Tianjin Medical Journal ›› 2023, Vol. 51 ›› Issue (2): 207-212.doi: 10.11958/20221393
• Clinical Research • Previous Articles Next Articles
XU Jinhui1( ), XU Guangjuan1, DUAN Lufen1, LIU Kaili2, ZHOU Qin1, SUN Jiantong1, DING Xinyuan1,△()
), XU Guangjuan1, DUAN Lufen1, LIU Kaili2, ZHOU Qin1, SUN Jiantong1, DING Xinyuan1,△()
Received:2022-08-31
Revised:2022-10-22
Published:2023-02-15
Online:2023-02-24
Contact:
△E-mail:XU Jinhui, XU Guangjuan, DUAN Lufen, LIU Kaili, ZHOU Qin, SUN Jiantong, DING Xinyuan. The risk factor analysis for immune-related adverse events in non-small cell lung cancer patients treated with immune checkpoint inhibitors and their relationship to effectiveness[J]. Tianjin Medical Journal, 2023, 51(2): 207-212.
CLC Number:
| 组别 | n | 肿瘤类型 | 治疗方案 | 免疫检查点抑制剂 | |||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非鳞癌 | 鳞癌 | 单药 | 联合化疗 | 帕博利珠 单抗 | 纳武利尤 单抗 | 信迪利 单抗 | 替雷利珠 单抗 | 卡瑞利珠 单抗 | 特瑞普利 单抗 | 度伐利尤 单抗 | |||||||||||||||||||||||||||||||||||
| 无irAEs组 | 79 | 41(51.9) | 38(48.1) | 23(29.1) | 56(70.9) | 15(19.0) | 6 (7.6) | 27(34.2) | 15(19.0) | 11(13.9) | 2(2.5) | 3(3.8) | |||||||||||||||||||||||||||||||||
| 有irAEs组 | 83 | 51(61.4) | 32(38.6) | 22(26.5) | 61(73.5) | 22(26.5) | 3 (3.6) | 23(27.7) | 16(19.3) | 13(15.7) | 4(4.8) | 2(2.4) | |||||||||||||||||||||||||||||||||
| χ2、t或Z | 1.503 | 0.137 | 3.655 | ||||||||||||||||||||||||||||||||||||||||||
| 组别 | 治疗线数 | PD-L1表达 | 既往基因突变 | 年龄(岁) | 性别 | ||||||||||||||||||||||||||||||||||||||||
| 一线 | 非一线 | 未检测 | <1% | 1%~49% | ≥50% | 有突变 | 无突变 | <65 | ≥65 | 男 | 女 | ||||||||||||||||||||||||||||||||||
| 无irAEs组 | 39(49.4) | 40(50.6) | 40(50.6) | 17(21.5) | 15(19.0) | 7(8.9) | 12(15.2) | 67(84.8) | 28(35.4) | 51(64.6) | 61(77.2) | 18(22.8) | |||||||||||||||||||||||||||||||||
| 有irAEs组 | 42(50.6) | 41(49.4) | 44(53.0) | 16(19.3) | 13(15.7) | 10(12.0) | 11(13.3) | 72(86.7) | 33(39.8) | 50(60.2) | 71(85.5) | 12(14.5) | |||||||||||||||||||||||||||||||||
| χ2、t或Z | 0.025 | 0.795 | 0.125 | 0.321 | 1.860 | ||||||||||||||||||||||||||||||||||||||||
| 组别 | 身高(m) | 体质量(kg) | PS评分(分) | 病理分期 | 转移部位 | 吸烟史 | ANC (×109/L) | ||||||||||||||||||||||||||||||||||||||
| 0~1 | ≥2 | Ⅲ期 | Ⅳ期 | <3 | ≥3 | 无 | 有 | ||||||||||||||||||||||||||||||||||||||
| 无irAEs组 | 1.65±0.07 | 62.5(51.5,70.0) | 73(92.4) | 6(7.6) | 18(22.8) | 61(77.2) | 70(88.6) | 9(11.4) | 36(45.6) | 43(54.4) | 4.1(3.2,5.1) | ||||||||||||||||||||||||||||||||||
