Tianjin Medical Journal ›› 2025, Vol. 53 ›› Issue (6): 619-624.doi: 10.11958/20241860
• Clinical Research • Previous Articles Next Articles
DU Yunze( ), TANG Qiong
), TANG Qiong
Received:2024-11-18
Revised:2025-04-08
Published:2025-06-15
Online:2025-06-20
DU Yunze, TANG Qiong. The clinical value of the combination of routine pleural effusion and serum assay in distinguishing tuberculous pleural effusion from malignant pleural effusion[J]. Tianjin Medical Journal, 2025, 53(6): 619-624.
CLC Number:
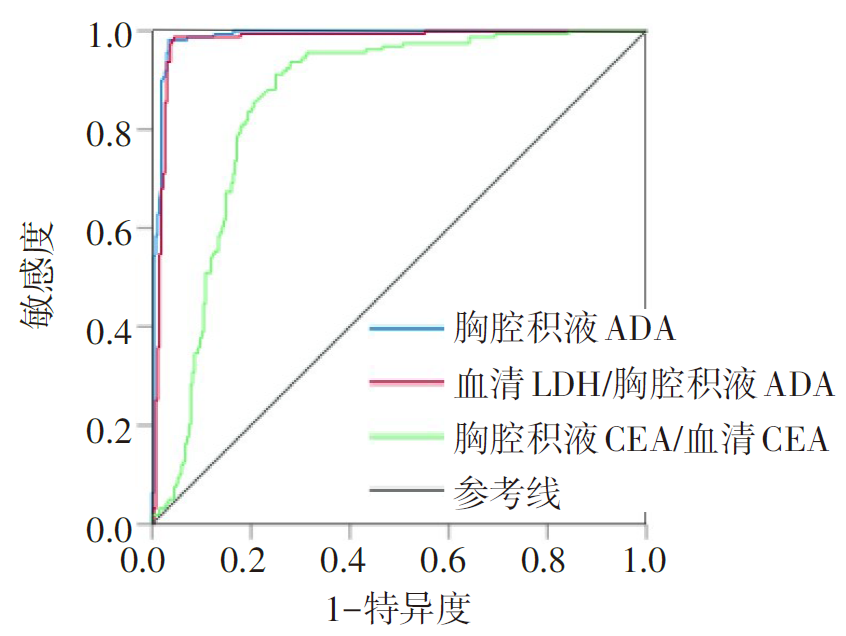
Fig.1 ROC curve of pleural effusion ADA, serum LDH/ pleural effusion ADA and pleural effusion CEA/ serum CEA in diagnosis of tuberculous pleural effusion
| 参数 | AUC | 95%CI | 截断值 | 敏感度/% | 特异度/% |
|---|---|---|---|---|---|
| 胸腔积液ADA | 0.988 | 0.978~0.997 | 29.700 U/L | 98.13 | 96.59 |
| 血清LDH/胸腔 积液ADA | 0.978 | 0.963~0.993 | 8.523 | 98.69 | 95.51 |
| 胸腔积液CEA/ 血清CEA | 0.854 | 0.817~0.891 | 1.096 | 91.24 | 75.03 |
Tab.1 The diagnostic value of different parameters for tuberculous pleural effusion in the study group
| 参数 | AUC | 95%CI | 截断值 | 敏感度/% | 特异度/% |
|---|---|---|---|---|---|
| 胸腔积液ADA | 0.988 | 0.978~0.997 | 29.700 U/L | 98.13 | 96.59 |
| 血清LDH/胸腔 积液ADA | 0.978 | 0.963~0.993 | 8.523 | 98.69 | 95.51 |
| 胸腔积液CEA/ 血清CEA | 0.854 | 0.817~0.891 | 1.096 | 91.24 | 75.03 |
| 组别 | n | 男性 | 年龄/岁 | ||||
|---|---|---|---|---|---|---|---|
| 结核组 | 160 | 118(73.8) | 55.38(37.00,73.00) | ||||
| 恶性组 | 267 | 145(54.3) | 71.66(65.00,73.00) | ||||
| χ2或Z | 15.988** | 7.676** | |||||
| 组别 | 胸腔积液 | ||||||
| LDH/(U/L) | ADA/(U/L) | CEA/(μg/L) | |||||
| 结核组 | 445.00(307.00,701.00) | 55.43(46.00,64.10) | 1.58(0.86,1.91) | ||||
| 恶性组 | 325.50(207.75,618.25) | 9.85(6.00,14.43) | 65.25(6.35,676.09) | ||||
| Z | 3.955** | 16.861** | 14.129** | ||||
| 组别 | 血清 | ||||||
