Tianjin Medical Journal ›› 2024, Vol. 52 ›› Issue (11): 1177-1182.doi: 10.11958/20240546
• Clinical Research • Previous Articles Next Articles
YU Ping1,2( ), ZHOU Min2, SU Dan1,2,△()
), ZHOU Min2, SU Dan1,2,△()
Received:2024-05-07
Revised:2024-07-26
Published:2024-11-15
Online:2024-11-12
Contact:
△E-mail:303483765@qq.com
YU Ping, ZHOU Min, SU Dan. Construction and validation of chemotherapy resistance prediction model for ovarian cancer[J]. Tianjin Medical Journal, 2024, 52(11): 1177-1182.
CLC Number:
| 组别 | n | 年龄/岁 | BMI/(kg/m2) | 病理类型(A/B/C/D)# | ||
|---|---|---|---|---|---|---|
| 未复发组 | 44 | 57.7±8.1 | 24.4±3.6 | 33/4/3/4 | ||
| 复发组 | 363 | 52.8±9.6 | 23.6±3.3 | 283/21/32/27 | ||
| t或χ2 | 3.262** | 1.482 | 1.065 | |||
| 组别 | 组织学分级(高/中/低分化) | FIGO分期(Ⅰ/Ⅱ/Ⅲ/Ⅳ) | ||||
| 未复发组 | 23/6/15 | 11/14/18/1 | ||||
| 复发组 | 45/89/229 | 72/41/223/27 | ||||
| Z | 2.192* | 2.924** | ||||
Tab.1 Comparison of clinical variables between the recurrence group and the non-recurrence group
| 组别 | n | 年龄/岁 | BMI/(kg/m2) | 病理类型(A/B/C/D)# | ||
|---|---|---|---|---|---|---|
| 未复发组 | 44 | 57.7±8.1 | 24.4±3.6 | 33/4/3/4 | ||
| 复发组 | 363 | 52.8±9.6 | 23.6±3.3 | 283/21/32/27 | ||
| t或χ2 | 3.262** | 1.482 | 1.065 | |||
| 组别 | 组织学分级(高/中/低分化) | FIGO分期(Ⅰ/Ⅱ/Ⅲ/Ⅳ) | ||||
| 未复发组 | 23/6/15 | 11/14/18/1 | ||||
| 复发组 | 45/89/229 | 72/41/223/27 | ||||
| Z | 2.192* | 2.924** | ||||
| 组别 | n | 年龄/岁 | BMI/(kg/m2) | 术前全腹增强CT | 手术相关 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 肿瘤最长径/cm | 腹腔积液 | 淋巴结增大 | 大网膜转移 | 手术时长/min | 术中出血量/mL | ||||||||||||
| 敏感组 | 304 | 52.3±10.1 | 23.6±3.2 | 9.2±5.6 | 181(59.5) | 100(32.9) | 178(58.6) | 270(210,354) | 500(300,800) | ||||||||
| 耐药组 | 59 | 53.1±9.4 | 23.6±3.5 | 7.8±4.4 | 29(49.2) | 31(52.5) | 30(50.8) | 290(205,350) | 580(350,800) | ||||||||
| t、χ2或Z | 0.516 | 0.020 | 1.530 | 2.186 | 8.270** | 1.199 | 0.456 | 0.265 | |||||||||
| 组别 | Hb降低值/(g/L) | 手术前后血肿瘤标志物变化率/% | |||||||||||||||
| AFP | CA125 | CA199 | CEA | HE4 | ROMA(绝经后) | ROMA(绝经前) | |||||||||||
| 敏感组 | 16.0±8.9 | 2.3±1.0 | 73.5±20.6 | 19.2(7.5,26.2) | 32.3±14.9 | 43.5±8.4 | 35.2(20.6,44.8) | 53.8±15.0 | |||||||||