| 有irAEs组 | 1.67±0.08 | 63.0(56.7,70.0) | 79(95.2) | 4(4.8) | 19(22.9) | 64(77.1) | 75(90.4) | 8(9.6) | 33(39.8) | 50(60.2) | 4.3 (3.1,5.7) | ||||||||||||||||||||||||||||||||||
| χ2、t或Z | 1.278 | 1.511 | 0.166 | 0.000 | 0.133 | 0.559 | 0.099 | ||||||||||||||||||||||||||||||||||||||
| 组别 | ALC(×109/L) | AEC(×109/L) | PLT(×109/L) | ALB(g/L) | NLR | PLR | PNI | ||||||||||||||||||||||||||||||||||||||
| <3 | ≥3 | <180 | ≥180 | <45 | ≥45 | ||||||||||||||||||||||||||||||||||||||||
| 无irAEs组 | 1.2(0.8,1.4) | 0.11(0.05,0.15) | 236(180,272) | 41.4(37.2,44.7) | 30(38.0) | 49(62.0) | 31(39.2) | 48(60.8) | 61(77.2) | 18(22.8) | |||||||||||||||||||||||||||||||||||
| 有irAEs组 | 1.5(1.2,1.8) | 0.13(0.07,0.21) | 221(179,304) | 40.8(37.5,43.6) | 49(59.0) | 34(41.0) | 55(66.3) | 28(33.7) | 70(84.3) | 13(15.7) | |||||||||||||||||||||||||||||||||||
| χ2、t或Z | 4.679** | 1.616 | 0.183 | 0.407 | 7.186** | 11.869** | 1.327 | ||||||||||||||||||||||||||||||||||||||
Tab.1 不同组间患者指标的比较
| 组别 | n | 肿瘤类型 | 治疗方案 | 免疫检查点抑制剂 | |||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非鳞癌 | 鳞癌 | 单药 | 联合化疗 | 帕博利珠 单抗 | 纳武利尤 单抗 | 信迪利 单抗 | 替雷利珠 单抗 | 卡瑞利珠 单抗 | 特瑞普利 单抗 | 度伐利尤 单抗 | |||||||||||||||||||||||||||||||||||
| 无irAEs组 | 79 | 41(51.9) | 38(48.1) | 23(29.1) | 56(70.9) | 15(19.0) | 6 (7.6) | 27(34.2) | 15(19.0) | 11(13.9) | 2(2.5) | 3(3.8) | |||||||||||||||||||||||||||||||||
| 有irAEs组 | 83 | 51(61.4) | 32(38.6) | 22(26.5) | 61(73.5) | 22(26.5) | 3 (3.6) | 23(27.7) | 16(19.3) | 13(15.7) | 4(4.8) | 2(2.4) | |||||||||||||||||||||||||||||||||
| χ2、t或Z | 1.503 | 0.137 | 3.655 | ||||||||||||||||||||||||||||||||||||||||||
| 组别 | 治疗线数 | PD-L1表达 | 既往基因突变 | 年龄(岁) | 性别 | ||||||||||||||||||||||||||||||||||||||||
| 一线 | 非一线 | 未检测 | <1% | 1%~49% | ≥50% | 有突变 | 无突变 | <65 | ≥65 | 男 | 女 | ||||||||||||||||||||||||||||||||||
| 无irAEs组 | 39(49.4) | 40(50.6) | 40(50.6) | 17(21.5) | 15(19.0) | 7(8.9) | 12(15.2) | 67(84.8) | 28(35.4) | 51(64.6) | 61(77.2) | 18(22.8) | |||||||||||||||||||||||||||||||||
| 有irAEs组 | 42(50.6) | 41(49.4) | 44(53.0) | 16(19.3) | 13(15.7) | 10(12.0) | 11(13.3) | 72(86.7) | 33(39.8) | 50(60.2) | 71(85.5) | 12(14.5) | |||||||||||||||||||||||||||||||||
| χ2、t或Z | 0.025 | 0.795 | 0.125 | 0.321 | 1.860 | ||||||||||||||||||||||||||||||||||||||||
