikui2, YANG Zhenwen1, DU Xin1,△()
), WANG Zhouming1, LIU Mingyu1, GUAN Xin1, LI Mengqi2, TIAN Yikui2, YANG Zhenwen1, DU Xin1,△()
Received:2025-05-13
Revised:2025-06-10
Published:2025-09-15
Online:2025-09-16
Contact:
△E-mail: NIU Shulin, WANG Zhouming, LIU Mingyu, GUAN Xin, LI Mengqi, TIAN Yikui, YANG Zhenwen, DU Xin. Analysis of the safety and efficacy of transcatheter mitral valve-in-valve replacement for the bioprosthetic mitral valve failure[J]. Tianjin Medical Journal, 2025, 53(9): 993-999.
CLC Number:
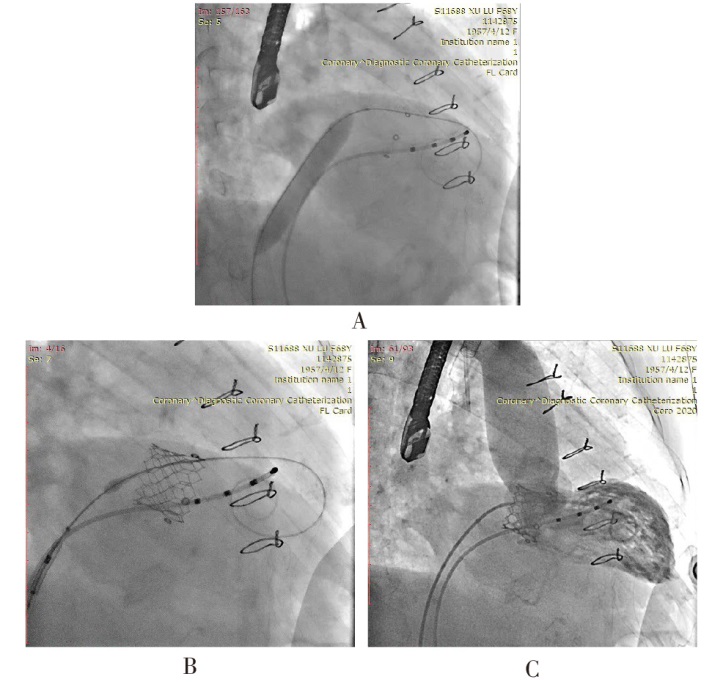
Fig.1 The interventional process of ViV-TMVR
| 组别 | n | 年龄/岁 | 男性 | BMI/ (kg/m2) | 生物瓣使用 年限/年 | 术前生物瓣 峰值流速/(m/s) | 平均跨瓣 压差/mmHg | LVEDD/mm | RA/mm | PASP/mmHg | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 国产组 | 10 | 71.80±5.88 | 6(60.0) | 23.20±2.15 | 12.60±3.10 | 2.79±0.46 | 15.38±5.42 | 48.90±5.41 | 48.40±7.69 | 61.40±19.02 | ||||||||
| 进口组 | 7 | 67.86±10.45 | 1(14.3) | 21.55±2.50 | 11.86±3.34 | 2.87±0.48 | 11.50±3.87 | 44.43±5.53 | 42.29±7.25 | 56.57±15.20 | ||||||||
| t或P | 0.997 | 0.134▲ | 1.452 | 0.472 | 0.309 | 1.263 | 1.663 | 1.650 | 0.557 | |||||||||
| 组别 | LVEF/% | STS评分/% | NYHAⅢ—Ⅳ级 | 高血压 | 冠心病 | 陈旧性脑梗死 | 心房颤动 | 糖尿病 | ||||||||||
| 国产组 | 64.00±3.83 | 6.54±1.03 | 9(90.0) | 4(40.0) | 3(30.0) | 1(10.0) | 4(40.0) | 3(30.0) | ||||||||||
| 进口组 | 63.86±2.48 | 6.34±1.41 | 6(85.7) | 2(28.6) | 1(14.3) | 1(14.3) | 4(57.1) | 1(14.3) | ||||||||||
| t或P | 0.086 | 0.341 | 1.000▲ | 1.000▲ | 0.603▲ | 1.000▲ | 0.637▲ | 0.603▲ | ||||||||||
Tab.1 Comparison of preoperative baseline data between the two groups of patients
| 组别 | n | 年龄/岁 | 男性 | BMI/ (kg/m2) | 生物瓣使用 年限/年 | 术前生物瓣 峰值流速/(m/s) | 平均跨瓣 压差/mmHg | LVEDD/mm | RA/mm | PASP/mmHg | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 国产组 | 10 | 71.80±5.88 | 6(60.0) | 23.20±2.15 | 12.60±3.10 | 2.79±0.46 | 15.38±5.42 | 48.90±5.41 | 48.40±7.69 | 61.40±19.02 | ||||||||
| 进口组 | 7 | 67.86±10.45 | 1(14.3) | 21.55±2.50 | 11.86±3.34 | 2.87±0.48 | 11.50±3.87 | 44.43±5.53 | 42.29±7.25 | 56.57±15.20 | ||||||||
| t或P | 0.997 | 0.134▲ | 1.452 | 0.472 | 0.309 | 1.263 | 1.663 | 1.650 | 0.557 | |||||||||