| 耐药组 | 13.6±5.4 | 1.8±0.8 | 50.3±20.1 | 28.1(11.2,37.1) | 37.8±14.4 | 52.7±2.8 | 23.4(11.2,29.5) | 39.5±13.3 | |||||||||
| Z或t | 0.881 | 1.252 | 7.896** | 0.417 | 0.670 | 0.456 | 0.499 | 1.470 | |||||||||
Tab.2 Comparison of clinical and surgical variables between the chemotherapy-resistant group and the chemotherapy-sensitive group
| 组别 | n | 年龄/岁 | BMI/(kg/m2) | 术前全腹增强CT | 手术相关 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 肿瘤最长径/cm | 腹腔积液 | 淋巴结增大 | 大网膜转移 | 手术时长/min | 术中出血量/mL | ||||||||||||
| 敏感组 | 304 | 52.3±10.1 | 23.6±3.2 | 9.2±5.6 | 181(59.5) | 100(32.9) | 178(58.6) | 270(210,354) | 500(300,800) | ||||||||
| 耐药组 | 59 | 53.1±9.4 | 23.6±3.5 | 7.8±4.4 | 29(49.2) | 31(52.5) | 30(50.8) | 290(205,350) | 580(350,800) | ||||||||
| t、χ2或Z | 0.516 | 0.020 | 1.530 | 2.186 | 8.270** | 1.199 | 0.456 | 0.265 | |||||||||
| 组别 | Hb降低值/(g/L) | 手术前后血肿瘤标志物变化率/% | |||||||||||||||
| AFP | CA125 | CA199 | CEA | HE4 | ROMA(绝经后) | ROMA(绝经前) | |||||||||||
| 敏感组 | 16.0±8.9 | 2.3±1.0 | 73.5±20.6 | 19.2(7.5,26.2) | 32.3±14.9 | 43.5±8.4 | 35.2(20.6,44.8) | 53.8±15.0 | |||||||||
| 耐药组 | 13.6±5.4 | 1.8±0.8 | 50.3±20.1 | 28.1(11.2,37.1) | 37.8±14.4 | 52.7±2.8 | 23.4(11.2,29.5) | 39.5±13.3 | |||||||||
| Z或t | 0.881 | 1.252 | 7.896** | 0.417 | 0.670 | 0.456 | 0.499 | 1.470 | |||||||||
| 组别 | n | 病理类型(A/B/C/D) | 组织学分级(高/中/低分化) | FIGO分期(Ⅰ/Ⅱ/Ⅲ/Ⅳ) | 免疫组化阳性CDX2 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 敏感组 | 304 | 253/11/19/21 | 32/83/189 | 67/36/181/20 | 160 | ||||||||||||||
| 耐药组 | 59 | 30/10/13/6 | 13/6/40 | 5/5/42/7 | 35 | ||||||||||||||
| χ2或Z | 36.492** | 0.097 | 2.817** | 0.890 | |||||||||||||||
| 组别 | 免疫组化阳性 | ||||||||||||||||||
| CK | CK7 | CK20 | ER | Ki-67 | P16 | WT-1 | PAX-8 | PR | VEGF | Villin | P53 | ||||||||
| 敏感组 | 171(56.2) | 101(33.2) | 171(56.2) | 84(27.6) | 207(68.1) | 131(43.1) | 179(58.9) | 135(44.4) | 56(18.4) | 181(59.5) | 89(29.3) | 173(56.9) | |||||||
| 耐药组 | 23(39.0) | 16(27.1) | 23(39.0) | 17(28.8) | 50(84.7) | 16(27.1) | 46(78.0) | 22(37.3) | 12(20.3) | 45(76.3) | 22(37.3) | 42(71.2) | |||||||
| χ2 | 0.458 | 0.843 | 0.458 | 0.034 | 6.628* | 5.232* | 7.637** | 1.020 | 0.119 | 5.887* | 1.494 | 4.172* | |||||||