| 组别 | 身高(m) | 体质量(kg) | PS评分(分) | 病理分期 | 转移部位 | 吸烟史 | ANC (×109/L) | ||||||||||||||||||||||||||||||||||||||
| 0~1 | ≥2 | Ⅲ期 | Ⅳ期 | <3 | ≥3 | 无 | 有 | ||||||||||||||||||||||||||||||||||||||
| 无irAEs组 | 1.65±0.07 | 62.5(51.5,70.0) | 73(92.4) | 6(7.6) | 18(22.8) | 61(77.2) | 70(88.6) | 9(11.4) | 36(45.6) | 43(54.4) | 4.1(3.2,5.1) | ||||||||||||||||||||||||||||||||||
| 有irAEs组 | 1.67±0.08 | 63.0(56.7,70.0) | 79(95.2) | 4(4.8) | 19(22.9) | 64(77.1) | 75(90.4) | 8(9.6) | 33(39.8) | 50(60.2) | 4.3 (3.1,5.7) | ||||||||||||||||||||||||||||||||||
| χ2、t或Z | 1.278 | 1.511 | 0.166 | 0.000 | 0.133 | 0.559 | 0.099 | ||||||||||||||||||||||||||||||||||||||
| 组别 | ALC(×109/L) | AEC(×109/L) | PLT(×109/L) | ALB(g/L) | NLR | PLR | PNI | ||||||||||||||||||||||||||||||||||||||
| <3 | ≥3 | <180 | ≥180 | <45 | ≥45 | ||||||||||||||||||||||||||||||||||||||||
| 无irAEs组 | 1.2(0.8,1.4) | 0.11(0.05,0.15) | 236(180,272) | 41.4(37.2,44.7) | 30(38.0) | 49(62.0) | 31(39.2) | 48(60.8) | 61(77.2) | 18(22.8) | |||||||||||||||||||||||||||||||||||
| 有irAEs组 | 1.5(1.2,1.8) | 0.13(0.07,0.21) | 221(179,304) | 40.8(37.5,43.6) | 49(59.0) | 34(41.0) | 55(66.3) | 28(33.7) | 70(84.3) | 13(15.7) | |||||||||||||||||||||||||||||||||||
| χ2、t或Z | 4.679** | 1.616 | 0.183 | 0.407 | 7.186** | 11.869** | 1.327 | ||||||||||||||||||||||||||||||||||||||
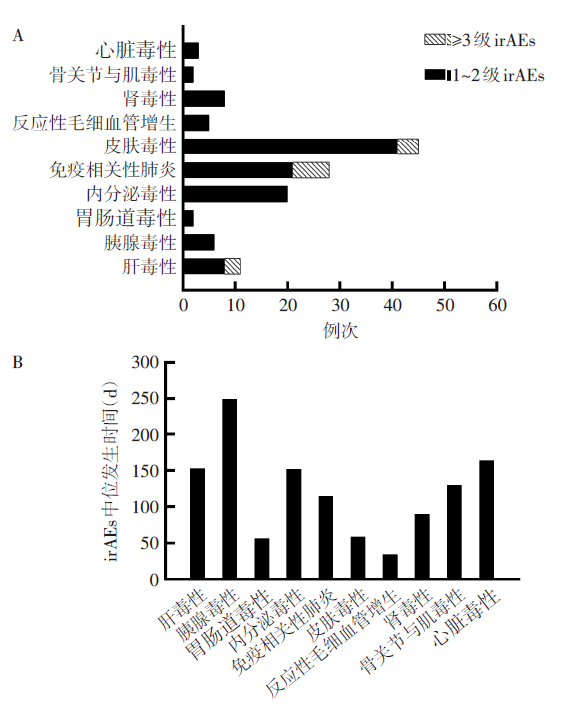
Fig.1 IrAEs spectrum (A) in patients treated with ICIs and time to onset of irAEs (B)
| 变量 | 单因素 | 多因素 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | Wald χ2 | P | OR | OR 95%CI | β | SE | Wald χ2 | P | OR | OR 95%CI | |
| 体质量 | 0.029 | 0.015 | 3.745 | 0.053 | 1.029 | 1.000~1.059 | 0.024 | 0.016 | 2.225 | 0.136 | 1.024 | 0.993~1.056 |
| ALC | 1.537 | 0.375 | 16.772 | <0.001 | 4.652 | 2.229~9.710 | 1.162 | 0.443 | 6.879 | 0.009 | 3.195 | 1.341~7.610 |
| AEC | 2.526 | 1.410 | 3.210 | 0.073 | 12.508 | 0.789~198.312 | 1.354 | 1.407 | 0.926 | 0.336 | 3.873 | 0.246~61.077 |
| NLR | -0.856 | 0.322 | 7.077 | 0.008 | 0.425 | 0.226~0.798 | -0.064 | 0.405 | 0.025 | 0.874 | 0.938 | 0.424~2.073 |
| PLR | -1.112 | 0.327 | 11.565 | 0.001 | 0.329 | 0.173~0.624 | -0.472 | 0.401 | 1.382 | 0.240 | 0.624 | 0.284~1.370 |
| 常数项 | -2.944 | 1.272 | 5.357 | 0.021 | 0.053 | |||||||
Tab.2 患者发生irAEs的单因素和多因素Logistic回归分析
| 变量 | 单因素 | 多因素 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | Wald χ2 | P | OR | OR 95%CI | β | SE | Wald χ2 | P | OR | OR 95%CI | |
