天津医药 ›› 2026, Vol. 54 ›› Issue (1): 35-40.doi: 10.11958/20251377
楚兴( ), 刘磊, 杨华, 陈宏△()
), 刘磊, 杨华, 陈宏△()
收稿日期:2025-04-02
修回日期:2025-06-27
出版日期:2026-01-15
发布日期:2026-01-19
通讯作者:
△ E-mail:作者简介:楚兴(1992),男,主治医师,主要从事肝胆胰肿瘤的诊断及治疗方面研究。E-mail:基金资助:
CHU Xing(), LIU Lei, YANG Hua, CHEN Hong△()
Received:2025-04-02
Revised:2025-06-27
Published:2026-01-15
Online:2026-01-19
Contact:
△ E-mail:楚兴, 刘磊, 杨华, 陈宏. 胆总管结石并发急性胆源性胰腺炎的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 35-40.
CHU Xing, LIU Lei, YANG Hua, CHEN Hong. Risk factors and prediction model construction for acute biliary pancreatitis complicated with common bile duct stones[J]. Tianjin Medical Journal, 2026, 54(1): 35-40.
摘要:
目的 分析胆总管结石(CBDS)并发急性胆源性胰腺炎(ABP)的危险因素并构建预测模型。方法 纳入并发ABP的CBDS患者105例为ABP组,另纳入未并发ABP的CBDS患者105例为非ABP组。收集所有CBDS患者临床资料,通过多因素非条件Logistic回归分析CBDS并发ABP的危险因素,并据此构建CBDS并发ABP的列线图预测模型,H-L检验预测模型的拟合度;受试者工作特征(ROC)曲线分析预测模型的预测价值,C-index分析预测模型的区分能力,校准曲线分析预测模型的准确性,决策曲线分析预测模型的临床效益。结果 Logistic回归分析显示,年龄高、糖尿病、结石直径大、胆总管直径大、中性粒细胞/淋巴细胞比值(NLR)高、血淀粉酶(AMS)高、C反应蛋白(CRP)高为CBDS并发ABP的独立危险因素(P<0.05)。基于影响CBDS并发ABP的危险因素构建列线图预测模型,该预测模型H-L检验P>0.05。ROC曲线显示,该预测模型预测CBDS并发ABP的曲线下面积为0.884,C-index为0.884,校准曲线显示模型预测概率趋势接近理想曲线,决策曲线显示预测模型净收益范围较大。结论 基于CBDS并发ABP的危险因素构建的列线图预测模型具有良好的预测能效。
中图分类号:
| 组别 | 性别 | 年龄/岁 | 体质量指数/(kg/m2) | 基础疾病 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | 高脂血症 | 糖尿病 | 高血压 | |||||||||||||
| 非ABP组 | 65(61.90) | 40(38.10) | 54.60±7.00 | 22.43±1.97 | 34(32.38) | 10(9.52) | 40(38.10) | ||||||||||
| ABP组 | 60(57.14) | 45(42.86) | 59.74±5.87 | 22.81±1.85 | 38(36.19) | 31(29.52) | 42(40.00) | ||||||||||
| χ2或t | 0.494 | 5.769** | 1.421 | 0.338 | 13.366** | 0.080 | |||||||||||
| 组别 | 饮酒史 | 吸烟史 | 结石数量 | 结石直径/mm | 胆总管直径/mm | WBC/(×109/L) | |||||||||||
| 多发 | 单发 | ||||||||||||||||
| 非ABP组 | 25(23.81) | 44(41.90) | 41(39.05) | 64(60.95) | 6.18±2.24 | 11.26±2.03 | 8.12±2.79 | ||||||||||
| ABP组 | 27(25.71) | 50(47.62) | 56(53.33) | 49(46.67) | 7.58±2.04 | 12.15±1.73 | 8.52±2.44 | ||||||||||
| χ2或t | 0.102 | 0.693 | 4.311* | 4.755** | 3.442* | 1.117 | |||||||||||
| 组别 | Hb/(g/L) | PLT/(×109/L) | NLR | DBIL/(μmol/L) | IBIL/(μmol/L) | TBIL/(μmol/L) | |||||||||||