Tab.3 Comparison of pathological characteristics between the chemotherapy-resistant group and the chemotherapy-sensitive group
| 组别 | n | 病理类型(A/B/C/D) | 组织学分级(高/中/低分化) | FIGO分期(Ⅰ/Ⅱ/Ⅲ/Ⅳ) | 免疫组化阳性CDX2 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 敏感组 | 304 | 253/11/19/21 | 32/83/189 | 67/36/181/20 | 160 | ||||||||||||||
| 耐药组 | 59 | 30/10/13/6 | 13/6/40 | 5/5/42/7 | 35 | ||||||||||||||
| χ2或Z | 36.492** | 0.097 | 2.817** | 0.890 | |||||||||||||||
| 组别 | 免疫组化阳性 | ||||||||||||||||||
| CK | CK7 | CK20 | ER | Ki-67 | P16 | WT-1 | PAX-8 | PR | VEGF | Villin | P53 | ||||||||
| 敏感组 | 171(56.2) | 101(33.2) | 171(56.2) | 84(27.6) | 207(68.1) | 131(43.1) | 179(58.9) | 135(44.4) | 56(18.4) | 181(59.5) | 89(29.3) | 173(56.9) | |||||||
| 耐药组 | 23(39.0) | 16(27.1) | 23(39.0) | 17(28.8) | 50(84.7) | 16(27.1) | 46(78.0) | 22(37.3) | 12(20.3) | 45(76.3) | 22(37.3) | 42(71.2) | |||||||
| χ2 | 0.458 | 0.843 | 0.458 | 0.034 | 6.628* | 5.232* | 7.637** | 1.020 | 0.119 | 5.887* | 1.494 | 4.172* | |||||||
| 组别 | n | 化疗前后血清肿瘤标志物变化率/% | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AFP | CA125 | CA199 | CEA | HE4 | ROMA(绝经后) | ROMA(绝经前) | ||||||
| 敏感组 | 304 | 9.6(1.2,26.9) | 49.3±37.7 | 13.5(7.5,19.2) | 40.5±15.6 | 5.5(3.2,7.8) | 60.0±14.7 | 49.1(34.5,76.3) | ||||
| 耐药组 | 59 | 15.2(9.3,18.5) | 49.9±37.8 | 31.8(17.9,49.4) | 48.2±11.6 | 10.4(5.6,18.4) | 57.1±14.8 | 31.3(19.7,50.5) | ||||
| Z或t | 1.125 | 0.059 | 0.046 | 0.406 | 0.194 | 0.261 | 2.256** | |||||
| 组别 | 化疗疗程/个 | 化疗不良反应 | ||||||||||
| 骨髓抑制 | 肝肾功损害 | 胃肠道反应 | ||||||||||
| 敏感组 | 7.3±2.7 | 88(28.9) | 63(20.7) | 94(30.9) | ||||||||
| 耐药组 | 7.0±3.9 | 16(27.1) | 9(15.3) | 17(28.8) | ||||||||
| χ2或t | 0.847 | 0.081 | 0.930 | 0.103 | ||||||||
Tab.4 Comparison of variables of chemotherapy and adverse reactions between the chemotherapy-resistant group and the chemotherapy-sensitive groups
| 组别 | n | 化疗前后血清肿瘤标志物变化率/% | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AFP | CA125 | CA199 | CEA | HE4 | ROMA(绝经后) | ROMA(绝经前) | ||||||
| 敏感组 | 304 | 9.6(1.2,26.9) | 49.3±37.7 | 13.5(7.5,19.2) | 40.5±15.6 | 5.5(3.2,7.8) | 60.0±14.7 | 49.1(34.5,76.3) | ||||