| 体质量 | 0.029 | 0.015 | 3.745 | 0.053 | 1.029 | 1.000~1.059 | 0.024 | 0.016 | 2.225 | 0.136 | 1.024 | 0.993~1.056 |
| ALC | 1.537 | 0.375 | 16.772 | <0.001 | 4.652 | 2.229~9.710 | 1.162 | 0.443 | 6.879 | 0.009 | 3.195 | 1.341~7.610 |
| AEC | 2.526 | 1.410 | 3.210 | 0.073 | 12.508 | 0.789~198.312 | 1.354 | 1.407 | 0.926 | 0.336 | 3.873 | 0.246~61.077 |
| NLR | -0.856 | 0.322 | 7.077 | 0.008 | 0.425 | 0.226~0.798 | -0.064 | 0.405 | 0.025 | 0.874 | 0.938 | 0.424~2.073 |
| PLR | -1.112 | 0.327 | 11.565 | 0.001 | 0.329 | 0.173~0.624 | -0.472 | 0.401 | 1.382 | 0.240 | 0.624 | 0.284~1.370 |
| 常数项 | -2.944 | 1.272 | 5.357 | 0.021 | 0.053 | |||||||
| 变量 | 单因素 | 多因素 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | Wald χ2 | P | OR | OR 95%CI | β | SE | Wald χ2 | P | OR | OR 95%CI | |
| ALC | 1.943 | 0.762 | 6.499 | 0.011 | 6.979 | 1.567~31.086 | 1.725 | 0.827 | 4.348 | 0.037 | 5.613 | 1.109~28.411 |
| PLR | -1.188 | 0.623 | 3.638 | 0.056 | 0.305 | 0.090~1.033 | -0.460 | 0.718 | 0.411 | 0.522 | 0.631 | 0.155~2.578 |
| 常数项 | -2.069 | 1.302 | 2.526 | 0.112 | 0.126 | |||||||
Tab.3 接受ICIs单药治疗患者发生irAEs的单因素和多因素Logistic回归分析
| 变量 | 单因素 | 多因素 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | Wald χ2 | P | OR | OR 95%CI | β | SE | Wald χ2 | P | OR | OR 95%CI | |
| ALC | 1.943 | 0.762 | 6.499 | 0.011 | 6.979 | 1.567~31.086 | 1.725 | 0.827 | 4.348 | 0.037 | 5.613 | 1.109~28.411 |
| PLR | -1.188 | 0.623 | 3.638 | 0.056 | 0.305 | 0.090~1.033 | -0.460 | 0.718 | 0.411 | 0.522 | 0.631 | 0.155~2.578 |
| 常数项 | -2.069 | 1.302 | 2.526 | 0.112 | 0.126 | |||||||
| 变量 | 单因素 | 多因素 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | Wald χ2 | P | OR | OR 95%CI | β | SE | Wald χ2 | P | OR | OR 95%CI | |
| ALC | 1.386 | 0.432 | 10.272 | 0.001 | 3.999 | 1.713~9.334 | 1.065 | 0.494 | 4.655 | 0.031 | 2.901 | 1.102~7.633 |
| NLR | -0.808 | 0.378 | 4.559 | 0.033 | 0.446 | 0.212~0.936 | -0.135 | 0.450 | 0.090 | 0.764 | 0.874 | 0.362~2.110 |
| PLR | -1.079 | 0.385 | 7.855 | 0.005 | 0.340 | 0.160~0.723 | -0.517 | 0.462 | 1.253 | 0.263 | 0.596 | 0.241~1.474 |
| 常数项 | -1.070 | 0.856 | 1.561 | 0.212 | 0.343 | |||||||
Tab.4 接受ICIs联合化疗患者发生irAEs的单因素和多因素Logistic回归分析
| 变量 | 单因素 | 多因素 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | Wald χ2 | P | OR | OR 95%CI | β | SE | Wald χ2 | P | OR | OR 95%CI | |