| 非ABP组 | 111.63±16.20 | 237.83±45.96 | 2.23±0.88 | 22.23±6.83 | 18.11±3.38 | 29.48±6.72 | |||||||||||
| ABP组 | 109.43±15.17 | 228.78±63.96 | 3.16±0.92 | 23.40±7.52 | 18.17±3.88 | 31.47±8.81 | |||||||||||
| t | 1.106 | 1.178 | 7.442** | 1.179 | 0.118 | 1.838 | |||||||||||
| 组别 | AST/(U/L) | ALT/(U/L) | AMS/(U/L) | ALB/(g/L) | Scr/(μmol/L) | BUN/(mmol/L) | CRP/(mg/L) | ||||||||||
| 非ABP组 | 52.01±6.56 | 55.25±7.28 | 129.30±22.26 | 40.46±5.13 | 73.36±12.06 | 5.26±1.18 | 9.74±3.02 | ||||||||||
| ABP组 | 52.06±8.13 | 55.66±7.86 | 149.34±31.66 | 39.22±5.04 | 73.56±11.95 | 5.28±1.29 | 12.36±3.43 | ||||||||||
| t | 0.052 | 0.396 | 5.308** | 1.766 | 0.120 | 0.112 | 5.853** | ||||||||||
表1 CBDS并发ABP的单因素分析
Tab.1 Univariate analysis of CBDS complicated with ABP (n=105)
| 组别 | 性别 | 年龄/岁 | 体质量指数/(kg/m2) | 基础疾病 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | 高脂血症 | 糖尿病 | 高血压 | |||||||||||||
| 非ABP组 | 65(61.90) | 40(38.10) | 54.60±7.00 | 22.43±1.97 | 34(32.38) | 10(9.52) | 40(38.10) | ||||||||||
| ABP组 | 60(57.14) | 45(42.86) | 59.74±5.87 | 22.81±1.85 | 38(36.19) | 31(29.52) | 42(40.00) | ||||||||||
| χ2或t | 0.494 | 5.769** | 1.421 | 0.338 | 13.366** | 0.080 | |||||||||||
| 组别 | 饮酒史 | 吸烟史 | 结石数量 | 结石直径/mm | 胆总管直径/mm | WBC/(×109/L) | |||||||||||
| 多发 | 单发 | ||||||||||||||||
| 非ABP组 | 25(23.81) | 44(41.90) | 41(39.05) | 64(60.95) | 6.18±2.24 | 11.26±2.03 | 8.12±2.79 | ||||||||||
| ABP组 | 27(25.71) | 50(47.62) | 56(53.33) | 49(46.67) | 7.58±2.04 | 12.15±1.73 | 8.52±2.44 | ||||||||||
| χ2或t | 0.102 | 0.693 | 4.311* | 4.755** | 3.442* | 1.117 | |||||||||||
| 组别 | Hb/(g/L) | PLT/(×109/L) | NLR | DBIL/(μmol/L) | IBIL/(μmol/L) | TBIL/(μmol/L) | |||||||||||
| 非ABP组 | 111.63±16.20 | 237.83±45.96 | 2.23±0.88 | 22.23±6.83 | 18.11±3.38 | 29.48±6.72 | |||||||||||
| ABP组 | 109.43±15.17 | 228.78±63.96 | 3.16±0.92 | 23.40±7.52 | 18.17±3.88 | 31.47±8.81 | |||||||||||
| t | 1.106 | 1.178 | 7.442** | 1.179 | 0.118 | 1.838 | |||||||||||
| 组别 | AST/(U/L) | ALT/(U/L) | AMS/(U/L) | ALB/(g/L) | Scr/(μmol/L) | BUN/(mmol/L) | CRP/(mg/L) | ||||||||||
| 非ABP组 | 52.01±6.56 | 55.25±7.28 | 129.30±22.26 | 40.46±5.13 | 73.36±12.06 | 5.26±1.18 | 9.74±3.02 | ||||||||||