| 耐药组 | 59 | 15.2(9.3,18.5) | 49.9±37.8 | 31.8(17.9,49.4) | 48.2±11.6 | 10.4(5.6,18.4) | 57.1±14.8 | 31.3(19.7,50.5) | ||||
| Z或t | 1.125 | 0.059 | 0.046 | 0.406 | 0.194 | 0.261 | 2.256** | |||||
| 组别 | 化疗疗程/个 | 化疗不良反应 | ||||||||||
| 骨髓抑制 | 肝肾功损害 | 胃肠道反应 | ||||||||||
| 敏感组 | 7.3±2.7 | 88(28.9) | 63(20.7) | 94(30.9) | ||||||||
| 耐药组 | 7.0±3.9 | 16(27.1) | 9(15.3) | 17(28.8) | ||||||||
| χ2或t | 0.847 | 0.081 | 0.930 | 0.103 | ||||||||
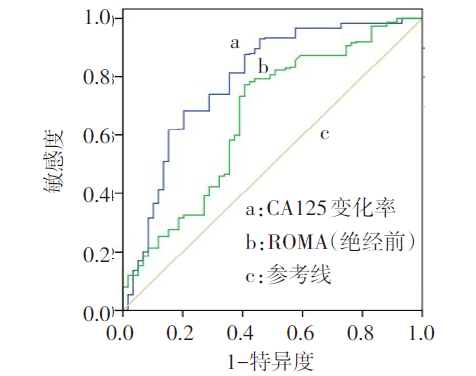
Fig.1 ROC curves of change rates of CA125 before and after surgery and the change rates of ROMA (premenopausal) before and after chemotherapy
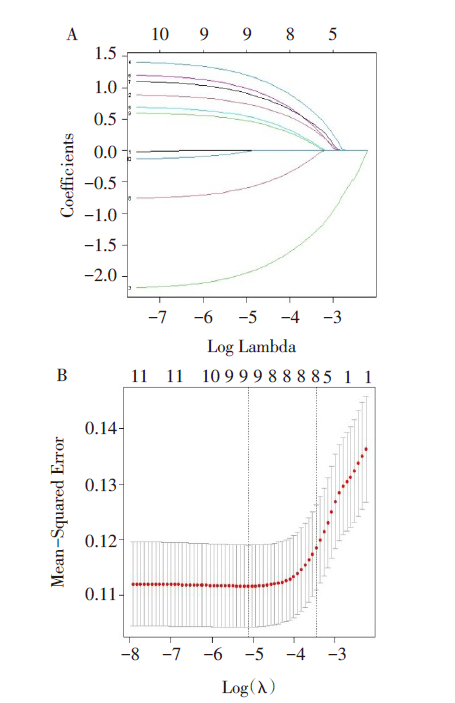
Fig.2 Screening of risk factors for chemo-resistance of ovarian cancer
| 临床特征 | β | SE | Waldχ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| 淋巴结增大 | 0.888 | 0.340 | 6.832 | 0.009 | 2.431 | 1.249~4.734 |
| 病理类型 | -2.207 | 0.386 | 32.769 | 0.001 | 0.110 | 0.052~0.234 |
| FIGO分期 | 1.433 | 0.446 | 10.299 | 0.001 | 4.189 | 1.747~10.049 |
| Ki-67 | 0.723 | 0.479 | 2.277 | 0.131 | 2.060 | 0.806~5.269 |
| WT-1 | 1.209 | 0.385 | 9.872 | 0.002 | 3.352 | 1.576~7.128 |
| VEGF | 1.102 | 0.428 | 6.628 | 0.010 | 3.011 | 1.301~6.970 |
| P16 | -0.778 | 0.367 | 4.499 | 0.034 | 0.460 | 0.224~0.943 |
| P53 | 0.622 | 0.357 | 3.036 | 0.081 | 1.863 | 0.925~3.749 |
| 常数项 | -3.849 | 0.668 | 33.208 | 0.001 | 0.021 | — |
Tab.5 Multifactorial Logistic regression for chemotherapy resistance prediction model in ovarian cancer
| 临床特征 | β | SE | Waldχ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| 淋巴结增大 | 0.888 | 0.340 | 6.832 | 0.009 | 2.431 | 1.249~4.734 |
| 病理类型 | -2.207 | 0.386 | 32.769 | 0.001 | 0.110 | 0.052~0.234 |
| FIGO分期 | 1.433 | 0.446 | 10.299 | 0.001 | 4.189 | 1.747~10.049 |
| Ki-67 | 0.723 | 0.479 | 2.277 | 0.131 | 2.060 | 0.806~5.269 |
| WT-1 | 1.209 | 0.385 | 9.872 | 0.002 | 3.352 | 1.576~7.128 |
| VEGF | 1.102 | 0.428 | 6.628 | 0.010 | 3.011 | 1.301~6.970 |
| P16 | -0.778 | 0.367 | 4.499 | 0.034 | 0.460 | 0.224~0.943 |
| P53 | 0.622 | 0.357 | 3.036 | 0.081 | 1.863 | 0.925~3.749 |
| 常数项 | -3.849 | 0.668 | 33.208 | 0.001 | 0.021 | — |
