Tianjin Medical Journal ›› 2024, Vol. 52 ›› Issue (8): 845-849.doi: 10.11958/20231766
• Clinical Research • Previous Articles Next Articles
GUO Zhenjiang( ), ZHAO Guangyuan, DU Liqiang, LIU Fangzhen△()
), ZHAO Guangyuan, DU Liqiang, LIU Fangzhen△()
Received:2023-11-27
Revised:2024-01-17
Published:2024-08-15
Online:2024-08-16
Contact:
E-mail:GUO Zhenjiang, ZHAO Guangyuan, DU Liqiang, LIU Fangzhen. Development and validation of a preoperative nomogram predictive model for proximal gastric cancer with microscopic positive margin[J]. Tianjin Medical Journal, 2024, 52(8): 845-849.
CLC Number:
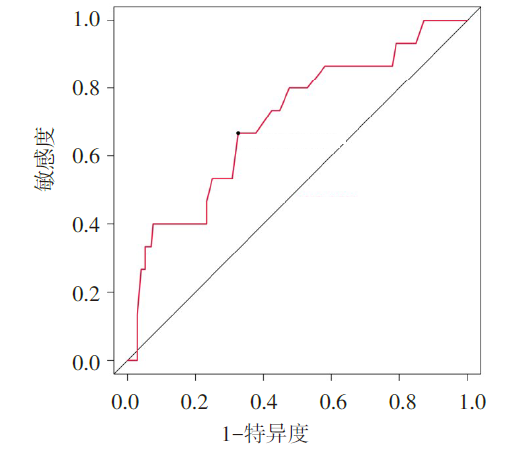
Fig.1 ROC curve of tumor size predicted positive margin of proximal gastric cancer
| 变量 | 上切缘R1组 (n=15) | 上切缘R0组 (n=172) | Z或χ2 |
|---|---|---|---|
| 年龄/岁 | 65.6(59.0,72.8) | 65.3(56.0,74.0) | 0.144 |
| 性别 | |||
| 男 | 10(66.7) | 103(59.9) | 0.265 |
| 女 | 5(33.3) | 69(40.1) | |
| 肿瘤长度 | |||
| ≤4.85 cm | 5(33.3) | 116(67.4) | 7.028** |
| >4.85 cm | 10(66.7) | 56(32.6) | |
| 肿瘤位置 | |||
| 非EGJ癌 | 10(66.7) | 149(86.6) | 4.318* |
| EGJ癌 | 5(33.3) | 23(13.4) | |
| Borrmann分型 | |||
| Ⅰ—Ⅱ | 3(20.0) | 82(47.7) | 4.262* |
| Ⅲ—Ⅳ | 12(80.0) | 90(52.3) | |
| 肿瘤分化 | |||
| 高-中分化 | 3(20.0) | 53(30.8) | 0.769 |
| 低-未分化 | 12(80.0) | 119(69.2) | |
| Lauren分型 | |||
| 肠型 | 5(33.3) | 108(62.8) | 5.007* |
| 弥漫型/混合型 | 10(66.7) | 64(37.2) | |
| cT分期 | |||
| cT2—3 | 6(40.0) | 119(69.1) | 5.303* |
| cT4 | 9(60.0) | 53(30.9) | |
| cN分期 | |||
| cN0 | 7(46.7) | 124(70.1) | 4.252* |
| cN+ | 8(53.3) | 48(29.9) |
Tab.1 Univariate analysis of preoperative variables with positive upper margin of proximal gastric cancer
| 变量 | 上切缘R1组 (n=15) | 上切缘R0组 (n=172) | Z或χ2 |
|---|---|---|---|
| 年龄/岁 | 65.6(59.0,72.8) | 65.3(56.0,74.0) | 0.144 |
| 性别 | |||
| 男 | 10(66.7) | 103(59.9) | 0.265 |
| 女 | 5(33.3) | 69(40.1) | |
| 肿瘤长度 | |||
| ≤4.85 cm | 5(33.3) | 116(67.4) | 7.028** |
| >4.85 cm | 10(66.7) | 56(32.6) | |
| 肿瘤位置 | |||
| 非EGJ癌 | 10(66.7) | 149(86.6) | 4.318* |
| EGJ癌 | 5(33.3) | 23(13.4) | |
| Borrmann分型 | |||
| Ⅰ—Ⅱ | 3(20.0) | 82(47.7) | 4.262* |
| Ⅲ—Ⅳ | 12(80.0) | 90(52.3) | |
| 肿瘤分化 | |||
| 高-中分化 | 3(20.0) | 53(30.8) | 0.769 |
| 低-未分化 | 12(80.0) | 119(69.2) | |
| Lauren分型 | |||
| 肠型 | 5(33.3) | 108(62.8) | 5.007* |
| 弥漫型/混合型 | 10(66.7) | 64(37.2) | |
| cT分期 | |||
| cT2—3 | 6(40.0) | 119(69.1) | 5.303* |
| cT4 | 9(60.0) | 53(30.9) | |
| cN分期 | |||
| cN0 | 7(46.7) | 124(70.1) | 4.252* |
| cN+ | 8(53.3) | 48(29.9) |
| 变量 | 变量类型 | 变量赋值 |
|---|---|---|
| 上切缘状态 | 因变量 | R0=0,R1=1 |
| 肿瘤长度 | 自变量 | ≤4.85 cm=0,>4.85 cm=1 |