| ABP组 | 52.06±8.13 | 55.66±7.86 | 149.34±31.66 | 39.22±5.04 | 73.56±11.95 | 5.28±1.29 | 12.36±3.43 | ||||||||||
| t | 0.052 | 0.396 | 5.308** | 1.766 | 0.120 | 0.112 | 5.853** | ||||||||||
| 变量 | β | SE | Wald χ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| 年龄 | 1.054 | 0.293 | 12.928 | <0.001 | 2.869 | 1.615~5.095 |
| 糖尿病 | 1.482 | 0.290 | 26.160 | <0.001 | 4.400 | 2.494~7.763 |
| 结石数量 | 1.291 | 0.721 | 3.207 | 0.073 | 3.638 | 0.885~14.950 |
| 结石直径 | 0.550 | 0.243 | 5.111 | 0.024 | 1.733 | 1.073~2.793 |
| 胆总管直径 | 0.584 | 0.253 | 5.345 | 0.021 | 1.794 | 1.093~2.944 |
| NLR | 1.318 | 0.264 | 24.990 | <0.001 | 3.738 | 2.229~6.267 |
| AMS | 0.880 | 0.246 | 12.798 | <0.001 | 2.412 | 1.489~3.907 |
| CRP | 1.124 | 0.255 | 19.503 | <0.001 | 3.077 | 1.869~5.068 |
| 常量 | -5.890 | 0.494 | 142.449 | <0.001 | 0.000 | - |
表2 CBDS并发ABP的多因素非条件Logistic回归分析
Tab.2 Multivariate unconditional Logistic regression analysis of CBDS complicated with ABP
| 变量 | β | SE | Wald χ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| 年龄 | 1.054 | 0.293 | 12.928 | <0.001 | 2.869 | 1.615~5.095 |
| 糖尿病 | 1.482 | 0.290 | 26.160 | <0.001 | 4.400 | 2.494~7.763 |
| 结石数量 | 1.291 | 0.721 | 3.207 | 0.073 | 3.638 | 0.885~14.950 |
| 结石直径 | 0.550 | 0.243 | 5.111 | 0.024 | 1.733 | 1.073~2.793 |
| 胆总管直径 | 0.584 | 0.253 | 5.345 | 0.021 | 1.794 | 1.093~2.944 |
| NLR | 1.318 | 0.264 | 24.990 | <0.001 | 3.738 | 2.229~6.267 |
| AMS | 0.880 | 0.246 | 12.798 | <0.001 | 2.412 | 1.489~3.907 |
| CRP | 1.124 | 0.255 | 19.503 | <0.001 | 3.077 | 1.869~5.068 |
| 常量 | -5.890 | 0.494 | 142.449 | <0.001 | 0.000 | - |
| 指标 | 年龄 | 糖尿病 | 结石直径 | 胆总管直径 | NLR | AMS | CRP |
|---|---|---|---|---|---|---|---|
| 年龄 | - | 1.292 | 0.060 | 0.416 | 0.001 | 0.130 | 0.551 |
| 糖尿病 | 1.292 | - | 0.056 | 0.056 | 1.926 | 0.147 | 1.178 |
| 结石直径 | 0.060 | 0.056 | - | 0.086 | 0.394 | 1.113 | 0.676 |
| 胆总管直径 | 0.416 | 0.056 | 0.086 | - | 0.111 | 0.715 | 0.591 |
| NLR | 0.001 | 1.926 | 0.394 | 0.111 | - | 0.224 | 0.909 |
| AMS | 0.130 | 0.147 | 1.113 | 0.715 | 0.224 | - | 1.713 |
| CRP | 0.551 | 1.178 | 0.676 | 0.591 | 0.909 | 1.713 | - |