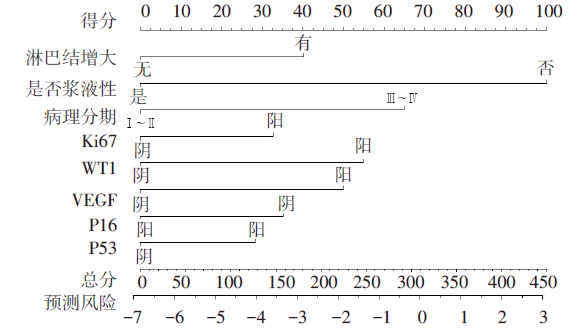
Fig.3 Nomogram of binary Logistic regression analysis for predicting the chemotherapy resistance of ovarian cancer
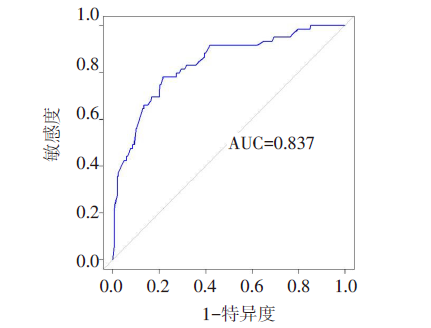
Fig.4 ROC curve analysis of the prediction model for ovarian cancer patients with chemo-resistance
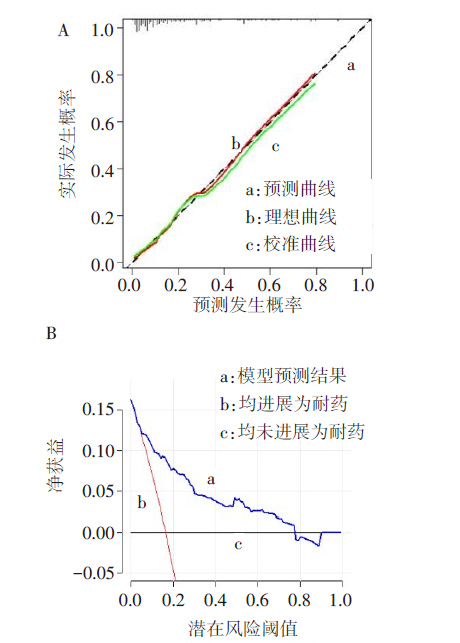
Fig.5 Calibration curve and DCA curve of a nomogram model predicting chemo-resistance of ovarian cancer
| [1] | 李少儒, 李燕, 刘珊, 等. LncRNA SNHG11通过抑制miR-184/CARM1信号轴促进卵巢癌生长[J]. 天津医药, 2023, 51(6):561-567. |
| LI S R, LI Y, LIU S, et al. Influences of lncRNA SNHG11 on proliferation, apoptosis, migration and invasion of ovarian cancer cells by regulating miR-184/CARM1 signaling axis[J]. Tianjin Med J, 2023, 51(6):561-567. doi:10.11958/20221256. | |
| [2] | 钱瑜华, 高燕, 张艳. 卵巢癌化疗耐药机制及治疗药物的研究进展[J]. 医学综述, 2022, 28(5):929-933. |
| QIAN Y H, GAO Y, ZHANG Y. Research progress of drug resistance mechanism and therapeutic drugs in ovarian cancer[J]. Medical Recapitulate, 2022, 28(5):929-933. doi:10.3969/j.issn.1006-2084.2022.05.017. | |
| [3] | 林世鑫, 高军. 黄酮类化合物抗卵巢癌化疗耐药的作用进展[J]. 天津医药, 2020, 48(10):1010-1014. |
| LIN S X, GAO J. Progress in the effect of flavonoids on drug resistance in ovarian cancer[J]. Tianjin Med J, 2020, 48(10):1010-1014. doi:10.11958/20200130. | |
| [4] | 赵玲, 刘历, 王海燕, 等. 基于CT-PCI与临床指标构建预测晚期上皮性卵巢癌减瘤术结局的列线图模型[J]. 中国医学计算机成像杂志, 2023, 29(3):283-289. |
| ZHAO L, LIU L, WANG H Y, et al. Construction of nomogram model to predict the outcome of debulking surgery for advanced epithelial ovarian cancer based on CT peritoneal cancer index and clinical indicators[J]. Chin Comput Med Imag, 2023, 29(3):283-289. doi:10.19627/j.cnki.cn31-1700/th.2023.03.018. | |
| [5] | ARMSTRONG DK, ALVAREZ RD, BACKES FJ, et al. NCCN guidelines(R) insights:ovarian cancer,version 3.2022[J]. J Natl Compr Canc Netw, 2022, 20(9):972-980. doi:10.6004/jnccn.2022.0047. |
| [6] | BASCH E, BECKER C, ROGAK LJ, et al. Composite grading algorithm for the national cancer institute's patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE)[J]. Clin Trials, 2021, 18(1):104-114. doi:10.1177/1740774520975120. |