| 组别 | LVEF/% | STS评分/% | NYHAⅢ—Ⅳ级 | 高血压 | 冠心病 | 陈旧性脑梗死 | 心房颤动 | 糖尿病 | ||||||||||
| 国产组 | 64.00±3.83 | 6.54±1.03 | 9(90.0) | 4(40.0) | 3(30.0) | 1(10.0) | 4(40.0) | 3(30.0) | ||||||||||
| 进口组 | 63.86±2.48 | 6.34±1.41 | 6(85.7) | 2(28.6) | 1(14.3) | 1(14.3) | 4(57.1) | 1(14.3) | ||||||||||
| t或P | 0.086 | 0.341 | 1.000▲ | 1.000▲ | 0.603▲ | 1.000▲ | 0.637▲ | 0.603▲ | ||||||||||
| 组别 | n | 手术时间/min | 瓣中瓣瓣周 轻度反流 | 术后即刻瓣中瓣 峰值流速/(m/s) | 术后即刻瓣中瓣 平均跨瓣压差/mmHg | 术后ICU/CCU监护时间/h | 术后住院 时间/d | |||
|---|---|---|---|---|---|---|---|---|---|---|
| 国产组 | 10 | 251.50±24.04 | 3(30.0) | 1.43±0.28 | 2.90±1.10 | 17.30±8.46 | 5.50±3.50 | |||
| 进口组 | 7 | 234.28±42.86 | 1(14.3) | 1.63±0.28 | 3.86±1.95 | 15.93±15.10 | 5.29±1.70 | |||
| t或P | 1.062 | 0.603▲ | 1.389 | 1.295 | 0.240 | 0.149 | ||||
| 组别 | 术后30 d NYHA心功能分级Ⅲ—Ⅳ级 | 术后30 d瓣中瓣平均跨瓣压差/mmHg | 术后30 d瓣中瓣峰值流速/(m/s) | |||||||
| 国产组 | 2(22.2) | 5.63±1.51 | 1.85±0.26 | |||||||
| 进口组 | 3(50.0) | 5.00±2.83 | 2.18±0.48 | |||||||
| t或P | 0.596▲ | 0.458 | 1.746 | |||||||
Tab.2 Comparison of interventional therapy data between the two groups of patients
| 组别 | n | 手术时间/min | 瓣中瓣瓣周 轻度反流 | 术后即刻瓣中瓣 峰值流速/(m/s) | 术后即刻瓣中瓣 平均跨瓣压差/mmHg | 术后ICU/CCU监护时间/h | 术后住院 时间/d | |||
|---|---|---|---|---|---|---|---|---|---|---|
| 国产组 | 10 | 251.50±24.04 | 3(30.0) | 1.43±0.28 | 2.90±1.10 | 17.30±8.46 | 5.50±3.50 | |||
| 进口组 | 7 | 234.28±42.86 | 1(14.3) | 1.63±0.28 | 3.86±1.95 | 15.93±15.10 | 5.29±1.70 | |||
| t或P | 1.062 | 0.603▲ | 1.389 | 1.295 | 0.240 | 0.149 | ||||
| 组别 | 术后30 d NYHA心功能分级Ⅲ—Ⅳ级 | 术后30 d瓣中瓣平均跨瓣压差/mmHg | 术后30 d瓣中瓣峰值流速/(m/s) | |||||||
| 国产组 | 2(22.2) | 5.63±1.51 | 1.85±0.26 | |||||||
| 进口组 | 3(50.0) | 5.00±2.83 | 2.18±0.48 | |||||||
| t或P | 0.596▲ | 0.458 | 1.746 | |||||||
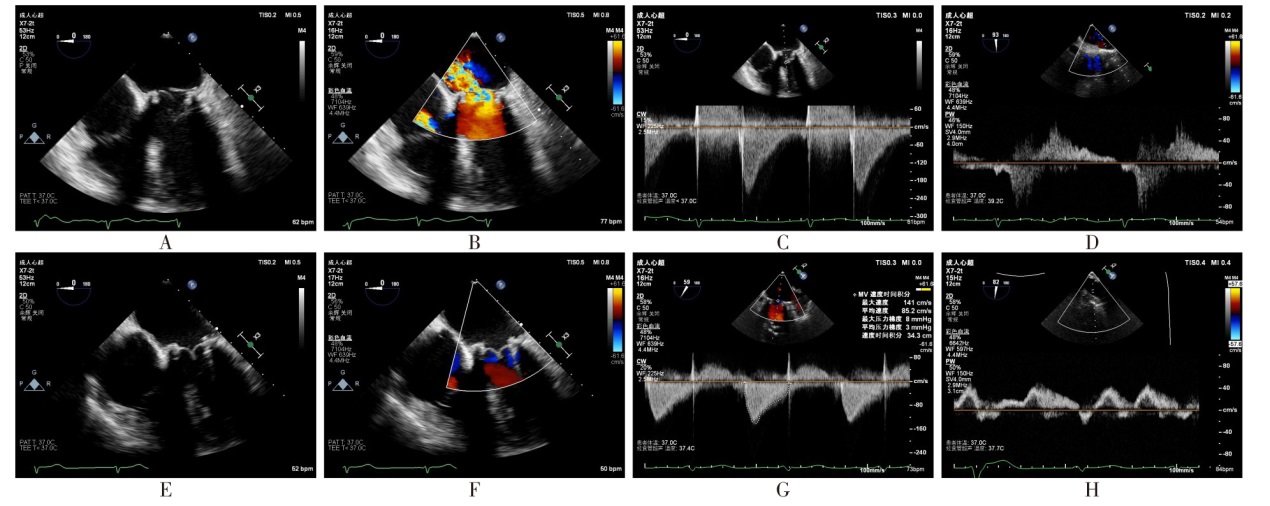
Fig.2 The real-time monitoring of TEE before and after ViV-TMVR
| 组别 | n | 生物瓣/瓣中瓣 峰值流速/(m/s) | 生物瓣/瓣中瓣平均跨瓣压差/mmHg | LVEF/% | |||
|---|---|---|---|---|---|---|---|
| 术前 | 17 | 2.81±0.47 | 15.29±6.42 | 64.38±2.80 | |||
| 术后即刻 | 17 | 1.49±0.30a | 3.00±1.15a | 59.25±4.83a | |||
| 术后30 d | 16 | 1.96±0.39ab | 5.86±1.68ab | 61.06±4.23a | |||
| F | 49.554** | 16.310** | 5.812* | ||||