表3 交互项检验
Tab.3 Analysis of interaction terms (χ2)
| 指标 | 年龄 | 糖尿病 | 结石直径 | 胆总管直径 | NLR | AMS | CRP |
|---|---|---|---|---|---|---|---|
| 年龄 | - | 1.292 | 0.060 | 0.416 | 0.001 | 0.130 | 0.551 |
| 糖尿病 | 1.292 | - | 0.056 | 0.056 | 1.926 | 0.147 | 1.178 |
| 结石直径 | 0.060 | 0.056 | - | 0.086 | 0.394 | 1.113 | 0.676 |
| 胆总管直径 | 0.416 | 0.056 | 0.086 | - | 0.111 | 0.715 | 0.591 |
| NLR | 0.001 | 1.926 | 0.394 | 0.111 | - | 0.224 | 0.909 |
| AMS | 0.130 | 0.147 | 1.113 | 0.715 | 0.224 | - | 1.713 |
| CRP | 0.551 | 1.178 | 0.676 | 0.591 | 0.909 | 1.713 | - |
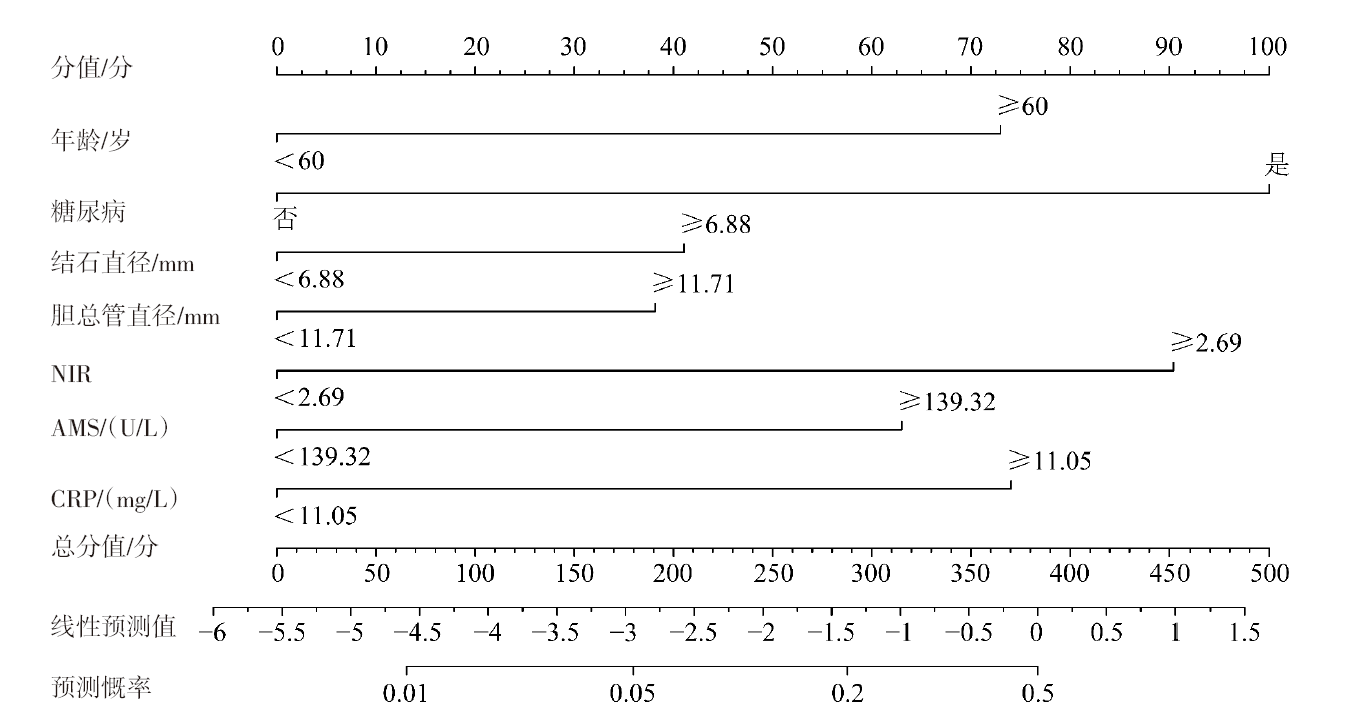
图1 CBDS并发ABP的列线图
Fig.1 Nomogram for CBDS complicated with ABP
| 指标 | AUC | 95%CI | 截断值 | 敏感度 | 特异度 | 约登 指数 |
|---|---|---|---|---|---|---|
| 年龄 | 0.665 | 0.630~0.698 | 65岁 | 0.552 | 0.712 | 0.265 |
| 糖尿病 | 0.598 | 0.563~0.633 | 是 | 0.295 | 0.901 | 0.196 |
| 结石直径 | 0.633 | 0.598~0.667 | 5.37 mm | 0.886 | 0.310 | 0.196 |
| 胆总管直径 | 0.628 | 0.593~0.662 | 11.49 mm | 0.714 | 0.511 | 0.226 |
| NLR | 0.721 | 0.688~0.752 | 2.63 | 0.752 | 0.601 | 0.354 |
| AMS | 0.691 | 0.657~0.723 | 150.98 U/L | 0.486 | 0.880 | 0.366 |
| CRP | 0.674 | 0.640~0.707 | 12.01 mg/L | 0.610 | 0.679 | 0.289 |
| 列线图模型 | 0.884 | 0.859~0.906 | 0.22 | 0.733 | 0.903 | 0.636 |
表4 各变量及列线图预测CBDS并发ABP的价值
Tab.4 Predictive value of each variable and the nomogram for CBDS complicated with ABP
| 指标 | AUC | 95%CI | 截断值 | 敏感度 | 特异度 | 约登 指数 |
|---|---|---|---|---|---|---|
| 年龄 | 0.665 | 0.630~0.698 | 65岁 | 0.552 | 0.712 | 0.265 |
| 糖尿病 | 0.598 | 0.563~0.633 | 是 | 0.295 | 0.901 | 0.196 |
| 结石直径 | 0.633 | 0.598~0.667 | 5.37 mm | 0.886 | 0.310 | 0.196 |
| 胆总管直径 | 0.628 | 0.593~0.662 | 11.49 mm | 0.714 | 0.511 | 0.226 |
| NLR | 0.721 | 0.688~0.752 | 2.63 | 0.752 | 0.601 | 0.354 |
| AMS | 0.691 | 0.657~0.723 | 150.98 U/L | 0.486 | 0.880 | 0.366 |
| CRP | 0.674 | 0.640~0.707 | 12.01 mg/L | 0.610 | 0.679 | 0.289 |
| 列线图模型 | 0.884 | 0.859~0.906 | 0.22 | 0.733 | 0.903 | 0.636 |
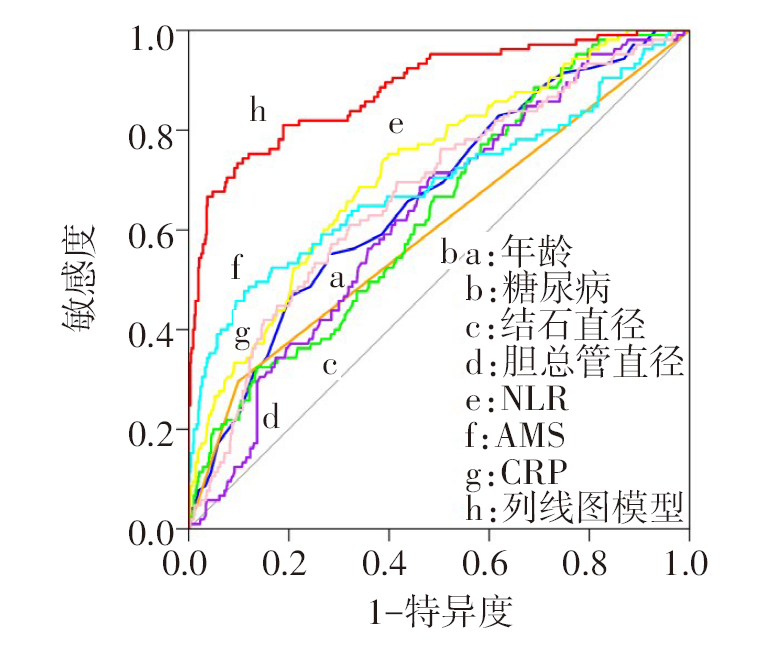
图2 各指标及预测模型预测CBDS并发ABP的ROC曲线
Fig.2 ROC curves of each indicator and the predictive model for CBDS complicated with ABP
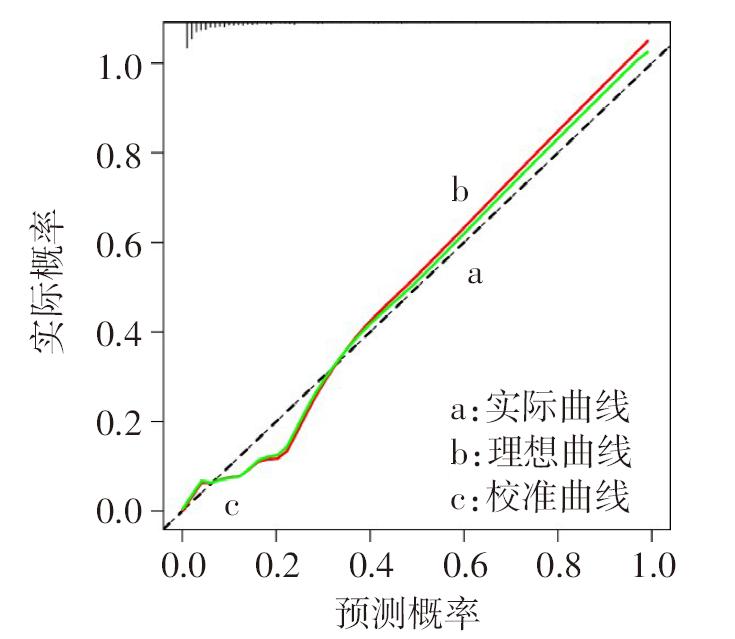