| LDH/(U/L) | ADA/(U/L) | CEA/(μg/L) | |||||
| 结核组 | 202.81(171.00,222.00) | 16.85(12.00,20.80) | 2.72(1.21,3.04) | ||||
| 恶性组 | 223.00(185.00,275.00) | 10.05(8.10,13.78) | 8.67(3.12,40.74) | ||||
| Z | 5.555** | 8.672** | 12.059** | ||||
Tab.2 Comparison of general data between the malignant group and the tuberculosis group
| 组别 | n | 男性 | 年龄/岁 | ||||
|---|---|---|---|---|---|---|---|
| 结核组 | 160 | 118(73.8) | 55.38(37.00,73.00) | ||||
| 恶性组 | 267 | 145(54.3) | 71.66(65.00,73.00) | ||||
| χ2或Z | 15.988** | 7.676** | |||||
| 组别 | 胸腔积液 | ||||||
| LDH/(U/L) | ADA/(U/L) | CEA/(μg/L) | |||||
| 结核组 | 445.00(307.00,701.00) | 55.43(46.00,64.10) | 1.58(0.86,1.91) | ||||
| 恶性组 | 325.50(207.75,618.25) | 9.85(6.00,14.43) | 65.25(6.35,676.09) | ||||
| Z | 3.955** | 16.861** | 14.129** | ||||
| 组别 | 血清 | ||||||
| LDH/(U/L) | ADA/(U/L) | CEA/(μg/L) | |||||
| 结核组 | 202.81(171.00,222.00) | 16.85(12.00,20.80) | 2.72(1.21,3.04) | ||||
| 恶性组 | 223.00(185.00,275.00) | 10.05(8.10,13.78) | 8.67(3.12,40.74) | ||||
| Z | 5.555** | 8.672** | 12.059** | ||||
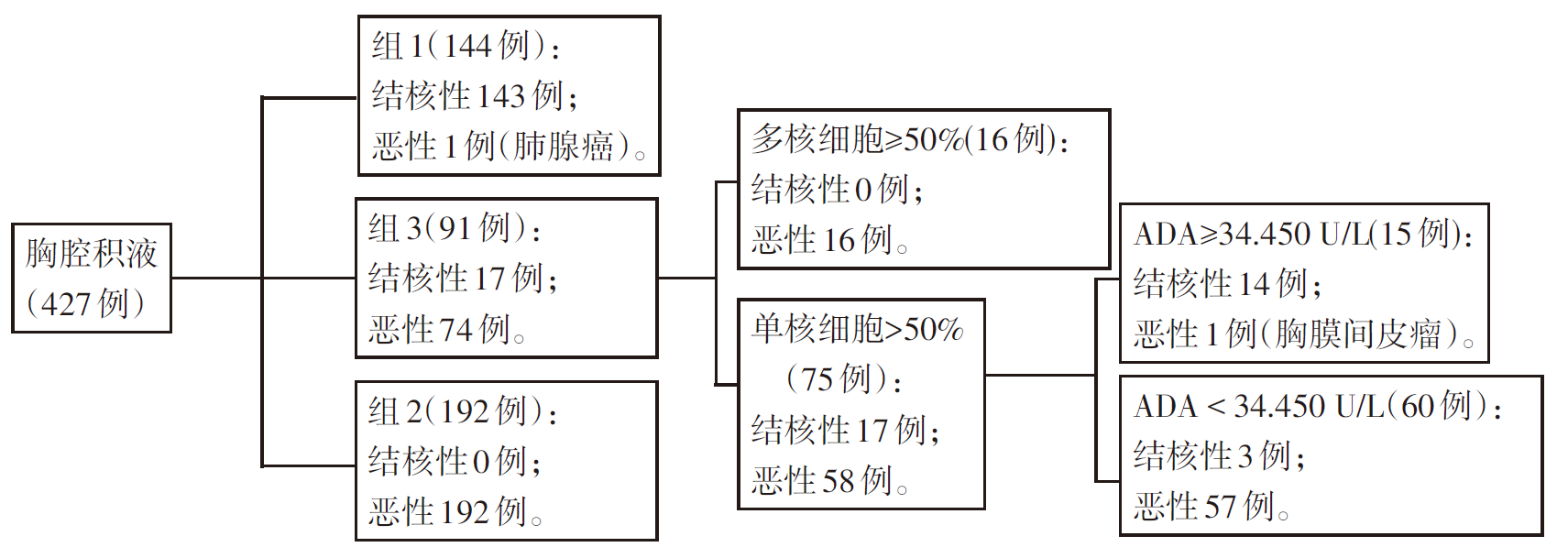
Fig.2 Diagnosis flowchart of the study group
| 诊断标准 | 结核性 | 恶性 | 敏感度/% | 特异度/% | ||||
|---|---|---|---|---|---|---|---|---|
| 真阳性 | 假阳性 | 合计 | 真阳性 | 假阳性 | 合计 | |||
| 1.5诊断流程 | 157 | 3 | 160 | 265 | 2 | 267 | 98.13 | 99.25 |
| ADA≥29.700 U/L | 156 | 9 | 165 | 259 | 3 | 262 | 94.55 | 98.86 |
Tab.3 1.5 Comparison of the diagnostic process, sensitivity and specificity of ADA≥29.700 U/L in the diagnosis of tuberculous pleural effusion
| 诊断标准 | 结核性 | 恶性 | 敏感度/% | 特异度/% | ||||
|---|---|---|---|---|---|---|---|---|
| 真阳性 | 假阳性 | 合计 | 真阳性 | 假阳性 | 合计 | |||
| 1.5诊断流程 | 157 | 3 | 160 | 265 | 2 | 267 | 98.13 | 99.25 |
| ADA≥29.700 U/L | 156 | 9 | 165 | 259 | 3 | 262 | 94.55 | 98.86 |