| 肿瘤位置 | 自变量 | 非EGJ癌=0,EGJ癌=1 |
| Borrmann分型 | 自变量 | Ⅰ—Ⅱ型=0,Ⅲ—Ⅳ型=1 |
| Lauren分型 | 自变量 | 肠型=0,弥漫型/混合型=1 |
| cT分期 | 自变量 | cT2—3期=0,cT4期=1 |
| cN分期 | 自变量 | cN0期=0,cN+期=1 |
Tab.2 Variable assignment table
| 变量 | 变量类型 | 变量赋值 |
|---|---|---|
| 上切缘状态 | 因变量 | R0=0,R1=1 |
| 肿瘤长度 | 自变量 | ≤4.85 cm=0,>4.85 cm=1 |
| 肿瘤位置 | 自变量 | 非EGJ癌=0,EGJ癌=1 |
| Borrmann分型 | 自变量 | Ⅰ—Ⅱ型=0,Ⅲ—Ⅳ型=1 |
| Lauren分型 | 自变量 | 肠型=0,弥漫型/混合型=1 |
| cT分期 | 自变量 | cT2—3期=0,cT4期=1 |
| cN分期 | 自变量 | cN0期=0,cN+期=1 |
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| 肿瘤长度 | 1.386 | 0.688 | 4.063 | 0.044 | 4.000(1.039~15.399) |
| 肿瘤位置 | 1.961 | 0.760 | 6.667 | 0.010 | 7.108(1.604~31.494) |
| Borrmann分型 | 1.945 | 0.773 | 6.334 | 0.012 | 6.991(1.538~31.782) |
| Lauren分型 | 2.026 | 0.730 | 7.706 | 0.006 | 7.583(1.814~31.701) |
| cT分期 | 2.110 | 0.752 | 7.876 | 0.005 | 8.249(1.890~36.007) |
| 常数项 | -6.895 | 1.262 | 29.830 | <0.001 | 0.001 |
Tab.3 Multivariate analysis of preoperative variables with positive uppermargin of proximal gastric cancer
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| 肿瘤长度 | 1.386 | 0.688 | 4.063 | 0.044 | 4.000(1.039~15.399) |
| 肿瘤位置 | 1.961 | 0.760 | 6.667 | 0.010 | 7.108(1.604~31.494) |
| Borrmann分型 | 1.945 | 0.773 | 6.334 | 0.012 | 6.991(1.538~31.782) |
| Lauren分型 | 2.026 | 0.730 | 7.706 | 0.006 | 7.583(1.814~31.701) |
| cT分期 | 2.110 | 0.752 | 7.876 | 0.005 | 8.249(1.890~36.007) |
| 常数项 | -6.895 | 1.262 | 29.830 | <0.001 | 0.001 |
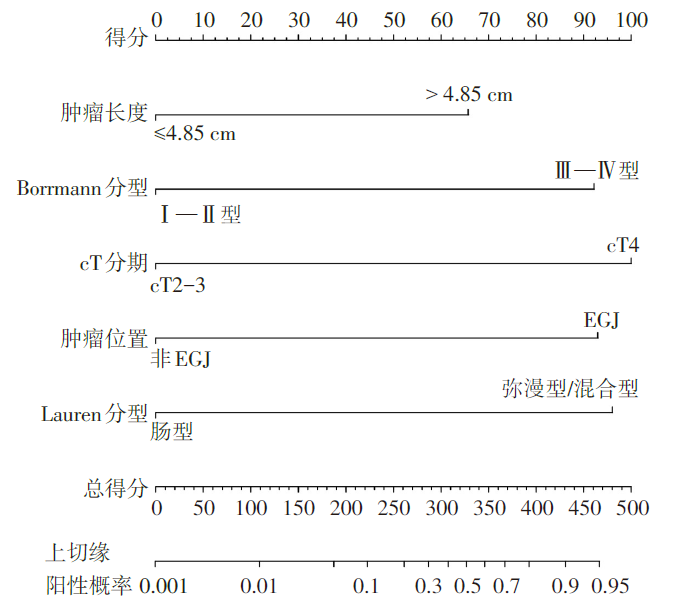
Fig.2 Nomogram for positive upper margin of proximal gastric cancer based on preoperative clinicopathological variables
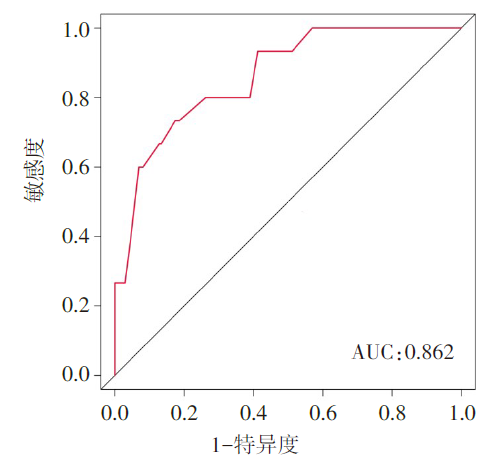
Fig.3 ROC curves of nomogram predicted positive margin of proximal gastric cancer
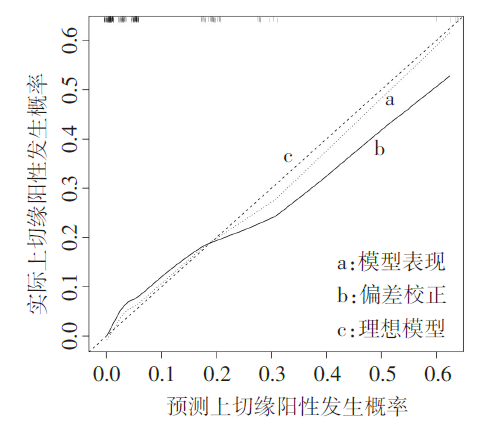
Fig.4 Calibration curve of the nomogram
| [1] | RAWLA P, BARSOUK A. Epidemiology of gastric cancer:global trends,risk factors and prevention[J]. Prz Gastroenterol, 2019, 14(1):26-38. doi:10.5114/pg.2018.80001. |
| [2] | 马岩, 薛英威. 胃上部癌手术消化道重建方式的选择[J]. 中华胃肠外科杂志, 2022, 25(5):396-400. |
| MA Y, XUE Y W. Choice of digestive tract reconstruction in upper gastric cancer[J]. Chin J Gastrointest Surg, 2022, 25(5):396-400. doi:10.3760/cma.j.cn441530-20220308-00092. | |
| [3] | KUMAZU Y, HAYASHI T, YOSHIKAWA T, et al. Risk factors analysis and stratification for microscopically positive resection margin in gastric cancer patients[J]. BMC Surg, 2020, 20(1):95. doi:10.1186/s12893-020-00744-5. |