| [7] | GONZÁLEZ-MARTÍN A, HARTER P, LEARY A, et al. Newly diagnosed and relapsed epithelial ovarian cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up[J]. Ann Oncol, 2023, 34(10):833-848. doi:10.1016/j.annonc.2023.07.011. |
| [8] | BUECHEL M, HERZOG T J, WESTIN S N, et al. Treatment of patients with recurrent epithelial ovarian cancer for whom platinum is still an option[J]. Ann Oncol, 2019, 30(5):721-732. doi:10.1093/annonc/mdz104. |
| [9] | LUVERO D, PLOTTI F, ALOISIA A, et al. Ovarian cancer relapse: From the latest scientific evidence to the best practice[J]. Crit Rev Oncol Hematol, 2019, 140:28-38. doi:10.1016/j.critrevonc.2019.05.014. |
| [10] | MA G, ZENG S, ZHAO Y, et al. Development and validation of a nomogram to predict cancer-specific survival of mucinous epithelial ovarian cancer after cytoreductive surgery[J]. J Ovarian Res, 2023, 16(1):120. doi:10.1186/s13048-023-01213-2. |
| [11] | SAID S A, BRETVELD R W, KOFFIJBERG H, et al. Clinicopathologic predictors of early relapse in advanced epithelial ovarian cancer: development of prediction models using nationwide data[J]. Cancer Epidemiol, 2021,75:102008. doi:10.1016/j.canep.2021.102008. |
| [12] | 朱艳红, 蔡玉洁, 葛银. 上皮性卵巢癌术后复发的相关影响因素分析[J]. 实用癌症杂志, 2022, 37(1):117-119. |
| ZHU Y H, CAI Y J, GE Y. Analysis of related factors of postoperative recurrence of epithelial ovarian cancer[J]. The Practical Journal of Cancer, 2022, 37(1):117-119. doi:10.3969/j.issn.1001-5930.2022.01.034. | |
| [13] | HEITZ F, HARTER P, ATASEVEN B, et al. Stage-and histologic subtype-dependent frequency of lymph node metastases in patients with epithelial ovarian cancer undergoing systematic pelvic and paraaortic lymphadenectomy[J]. Ann Surg Oncol, 2018, 25(7):2053-2059. doi:10.1245/s10434-018-6412-y. |
| [14] | PEREZ-FIDALGO J A, ORTEGA B, SIMON S, et al. NOTCH signalling in ovarian cancer angiogenesis[J]. Ann Transl Med, 2020, 8(24):1705. doi:10.21037/atm-20-4497. |
| [15] | DAVIS A, TINKER A V, FRIEDLANDER M. "Platinum resistant" ovarian cancer: what is it, who to treat and how to measure benefit?[J]. Gynecol Oncol, 2014, 133(3):624-631. doi:10.1016/j.ygyno.2014.02.038. |