| 组别 | n | 原发性肺癌 | 转移癌 | 其他 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 腺癌 | 鳞癌 | 小细胞癌 | 肺泡癌 | 总计 | 乳腺 | 消化系统 | 泌尿系统 | 妇科 | 皮肤 | 骨 | 总计 | 胸膜间 皮瘤 | 淋巴瘤 | 白血病 | 总计 | |||
| 研究组 | ||||||||||||||||||
| 组1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | |
| 组2 | 192 | 141 | 19 | 17 | 1 | 178 | 6 | 4 | 1 | 0 | 0 | 1 | 12 | 2 | 0 | 0 | 2 | |
| 组3 | 74 | 28 | 4 | 6 | 1 | 39 | 8 | 8 | 4 | 4 | 2 | 0 | 26 | 6 | 3 | 0 | 9 | |
| 总计 | 267 | 169 | 23 | 23 | 2 | 217 | 14 | 12 | 5 | 4 | 2 | 1 | 38 | 9 | 3 | 0 | 12 | |
| 验证组 | ||||||||||||||||||
| 组1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | |
| 组2 | 58 | 32 | 8 | 2 | 0 | 42 | 3 | 2 | 1 | 8 | 0 | 0 | 14 | 1 | 0 | 1 | 2 | |
| 组3 | 23 | 8 | 0 | 0 | 0 | 8 | 1 | 4 | 2 | 2 | 0 | 0 | 9 | 4 | 2 | 0 | 6 | |
| 总计 | 82 | 40 | 8 | 2 | 0 | 50 | 4 | 6 | 3 | 10 | 0 | 0 | 23 | 5 | 2 | 2 | 9 | |
Tab.4 Malignant pleural effusion disease composition in the study group and the verification group
| 组别 | n | 原发性肺癌 | 转移癌 | 其他 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 腺癌 | 鳞癌 | 小细胞癌 | 肺泡癌 | 总计 | 乳腺 | 消化系统 | 泌尿系统 | 妇科 | 皮肤 | 骨 | 总计 | 胸膜间 皮瘤 | 淋巴瘤 | 白血病 | 总计 | |||
| 研究组 | ||||||||||||||||||
| 组1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | |
| 组2 | 192 | 141 | 19 | 17 | 1 | 178 | 6 | 4 | 1 | 0 | 0 | 1 | 12 | 2 | 0 | 0 | 2 | |
| 组3 | 74 | 28 | 4 | 6 | 1 | 39 | 8 | 8 | 4 | 4 | 2 | 0 | 26 | 6 | 3 | 0 | 9 | |
| 总计 | 267 | 169 | 23 | 23 | 2 | 217 | 14 | 12 | 5 | 4 | 2 | 1 | 38 | 9 | 3 | 0 | 12 | |
| 验证组 | ||||||||||||||||||
| 组1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | |
| 组2 | 58 | 32 | 8 | 2 | 0 | 42 | 3 | 2 | 1 | 8 | 0 | 0 | 14 | 1 | 0 | 1 | 2 | |
| 组3 | 23 | 8 | 0 | 0 | 0 | 8 | 1 | 4 | 2 | 2 | 0 | 0 | 9 | 4 | 2 | 0 | 6 | |
| 总计 | 82 | 40 | 8 | 2 | 0 | 50 | 4 | 6 | 3 | 10 | 0 | 0 | 23 | 5 | 2 | 2 | 9 | |
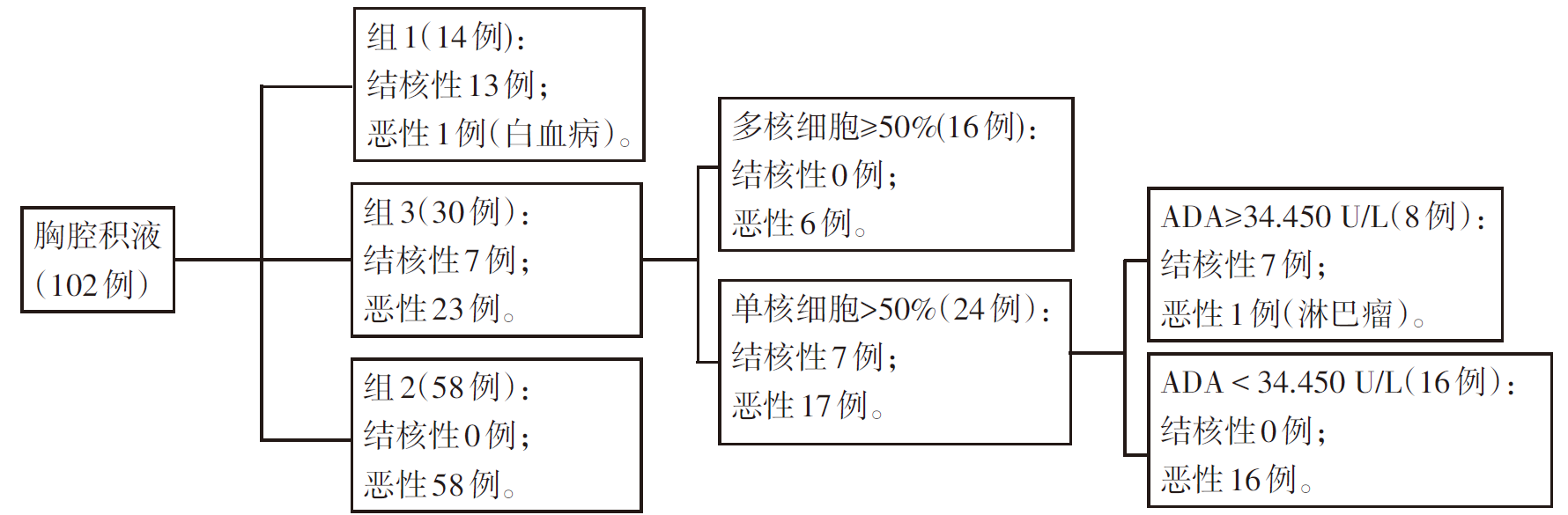