| 组别 | LVEDD/mm | RA/mm | PASP/mmHg | ||||
| 术前 | 47.00±5.93 | 45.00±7.26 | 58.67±18.16 | ||||
| 术后即刻 | 45.63±4.66 | 45.37±7.39 | 42.07±14.58a | ||||
| 术后30 d | 45.88±3.52 | 43.06±7.44 | 41.80±14.05a | ||||
| F | 0.574 | 2.814 | 11.927** | ||||
Tab.3 Comparison of echocardiographic results before the operation, immediately after the operation and 30 days after the operation
| 组别 | n | 生物瓣/瓣中瓣 峰值流速/(m/s) | 生物瓣/瓣中瓣平均跨瓣压差/mmHg | LVEF/% | |||
|---|---|---|---|---|---|---|---|
| 术前 | 17 | 2.81±0.47 | 15.29±6.42 | 64.38±2.80 | |||
| 术后即刻 | 17 | 1.49±0.30a | 3.00±1.15a | 59.25±4.83a | |||
| 术后30 d | 16 | 1.96±0.39ab | 5.86±1.68ab | 61.06±4.23a | |||
| F | 49.554** | 16.310** | 5.812* | ||||
| 组别 | LVEDD/mm | RA/mm | PASP/mmHg | ||||
| 术前 | 47.00±5.93 | 45.00±7.26 | 58.67±18.16 | ||||
| 术后即刻 | 45.63±4.66 | 45.37±7.39 | 42.07±14.58a | ||||
| 术后30 d | 45.88±3.52 | 43.06±7.44 | 41.80±14.05a | ||||
| F | 0.574 | 2.814 | 11.927** | ||||
| [1] | CHEN C Y, LIN C P, HUNG K C, et al. Durability of biological valves implanted in aortic or mitral positions:a nationwide cohort study[J]. Ann Thorac Surg, 2023, 116(4):751-757. doi:10.1016/j.athoracsur.2023.05.038. |
| [2] | ZWISCHENBERGER B A, GACA J G, HANEY J C, et al. Late outcomes of porcine and pericardial bioprostheses after mitral valve replacement in 1162 patients[J]. Ann Thorac Surg, 2024, 118(4):882-888. doi:10.1016/j.athoracsur.2024.04.002. |
| [3] | BOURGUIGNON T, BOUQUIAUX-STABLO A L, LOARDI C, et al. Very late outcomes for mitral valve replacement with the Carpentier-Edwards pericardial bioprosthesis:25-year follow-up of 450 implantations[J]. J Thorac Cardiovasc Surg, 2014, 148(5):2004-2011.e1. doi:10.1016/j.jtcvs.2014.02.050. |
| [4] | MEHAFFEY H J, HAWKINS R B, SCHUBERT S, et al. Contemporary outcomes in reoperative mitral valve surgery[J]. Heart, 2018, 104(8):652-656. doi:10.1136/heartjnl-2017-312047. |
| [5] | EJIOFOR J I, HIRJI S A, RAMIREZ-DEL VAL F, et al. Outcomes of repeat mitral valve replacement in patients with prior mitral surgery:a benchmark for transcatheter approaches[J]. J Thorac Cardiovasc Surg, 2018, 156(2):619-627.e1. doi:10.1016/j.jtcvs.2018.03.126. |