| ALC | 1.386 | 0.432 | 10.272 | 0.001 | 3.999 | 1.713~9.334 | 1.065 | 0.494 | 4.655 | 0.031 | 2.901 | 1.102~7.633 |
| NLR | -0.808 | 0.378 | 4.559 | 0.033 | 0.446 | 0.212~0.936 | -0.135 | 0.450 | 0.090 | 0.764 | 0.874 | 0.362~2.110 |
| PLR | -1.079 | 0.385 | 7.855 | 0.005 | 0.340 | 0.160~0.723 | -0.517 | 0.462 | 1.253 | 0.263 | 0.596 | 0.241~1.474 |
| 常数项 | -1.070 | 0.856 | 1.561 | 0.212 | 0.343 | |||||||
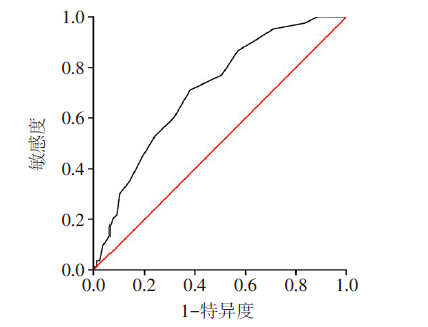
Fig.2 ROC curve of irAEs predicted by ALC level
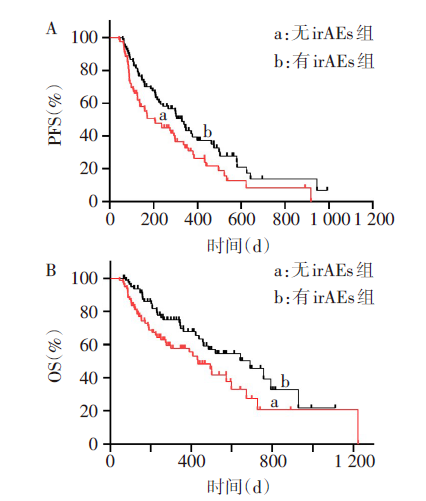
Fig.3 Impact of immune-related adverse events (irAEs) on PFS (A) and OS (B) of all NSCLC patients treated with ICIs
| [1] | SUNG H, FERLAY J, SIEGEL R L, et al. Global Cancer Statistics 2020:GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries[J]. CA Cancer J Clin, 2021, 71(3):209-249. doi:10.3322/caac.21660. |
| [2] | CHEN W, ZHENG R, BAADE P D, et al. Cancer statistics in China,2015[J]. CA Cancer J Clin, 2016, 66(2):115-132. doi:10.3322/caac.21338. |
| [3] | GADGEEL S, RODRÍGUEZ-ABREU D, SPERANZA G, et al. Updated analysis from KEYNOTE-189:Pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metastatic nonsquamous non-small-cell lung cancer[J]. J Clin Oncol, 2020, 38(14):1505-1517. doi:10.1200/JCO.19.03136. |
| [4] | CHAMPIAT S, LAMBOTTE O, BARREAU E, et al. Management of immune checkpoint blockade dysimmune toxicities:A collaborative position paper[J]. Ann Oncol, 2016, 27(4):559-574. doi:10.1093/annonc/mdv623. |
| [5] | DIEHL A, YARCHOAN M, HOPKINS A, et al. Relationships between lymphocyte counts and treatment-related toxicities and clinical responses in patients with solid tumors treated with PD-1 checkpoint inhibitors[J]. Oncotarget, 2017, 8(69):114268-114280. doi:10.18632/oncotarget.23217. |
| [6] | PAVAN A, CALVETTI L, DAL MASO A, et al. Peripheral blood markers identify risk of immune-related toxicity in advanced non-small cell lung cancer treated with immune-checkpoint inhibitors[J]. Oncologist, 2019, 24(8):1128-1136. doi:10.1634/theoncologist.2018-0563. |
| [7] | WATANABE I, KANAUCHI N, WATANABE H. Preoperative prognostic nutritional index as a predictor of outcomes in elderly patients after surgery for lung cancer[J]. Jpn J Clin Oncol, 2018, 48(4):382-387. doi:10.1093/jjco/hyy014. |
| [8] | 中国临床肿瘤学会指南工作委员会. 中国临床肿瘤学会(CSCO)免疫检查点抑制剂相关的毒性管理指南[M]. 北京: 人民卫生出版社, 2019:27-118. |