Fig.3 Diagnostic flowchart of the verification group
| [1] | KIM H W, KIM K H, SHIN A Y, et al. Investigating the appropriate adenosine deaminase cutoff value for the diagnosis of tuberculous pleural effusion in a country with decreasing TB burden[J]. Sci Rep, 2022, 12(1):7586. doi:10.1038/s41598-022-11460-w. |
| [2] | VORSTER M J, ALLWOOD B W, DIACON A H, et al. Tuberculous pleural effusions:Advances and controversies[J]. J Thorac Dis, 2015, 7(6):981-991. doi:10.3978/j.issn.2072-1439.2015.02.18. |
| [3] | KOO H K, MIN J, KIM H W, et al. Cluster analysis categorizes five phenotypes of pulmonary tuberculosis[J]. Sci Rep, 2022, 12(1):10084. doi:10.1038/s41598-022-13526-1. |
| [4] | GAO L, WANG W, ZHANG Y, et al. Adenosine deaminase-based measurement in the differential diagnosis of pleural effusion:A multicenter retrospective study[J]. Ther Adv Respir Dis, 2023,17:17534666231155747. doi:10.1177/17534666231155747. |
| [5] | KRISHNAN V G, KUNOOR A, KEECHILATH P, et al. Diagnostic utility of pleural fluid carcinoembryonic antigen in patients with exudative pleural effusion[J]. Lung India, 2021, 38(2):139-143. doi:10.4103/lungindia.lungindia_196_20. |
| [6] | REN Z, XU L. Role of cancer ratio and other new parameters in the differential diagnosis of malignant pleural effusion[J]. Clinics(Sao Paulo), 2021,76:e2515. doi:10.6061/clinics/2021/e2515. |
| [7] | 尉艳霞, 童朝晖, 龚娟妮, 等. 腺苷脱氨酶诊断结核性胸腔积液价值的再评价[J]. 中华结核和呼吸杂志, 2010, 33(4):273-275. |
| YU Y X, TONG Z H, GONG J N, et al. Evaluation of the diagnostic value of adenosine deaminase activity in tuberculous pleuritis[J]. Chinese Journal of Tuberculosis and Respiratory Diseases, 2010, 33(4):273-275. doi:10.3760/cma.j.issn.1001-0939.2010.04.012. | |