图3 预测模型预测CBDS并发ABP的校准曲线
Fig.3 Calibration curve of the predictive model for CBDS complicated with ABP
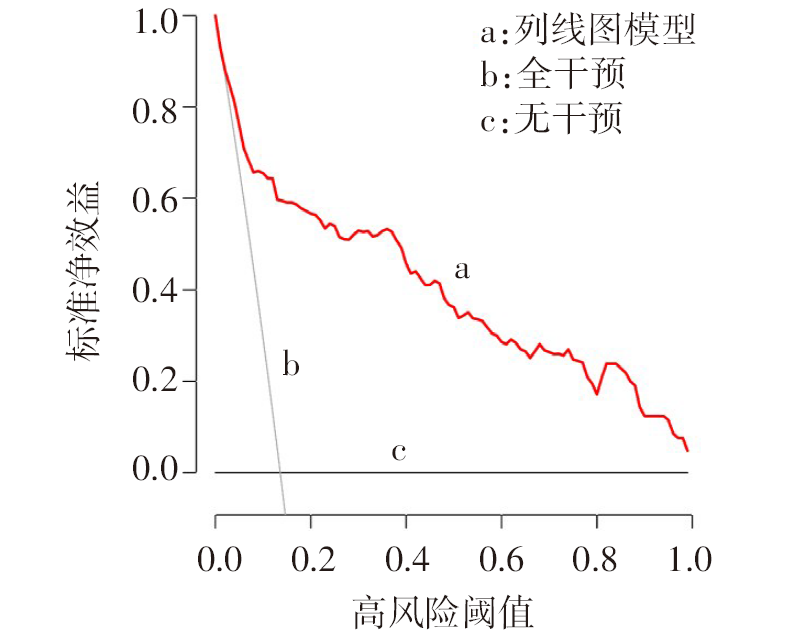
图4 预测模型预测CBDS并发ABP的决策曲线
Fig.4 Decision curve of the predictive model for CBDS complicated with ABP
| [1] | 张井虹, 尚海涛, 刘军舰, 等. 继发性胆总管结石外科治疗策略研究[J]. 天津医药, 2021, 49(5):505-509. |
| ZHANG J H, SHANG H T, LIU J J, et al. Study on surgical treatment strategy for secondary choledocholithiasis[J]. Tianjin Med J, 2021, 49(5):505-509. doi:10.11958/20203545. | |
| [2] | 中华中医药学会《重症急性胰腺炎中西医结合诊疗指南》起草组. 重症急性胰腺炎中西医结合诊疗指南[J]. 临床肝胆病杂志, 2024, 40(6):1114-1125. |
| Drafting Group of Guidelines for Integrated Traditional Chinese and Western Medicine Diagnosis and Treatment of Severe Acute Pancreatitis,Chinese Association of Traditional Chinese Medicine. Guidelines for integrated traditional Chinese and western medicine diagnosis and treatment of severe acute pancreatitis[J]. J Clin Hepatol, 2024, 40(6):1114-1125. doi:10.12449/JCH240608. | |
| [3] | LAI T, LI J, ZHOU Z, et al. Etiological changes and prognosis of hospitalized patients with acute pancreatitis over a 15-year period[J]. Dig Dis Sci, 2024, 69(1):56-65. doi:10.1007/s10620-023-08172-0. |
| [4] | WANG X, YU W, JIANG G, et al. Global epidemiology of gallstones in the 21st century:a systematic review and meta-analysis[J]. Clin Gastroenterol Hepatol, 2024, 22(8):1586-1595. doi:10.1016/j.cgh.2024.01.051. |
| [5] | 中国中西医结合学会消化系统疾病专业委员会. 胆石症中西医结合诊疗共识意见(2017年)[J]. 中国中西医结合消化杂志, 2018, 26(2):132-138. |
| Chinese Society of Integrated Traditional Chinese and Western Medicine,Digestive Diseases Specialty Committee. Consensus opinions on integrated traditional Chinese and western medicine diagnosis and treatment of cholelithiasis(2017)[J]. Chin J Integr Trad West Med Dig, 2018, 26(2):132-138. doi:10.3969/j.issn.1671-038X.2018.02.04. | |
| [6] | 中华医学会外科学分会胰腺外科学组. 中国急性胰腺炎诊治指南(2021)[J]. 中华外科杂志, 2021, 59(7):578-587. |
| Chinese Pancreatic Surgery Association,Chinese Society of Surgery,Chinese Medical Association. Guidelines for diagnosis and treatment of acute pancreatitis in China(2021)[J]. Chin J Surg, 2021, 59(7):578-587. doi:10.3760/cma.j.cn112139-20210416-00172. | |