| [16] | FU Y, WANG X, PAN Z, et al. Clinical outcomes and prognostic factors of patients with epithelial ovarian cancer subjected to first-line treatment:a retrospective study of 251 cases[J]. Front Med, 2014, 8(1):91-95. doi:10.1007/s11684-014-0305-7. |
| [17] | 蒋琴, 徐杰, 严科. 卵巢癌铂耐药复发相关临床因素研究[J]. 中国临床医生杂志, 2021, 49(11):1287-1290. |
| JIANG Q, XU J, YAN K. Study on the clinical factors of recurrence of platinum resistance in ovarian cancer[J]. China Clinical Journal, 2021, 49(11):1287-1290. doi:10.3969/j.issn.2095-8552.2021.11.008. | |
| [18] | GRABOWSKI J P, MARTINEZ VILA C, RICHTER R, et al. Ki67 expression as a predictor of chemotherapy outcome in low-grade serous ovarian cancer[J]. Int J Gynecol Cancer, 2020, 30(4):498-503. doi:10.1136/ijgc-2019-000976. |
| [19] | LI J, POI M J, TSAI M D. Regulatory mechanisms of tumor suppressor P16(INK4A) and their relevance to cancer[J]. Biochemistry, 2011, 50(25):5566-5582. doi:10.1021/bi200642e. |
| [20] | COLLOCA G, VENTURINO A, GOVERNATO I. CA125-related tumor cell kinetics variables after chemotherapy in advanced ovarian cancer:a systematic review[J]. Clin Transl Oncol, 2016, 18(8):813-824. doi:10.1007/s12094-015-1441-5. |
| [21] | SONG Y J. Prediction of optimal debulking surgery in ovarian cancer[J]. Gland Surg, 2021, 10(3):1173-1181. doi:10.21037/gs-2019-ursoc-08. |
| [22] | ŠPACIR PRSKALO Z, BULIĆ P, LANGER S, et al. Proofs for implementation of higher HE4 and ROMA index cut-off values in ovarian cancer preoperative stratification[J]. J Obstet Gynaecol, 2019, 39(2):195-201. doi:10.1080/01443615.2018.1476471. |
| [23] | BACALBASA N, DIMA S, BALESCU I, et al. Results of primary cytoreductive surgery in advanced-stage epithelial ovarian cancer: a single-center experience[J]. Anticancer Res, 2015, 35(7):4099-4104. |
| [24] | PARASHKEVOVA A, SEHOULI J, RICHTER R, et al. Preoperative CA-125 value as a predictive factor for postoperative outcome in first relapse of platinum-sensitive serous ovarian cancer[J]. Anticancer Res, 2018, 38(8):4865-4870. doi:10.21873/anticanres.12799. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||