| [8] | LI Y, CHEN Z, YANG P, et al. Differentiating between tuberculous and non-tuberculous pleural effusions using the pleural fluid ratio of 10× adenosine deaminase/lactate dehydrogenase[J]. J Thorac Dis, 2023, 15(5):2627-2635. doi:10.21037/jtd-23-383. |
| [9] | ABRAO F C, DE ABREU I R, MIYAKE D H, et al. Role of adenosine deaminase and the influence of age on the diagnosis of pleural tuberculosis[J]. Int J Tuberc Lung Dis, 2014, 18(11):1363-1369. doi:10.5588/ijtld.14.0257. |
| [10] | ZANINI D, MANFREDI L H, PELINSON L P, et al. ADA activity is decreased in lymphocytes from patients with advanced stage of lung cancer[J]. Med Oncol, 2019, 36(9):78. doi:10.1007/s12032-019-1301-1. |
| [11] | IBRAHIM I E, GEHAN A A, ALSHIMAA M A, et al. Role of cancer ratio and carcinogenic embryonic antigen ratio in diagnosis of pleural effusion[J]. Egyptian Journal of Chest Diseases and Tuberculosis, 2017, 66(4):671-674. doi:10.1016/j.ejcdt.2017.07.001. |
| [12] | VERMA A, ABISHEGANADEN J, LIGHT R W. Identifying malignant pleural effusion by a cancer ratio(serum LDH:pleural fluid ADA ratio)[J]. Lung, 2016, 194(1):147-153. doi:10.1007/s00408-015-9831-6. |
| [13] | HACKNER K, ERRHALT P, HANDZHIEV S. Ratio of carcinoembryonic antigen in pleural fluid and serum for the diagnosis of malignant pleural effusion[J]. Ther Adv Med Oncol, 2019,11:1758835919850341. doi:10.1177/1758835919850341. |
| [14] | WANG J, LIU J, XIE X, et al. The pleural fluid lactate dehydrogenase/adenosine deaminase ratio differentiates between tuberculous and parapneumonic pleural effusions[J]. BMC Pulm Med, 2017, 17(1):168. doi:10.1186/s12890-017-0526-z. |
| [15] | LEE J, PARK J E, CHOI S H, et al. Laboratory and radiological discrimination between tuberculous and malignant pleural effusions with high adenosine deaminase levels[J]. Korean J Intern Med, 2022, 37(1):137-145. doi:10.3904/kjim.2020.246. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||