| [7] | 张雅男, 王奥, 张莉, 等. 急性胆石性胰腺炎病因学的研究进展[J]. 中华肝胆外科杂志, 2024, 30(2):156-160. |
| ZHANG Y N, WANG A, ZHANG L, et al. Research progress in etiology of acute gallstone pancreatitis[J]. Chin J Hepatobiliary Surg, 2024, 30(2):156-160. doi:10.3760/cma.j.cn113884-20230907-00064. | |
| [8] | GUPTA V, ABHINAV A, VUTHALURU S, et al. The multifaceted impact of gallstones:understanding complications and management strategies[J]. Cureus, 2024, 16(6):e62500. doi:10.7759/cureus.62500. |
| [9] | 韦慧芬, 唐国都, 梁志海, 等. 不同年龄段人群发生急性胰腺炎的临床特点回顾分析[J]. 世界华人消化杂志, 2019, 27(10):624-631. |
| WEI H F, TANG G D, LIANG Z H, et al. Clinical features of acute pancreatitis in people of different age groups:a retrospective analysis[J]. Shijie Huaren Xiaohua Zazhi, 2019, 27(10):624-631. doi:10.11569/wcjd.v27.i10.624. | |
| [10] | HERRERA-LEBLANC I D, DOMÍNGUEZ-HERNÁNDEZ M F, PALACIOS-SAUCEDO G C, et al. Common bile duct diameter by age groups in adult patients without bile duct pathology[J]. Cir Cir, 2022, 90(4):503-507. doi:10.24875/CIRU.20001391. |
| [11] | 林锐, 施宝民. 老年急性胰腺炎的诊疗进展[J]. 老年医学与保健, 2022, 28(1):4-7. |
| LIN R, SHI B M. Advances in diagnosis and treatment of acute pancreatitis in the elderly[J]. Geriatr Health Care, 2022, 28(1):4-7. doi:10.3969/j.issn.1008-8296.2022.01.002. | |
| [12] | RATHEESH R, ULRICH M T, GHOZY S, et al. The association between diabetes and gallstones:a nationwide population-based cohort study[J]. Prz Gastroenterol, 2023, 18(3):292-299. doi:10.5114/pg.2023.131395. |
| [13] | KHOURY T, SBEIT W. Diabetes mellitus is associated with a higher rate of acute cholangitis among patients with common bile duct stones:a retrospective study[J]. Medicine (Baltimore), 2022, 101(4):e28687. doi:10.1097/MD.0000000000028687. |
| [14] | CHUNG K H, CHO I R, CHOI Y H, et al. Association between diabetic status and risk of acute pancreatitis:a nationwide population-based study[J]. J Evid Based Med, 2024, 17(3):588-596. doi:10.1111/jebm.12637. |