| Chinese Society of Clinical Oncology Guidelines Working Committee. Management of immunotherapy-related toxicities:CSCO Clinical Practice Guidelines[M]. Beijing: People's Health Publishing House, 2019:27-118. | |
| [9] | EISENHAUER E A, THERASSE P, BOGAERTS J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1)[J]. Eur J Cancer, 2009, 45(2):228-247. doi:10.1016/j.ejca.2008.10.026. |
| [10] | SHI Y, FANG J, ZHOU C, et al. Immune checkpoint inhibitor-related adverse events in lung cancer:Real-world incidence and management practices of 1905 patients in China[J]. Thorac Cancer, 2022, 13(3):412-422. doi:10.1111/1759-7714.14274. |
| [11] | EIGENTLER T K, HASSEL J C, BERKING C, et al. Diagnosis,monitoring and management of immune-related adverse drug reactions of anti-PD-1 antibody therapy[J]. Cancer Treat Rev, 2016, 45:7-18. doi:10.1016/j.ctrv.2016.02.003. |
| [12] | HARATANI K, HAYASHI H, CHIBA Y, et al. Association of immune-related adverse events with nivolumab efficacy in non-small-cell lung cancer[J]. JAMA Oncol, 2018, 4(3):374-378. doi:10.1001/jamaoncol.2017.2925. |
| [13] | 中国临床肿瘤学会指南工作委员会. 中国临床肿瘤学会(CSCO)免疫检查点抑制剂临床应用指南2022[M]. 北京: 人民卫生出版社, 2022:106-122. |
| Guidelines Working Committee of Chinese Society of Clinical Oncology. Chinese Society of Clinical Oncology (CSCO) Guidelines for Clinical Application of Immune Checkpoint Inhibitors 2022[M]. Beijing: People's Health Publishing House, 2022:106-122. | |
| [14] | LIU C, ZHENG S, JIN R, et al. The superior efficacy of anti-PD-1/PD-L1 immunotherapy in KRAS-mutant non-small cell lung cancer that correlates with an inflammatory phenotype and increased immunogenicity[J]. Cancer Lett, 2020, 470:95-105. doi:10.1016/j.canlet.2019.10.027. |
| [15] | CHEN X, NIE J, DAI L, et al. Immune-related adverse events and their association with the effectiveness of PD-1/PD-L1 inhibitors in non-small cell lung cancer:A real-world study from China[J]. Front Oncol, 2021, 11:607531. doi:10.3389/fonc.2021.607531. |
| [16] | KHOJA L, DAY D, WEI-WU CHEN T, et al. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors:A systematic review[J]. Ann Oncol, 2017, 28(10):2377-2385. doi:10.1093/annonc/mdx286. |
| [17] | SURESH K, VOONG K R, SHANKAR B, et al. Pneumonitis in non-small cell lung cancer patients receiving immune checkpoint immunotherapy:Incidence and risk factors[J]. J Thorac Oncol, 2018, 13(12):1930-1939. doi:10.1016/j.jtho.2018.08.2035. |