| [6] | UEYAMA H A, MIYAMOTO Y, WATANABE A, et al. Cardiac reoperation or transcatheter mitral valve replacement for patients with failed mitral prostheses[J]. J Am Coll Cardiol, 2024, 83(2):317-330. doi:10.1016/j.jacc.2023.10.014. |
| [7] | TRUONG S, PETERSEN J, HAVERS-BORGERSEN E, et al. Outcomes of mitral valve reoperation and first-time surgery for mitral regurgitation:a nationwide study[J]. Int J Cardiol, 2025, 430:133175. doi:10.1016/j.ijcard.2025.133175. |
| [8] | ZUBAREVICH A, SZCZECHOWICZ M, ARJOMANDI RAD A, et al. Mitral surgical redo versus transapical transcatheter mitral valve implantation[J]. PLoS One, 2021, 16(8):e0256569. doi:10.1371/journal.pone.0256569. |
| [9] | GUERRERO M, PURSNANI A, NARANG A, et al. Prospective evaluation of transseptal TMVR for failed surgical bioprostheses:MITRAL trial valve-in-valve Arm 1-year outcomes[J]. JACC Cardiovasc Interv, 2021, 14(8):859-872. doi:10.1016/j.jcin.2021.02.027. |
| [10] | NASIR M M, AMIR S, SHAHID A, et al. Valve-in-valve transcatheter mitral valve replacement versus redo-surgical mitral valve replacement for degenerated bioprosthetic mitral valves:a systematic review and meta-analysis[J]. Int J Cardiol, 2024, 415:132448. doi:10.1016/j.ijcard.2024.132448. |
| [11] | COISNE A, LANCELLOTTI P, HABIB G, et al. ACC/AHA and ESC/EACTS guidelines for the management of valvular heart diseases:JACC Guideline Comparison[J]. J Am Coll Cardiol, 2023, 82(8):721-734. doi:10.1016/j.jacc.2023.05.061. |
| [12] | YOON S H, WHISENANT B K, BLEIZIFFER S, et al. Outcomes of transcatheter mitral valve replacement for degenerated bioprostheses,failed annuloplasty rings,and mitral annular calcification[J]. Eur Heart J, 2019, 40(5):441-451. doi:10.1093/eurheartj/ehy590. |
| [13] | ELEID M F, WHISENANT B K, CABALKA A K, et al. Early outcomes of percutaneous transvenous transseptal transcatheter valve implantation in failed bioprosthetic mitral valves,ring annuloplasty,and severe mitral annular calcification[J]. JACC Cardiovasc Interv, 2017, 10(19):1932-1942. doi:10.1016/j.jcin.2017.08.014. |