| [15] | GUO X, LI Y, LIN H, et al. A nomogram for clinical estimation of acute biliary pancreatitis risk among patients with symptomatic gallstones:a retrospective case-control study[J]. Front Cell Infect Microbiol, 2022,12:935927. doi:10.3389/fcimb.2022.935927. |
| [16] | 郑冰峰, 刘建生. 胆源性急性胰腺炎与高脂血症性急性胰腺炎临床特点比较的研究进展[J]. 国际消化病杂志, 2020, 40(3):157-160. |
| ZHENG B F, LIU J S. Progress in comparative study of clinical features between biliary acute pancreatitis and hyperlipidemic acute pancreatitis[J]. Int J Dig Dis, 2020, 40(3):157-160. doi:10.3969/j.issn.1673-534X.2020.03.005. | |
| [17] | 李启元, 罗岩, 孙备. 急性胆源性胰腺炎诊治策略[J]. 肝胆外科杂志, 2023, 31(6):405-408. |
| LI Q Y, LUO Y, SUN B. Diagnosis and treatment strategies for acute biliary pancreatitis[J]. J Hepatobiliary Surg, 2023, 31(6):405-408. doi:10.3969/j.issn.1006-4761.2023.06.003. | |
| [18] | 陆颖超, 黄锦山, 徐红星, 等. 胆囊结石患者并发急性胆源性胰腺炎的影响因素分析及列线图预测模型构建[J]. 中国普通外科杂志, 2023, 32(8):1199-1207. |
| LU Y C, HUANG J S, XU H X, et al. Analysis of influencing factors for acute biliary pancreatitis in patients with cholecystolithiasis and construction of nomogram prediction model[J]. Chin J Gen Surg, 2023, 32(8):1199-1207. doi:10.7659/j.issn.1005-6947.2023.08.008. | |
| [19] | 刘涛, 刘悦泽, 张太平. 急性胰腺炎基础及临床转化研究进展[J]. 中国实用外科杂志, 2024, 44(5):594-597,600. |
| LIU T, LIU Y Z, ZHANG T P. Advancements in both basic and clinical translational research on acute pancreatitis[J]. Chin J Pract Surg, 2024, 44(5):594-597,600. doi:10.19538/j.cjps.issn1005-2208.2024.05.21. | |
| [20] | 彭凯新, 文礼. 急性胰腺炎的发病机制研究进展及未来展望[J]. 西安交通大学学报(医学版), 2024, 45(2):167-177. |
| PENG K X, WEN L. Research progress and future prospect on the pathogenesis of acute pancreatitis[J]. Journal of Xi’an Jiaotong University (Medical Sciences), 2024, 45(2):167-177. doi:10.7652/jdyxb202402001. | |
| [21] | 王田, 白毅, 赵静, 等. 全身炎症指数和预后营养指数对重度胰腺炎的早期诊断价值[J]. 检验医学, 2024, 39(6):598-601. |
| WANG T, BAI Y, ZHAO J, et al. Early diagnostic value of systemic inflammatory index and prognostic nutritional index in severe pancreatitis[J]. Laboratory Medicine, 2024, 39(6):598-601. doi:10.3969/j.issn.1673-8640.2024.06.015. | |
| [22] | 中国妇幼保健协会临床诊断与实验医学分会. 中国儿童全血C反应蛋白检测系统性能评价标准建立专家共识[J]. 检验医学, 2021, 36(12):1201-1205. |