| [4] | VAN DER WERF L R, CORDS C, ARNTZ I, et al. Population-based study on risk factors for tumor-positive resection margins in patients with gastric cancer[J]. Ann Surg Oncol, 2019, 26(7):2222-2233. doi:10.1245/s10434-019-07381-0. |
| [5] | NICLAUSS N, JUNG M K, CHEVALLAY M, et al. Minimal length of proximal resection margin in adenocarcinoma of the esophagogastric junction:a systematic review of the literature[J]. Updates Surg, 2019, 71(3):401-409. doi:10.1007/s13304-019-00665-w. |
| [6] | FENG F, TIAN Y, XU G, et al. The length of proximal margin does not influence the prognosis of Siewert type Ⅱ/Ⅲ adenocarcinoma of esophagogastric junction after transhiatal curative gastrectomy[J]. Springerplus, 2016,5:588. doi:10.1186/s40064-016-2240-3. |
| [7] | 黄庆峰, 杨立成, 吴建军. 影响Lauren分型胃癌患者行根治术治疗后早期复发的因素分析[J]. 中国中西医结合外科杂志, 2022, 28(3):325-330. |
| HUANG Q F, YANG L C, WU J J. Analysis of factors influencing early recurrence of lauren type gastric cancer after radical resection[J]. Chinese Journal of Integrated Traditional Chinese and Western Medicine Surgery, 2022, 28(3):325-330. doi:10.3969/j.issn.1007-6948.2022.03.008. | |
| [8] | 郭振江, 赵光远, 杜立强, 等. 进展期胃癌脉管侵犯术前列线图预测模型的建立和验证[J]. 天津医药, 2023, 51(12):1382-1386. |
| GUO Z J, ZHAO G Y, DU L Q, et al. Establishment and validation of a predictive nomogram model for advanced gastric cancer with lymphovascular invasion[J]. Tianjin Med J, 2023, 51(12):1382-1386. doi:10.11958/20230513. | |
| [9] | GUO Z, GUO H, TIAN Y, et al. Nomograms for predicting disease-free survival in patients with siewert type II/III adenocarcinoma of the esophagogastric junction receiving neoadjuvant therapy and radical surgery[J]. Front Oncol, 2022, 12:908229. doi:10.3389/fonc.2022.908229. |
| [10] | CHO B C, JEUNG H C, CHOI H J, et al. Prognostic impact of resection margin involvement after extended(D2/D3)gastrectomy for advanced gastric cancer:a 15-year experience at a single institute[J]. J Surg Oncol, 2007, 95(6):461-468. doi:10.1002/jso.20731. |
| [11] | MORGAGNI P, GARCEA D, MARRELLI D, et al. Resection line involvement after gastric cancer surgery:clinical outcome in nonsurgically retreated patients[J]. World J Surg, 2008, 32(12):2661-2667. doi:10.1007/s00268-008-9747-x. |
| [12] | NAGATA T, ICHIKAWA D, KOMATSU S, et al. Prognostic impact of microscopic positive margin in gastric cancer patients[J]. J Surg Oncol, 2011, 104(6):592-597. doi:10.1002/jso.22022. |
| [13] | WOO J W, RYU K W, PARK J Y, et al. Prognostic impact of microscopic tumor involved resection margin in advanced gastric cancer patients after gastric resection[J]. World J Surg, 2014, 38(2):439-446. doi:10.1007/s00268-013-2301-5. |