| [18] | EGAMI S, KAWAZOE H, HASHIMOTO H, et al. Peripheral blood biomarkers predict immune-related adverse events in non-small cell lung cancer patients treated with pembrolizumab:A multicenter retrospective study[J]. J Cancer, 2021, 12(7):2105-2112. doi:10.7150/jca.53242. |
| [19] | SCHIETINGER A, GREENBERG P D. Tolerance and exhaustion:Defining mechanisms of T cell dysfunction[J]. Trends Immunol, 2014, 35(2):51-60. doi:10.1016/j.it.2013.10.001. |
| [20] | GARBO R, LORENZUT S, DEL NEGRO I, et al. Lower lymphocyte counts and older age are associated with reduced multiple sclerosis disease activity during dimethyl fumarate treatment[J]. Mult Scler Relat Disord, 2021, 49:102781. doi:10.1016/j.msard.2021.102781. |
| [21] | BALDINI E, LUNGHI A, CORTESI E, et al. Immune-related adverse events correlate with clinical outcomes in NSCLC patients treated with nivolumab: The Italian NSCLC expanded access program[J]. Lung Cancer, 2020, 140:59-64. doi:10.1016/j.lungcan.2019.12.014. |
| [22] | CORTELLINI A, FRIEDLAENDER A, BANNA G L, et al. Immune-related adverse events of pembrolizumab in a large real-world cohort of patients with NSCLC with a PD-L1 expression ≥ 50% and their relationship with clinical outcomes[J]. Clin Lung Cancer, 2020, 21(6):498-508.e2. doi:10.1016/j.cllc.2020.06.010. |
| [23] | CORTELLINI A, CHIARI R, RICCIUTI B, et al. Correlations between the immune-related adverse events spectrum and efficacy of anti-PD1 immunotherapy in NSCLC patients[J]. Clin Lung Cancer, 2019, 20(4):237-247.e1. doi:10.1016/j.cllc.2019.02.006. |
| [24] | 赵倩, 陈瑞祥, 温瑾, 等. ICIs治疗NSCLC致免疫相关不良反应与疗效相关性的Meta分析[J]. 中国药房, 2022, 33(6):745-752. |
| ZHAO Q, CHEN R X, WEN J, et al. Meta-analysis of the correlation between immune-related adverse events and efficacy of immune checkpoint inhibitors in the treatment of non-small cell lung cancer[J]. China Pharmacy, 2022, 33(6):745-752. doi:10.6039/j.issn.1001-0408.2022.06.17. | |
| [25] | LEE D J, LEE H J J R, FARMER J R, et al. Mechanisms driving immune-related adverse events in cancer patients treated with immune checkpoint inhibitors[J]. Curr Cardiol Rep, 2021, 23(8):98. doi:10.1007/s11886-021-01530-2. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||