| Clinical Diagnosis and Laboratory Medicine Branch of China Maternal and Child Health Association. Expert consensus on establishment of standards for the performance evaluation of systems for whole blood C-reactive protein determination of Chinese children[J]. Laboratory Medicine, 2021, 36(12):1201-1205. doi:10.3969/j.issn.1673-8640.2021.012.001. | |
| [23] | 王庆, 夏婷婷. 未成熟粒细胞计数、C反应蛋白、中性粒细胞/淋巴细胞、降钙素原结合MCTSI评分在急性胆源性胰腺炎中的诊断价值[J]. 中华消化病与影像杂志(电子版), 2023, 13(4):224-228. |
| WANG Q, XIA T T. Diagnostic value of immature granulocyte count,C-reactive protein,NLR,PCT combined with MCTSI score in acute biliary pancreatitis[J]. Chin J Digest Dis Med Imageol(Electronic Edition), 2023, 13(4):224-228. doi:10.3877/cma.j.issn.2095-2015.2023.04.007. |
| [1] | 李斌, 谭振刚, 张华清. 基于息肉特征和血清学指标构建结直肠息肉复发风险预测模型及效能分析[J]. 天津医药, 2026, 54(3): 249-253. |
| [2] | 朱海燕, 王烨, 尹艳. 老年NSCLC患者术后胃肠功能紊乱的危险因素研究[J]. 天津医药, 2026, 54(3): 289-294. |
| [3] | 刘晓华, 韩婷婷, 高玉杰. 增强CT淋巴结边缘特征联合IPI对难治性弥漫大B细胞巴瘤的预测价值[J]. 天津医药, 2026, 54(3): 303-308. |
| [4] | 陈丽, 陈楠. COPD进展为Ⅱ型呼吸衰竭预警模型的建立与验证[J]. 天津医药, 2026, 54(2): 189-195. |
| [5] | 程云, 夏明农, 张帆, 李凤. 小儿热性惊厥发展为癫痫的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 52-57. |
| [6] | 陈敏, 夏莉, 朱荣媛, 王欣雨, 季骏. 拔除第一前磨牙正畸治疗后牙龈内陷的危险因素及预测模型的构建[J]. 天津医药, 2026, 54(1): 57-63. |
| [7] | 李贺, 马胜山, 孙阳, 武栋泽, 李小飞. 关节镜肩袖修补术后再撕裂风险的影响因素及预测模型构建[J]. 天津医药, 2026, 54(1): 64-69. |
| [8] | 周利军, 曾文静, 胡琴. 哌拉西林他唑巴坦致低钾血症的危险因素分析[J]. 天津医药, 2025, 53(9): 937-941. |
| [9] | 陈慧, 赵凯, 刘振国, 常瑛, 巨康璐. 金丝桃素通过调控NLRP3炎症小体改善小鼠急性胰腺炎的机制探讨[J]. 天津医药, 2025, 53(8): 820-825. |
| [10] | 刘志远, 杨声飞, 钱释然, 邓忆莲, 黎东伟, 李君久. 胸乳入路腔镜甲状腺术后早期低钙血症的危险因素分析及预测模型构建[J]. 天津医药, 2025, 53(8): 826-830. |
| [11] | 刘鹏勇, 刘梦友, 周昱, 管海, 田振, 胡浩, 岳晓松, 关倩楠. 甲状腺全切术后并发永久性甲状旁腺功能减退的危险因素及列线图建立[J]. 天津医药, 2025, 53(8): 850-855. |
| [12] | 金吴娟, 倪刚, 黄欣宇, 王羊洋. 老年消化道出血患者不良预后的列线图预测模型的构建与验证[J]. 天津医药, 2025, 53(7): 694-699. |
| [13] | 陈英, 郭长英, 张静, 李娟, 陈丰毅. 基于术前肺动脉压评估心脏移植术后右心衰竭的发生风险[J]. 天津医药, 2025, 53(7): 751-755. |
| [14] | 李建林, 孙思进, 王大力. Ⅰ—Ⅱ期非小细胞肺癌胸腔镜术后心肺并发症的影响因素及预测模型构建[J]. 天津医药, 2025, 53(6): 583-588. |
| [15] | 陈珍进, 金晓青, 祁安宁, 韩崇旭. 血浆血管性血友病因子抗原水平对老年急性心肌梗死患者长期预后的预测价值[J]. 天津医药, 2025, 53(6): 589-593. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||