| [14] | IWATSUKI M, MATSUMOTO C, MIMORI K, et al. The comprehensive review of gastric adenocarcinoma and proximal polyposis of the stomach(GAPPS)from diagnosis and treatment[J]. Ann Gastroenterol Surg, 2023, 7(5):725-732. doi:10.1002/ags3.12708. |
| [15] | Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014(ver. 4)[J]. Gastric Cancer,2017, 20(1):1-19. doi:10.1007/s10120-016-0622-4. |
| [16] | 中华医学会外科学分会腹腔镜与内镜外科学组. Siewert Ⅱ型食管胃结合部腺癌腔镜手术治疗中国专家共识(2023版)[J]. 中华消化外科杂志, 2023, 22(7):799-809. |
| Chinese Society of Laparoscopic and Endoscopic Surgery,Chinese Surgical Society, Chinese Medical Association. Chinese expert consensus on endoscopic surgery for Siewert Ⅱ adenocarcinoma of esophagogastric junction(2023 edition)[J]. Chin J Dig Surg, 2023, 22(7):799-809. doi:10.3760/cma.j.cn115610-20230628-00320. | |
| [17] | MINE S, SANO T, HIKI N, et al. Proximal margin length with transhiatal gastrectomy for Siewert type Ⅱ and III adenocarcinomas of the oesophagogastric junction[J]. Br J Surg, 2013, 100(8):1050-1054. doi:10.1002/bjs.9170. |
| [18] | LEE J H, KIM Y I. Which is the optimal extent of resection in middle third gastric cancer between total gastrectomy and subtotal gastrectomy?[J]. J Gastric Cancer, 2010, 10(4):226-233. doi:10.5230/jgc.2010.10.4.226. |
| [19] | BISSOLATI M, DESIO M, ROSA F, et al. Risk factor analysis for involvement of resection margins in gastric and esophagogastric junction cancer:an Italian multicenter study[J]. Gastric Cancer, 2017, 20(1):70-82. doi:10.1007/s10120-015-0589-6. |
| [20] | GIANDOLA T, MAINO C, MARRAPODI G, et al. Imaging in gastric cancer:current practice and future perspectives[J]. Diagnostics(Basel), 2023, 13(7):1276. doi:10.3390/diagnostics13071276. |
| [21] | WANI A H, PARRY A H, FEROZ I, et al. Preoperative staging of gastric cancer using computed tomography and its correlation with histopathology with emphasis on multi-planar reformations and virtual gastroscopy[J]. J Gastrointest Cancer, 2021, 52(2):606-615. doi:10.1007/s12029-020-00436-6. |
| [22] | JIANG Z Y, KINAMI S, NAKAMURA N, et al. Diagnostic ability of multi-detector spiral computed tomography for pathological lymph node metastasis of advanced gastric cancer[J]. World J Gastrointest Oncol, 2020, 12(4):435-446. doi:10.4251/wjgo.v12.i4.435. |
| [23] | LEE J H, AHN S H, PARK D J, et al. Clinical impact of tumor infiltration at the transected surgical margin during gastric cancer surgery[J]. J Surg Oncol, 2012, 106(6):772-776. doi:10.1002/jso.23123. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||