| [14] | PIRELLI L, HONG E, STEFFEN R, et al. Mitral valve-in-valve and valve-in-ring: tips, tricks,and outcomes[J]. Ann Cardiothorac Surg, 2021, 10(1):96-112. doi:10.21037/acs-2019-mv-169. |
| [15] | 张靖男, 万俊义, 宋会军, 等. 经导管“瓣中瓣”置换术治疗二尖瓣置换术后生物瓣衰败的疗效评价[J]. 中国循环杂志, 2023, 38(2):165-170. |
| ZHANG J N, WAN J Y, SONG H J, et al. Clinical efficacy of transcatheter mitral valve-in-valve replacement in patients with degenerated bioprosthesi[J]. Chinese Circulation Journal, 2023, 38(2):165-170. doi:10.3969/j.issn.1000-3614.2023.02.008. | |
| [16] | PIBAROT P, DUMESNIL J G, LEBLANC M H, et al. Changes in left ventricular mass and function after aortic valve replacement:a comparison between stentless and stented bioprosthetic valves[J]. J Am Soc Echocardiogr, 1999, 12(11):981-987. doi:10.1016/s0894-7317(99)70152-5. |
| [17] | AL-TAWIL M, BUTT S, REAP S, et al. Transseptal vs transapical transcatheter mitral valve-in-valve and valve-in-ring implantation:a systematic review and meta-analysis[J]. Curr Probl Cardiol, 2023, 48(7):101684. doi:10.1016/j.cpcardiol.2023.101684. |
| [18] | BAPAT V, MYDIN I, CHADALAVADA S, et al. A guide to fluoroscopic identification and design of bioprosthetic valves:a reference for valve-in-valve procedure[J]. Catheter Cardiovasc Interv, 2013, 81(5):853-861. doi:10.1002/ccd.24419. |
| [19] | SCHAMROTH PRAVDA N, MISHAEV R, LEVI A, et al. Five-year outcomes of patients with mitral structural valve deterioration treated with transcatheter valve in valve implantation - a single center prospective registry[J]. Front Cardiovasc Med, 2022, 9:883242. doi:10.3389/fcvm.2022.883242. |
| [20] | AKODAD M, TRPKOV C, CHEUNG A, et al. Valve-in-valve transcatheter mitral valve replacement:a large first-in-human 13-year experience[J]. Can J Cardiol, 2023, 39(12):1959-1970. doi:10.1016/j.cjca.2023.08.018. |
| [21] | GOEL K, MAKKAR R, KRISHNASWAMY A, et al. Contemporary outcomes and trends for the transseptal mitral valve-in-valve procedure using balloon expandable transcatheter valves in the United States[J]. Circulation, 2024, 150(19):1493-1504. doi:10.1161/CIRCULATIONAHA.124.068847. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||