Tianjin Medical Journal ›› 2022, Vol. 50 ›› Issue (9): 953-958.doi: 10.11958/20212745
• Clinical Research • Previous Articles Next Articles
WANG Le( ), CHEN Xing, LIANG Maoli, ZHANG Jing, WANG Yan, CHEN Baoyuan, CAO Jie()
), CHEN Xing, LIANG Maoli, ZHANG Jing, WANG Yan, CHEN Baoyuan, CAO Jie()
Received:2021-12-13
Revised:2022-02-25
Published:2022-09-15
Online:2022-09-05
Contact:
CAO Jie
E-mail:2629411288@qq.com;tjcaojie@163.com
WANG Le, CHEN Xing, LIANG Maoli, ZHANG Jing, WANG Yan, CHEN Baoyuan, CAO Jie. Analysis of influencing factors and predictive indicators of obstructive sleep apnea combined with obesity-related sleep hypoventilation[J]. Tianjin Medical Journal, 2022, 50(9): 953-958.
CLC Number:
| 组别 | n | 男性 | 年龄(岁) | 颈围(cm) | 腰围(cm) | BMI(kg/m2) | 吸烟史 | 饮酒史 | 高血压 | 冠心病 | 糖尿病 | 脑卒中 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单纯OSA组 | 109 | 77(70.6) | 45.3±12.3 | 43.8±7.6 | 111.2±10.8 | 33.6±3.1 | 38(34.8) | 44(40.3) | 59(54.1) | 15(13.8) | 25(22.9) | 4(3.6) |
| OSA合并ORSH组 | 46 | 39(84.7) | 42.4±14.4 | 43.8±2.9 | 115.5±11.3 | 34.6±4.9 | 18(39.1) | 18(39.1) | 21(45.6) | 7(15.2) | 11(23.9) | 2(4.3) |
| OSA合并OHS组 | 30 | 19(70.3) | 49.3±11.9 | 45.8±3.6 | 122.7±15.0ab | 36.8±6.2ab | 14(46.6) | 13(43.3) | 18(60.0) | 5(16.6) | 7(23.3) | 5(16.6)ab |
| χ2或F | 4.967 | 2.626 | 1.273 | 6.340** | 6.713** | 1.437 | 0.136 | 1.619 | 0.178 | 0.017 | 7.385* |
Tab.1 Comparison of basic data between the three groups of patients
| 组别 | n | 男性 | 年龄(岁) | 颈围(cm) | 腰围(cm) | BMI(kg/m2) | 吸烟史 | 饮酒史 | 高血压 | 冠心病 | 糖尿病 | 脑卒中 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单纯OSA组 | 109 | 77(70.6) | 45.3±12.3 | 43.8±7.6 | 111.2±10.8 | 33.6±3.1 | 38(34.8) | 44(40.3) | 59(54.1) | 15(13.8) | 25(22.9) | 4(3.6) |
| OSA合并ORSH组 | 46 | 39(84.7) | 42.4±14.4 | 43.8±2.9 | 115.5±11.3 | 34.6±4.9 | 18(39.1) | 18(39.1) | 21(45.6) | 7(15.2) | 11(23.9) | 2(4.3) |
| OSA合并OHS组 | 30 | 19(70.3) | 49.3±11.9 | 45.8±3.6 | 122.7±15.0ab | 36.8±6.2ab | 14(46.6) | 13(43.3) | 18(60.0) | 5(16.6) | 7(23.3) | 5(16.6)ab |
| χ2或F | 4.967 | 2.626 | 1.273 | 6.340** | 6.713** | 1.437 | 0.136 | 1.619 | 0.178 | 0.017 | 7.385* |
| 组别 | n | pH值 | p(O2)(mmHg) | ||
|---|---|---|---|---|---|
| 单纯OSA组 | 109 | 7.41±0.02 | 75.43±9.24 | ||
| OSA合并ORSH组 | 46 | 7.41±0.02 | 73.20±7.82 | ||
| OSA合并OHS组 | 30 | 7.39±0.03 | 68.90±8.51a | ||
| F | 5.477 | 6.567** | |||
| 组别 | p(CO2)(mmHg) | HCO3-(mmol/L) | |||
| 单纯OSA组 | 39.86±2.89 | 24.53±1.87 | |||
| OSA合并ORSH组 | 41.57±2.34a | 25.60±1.67a | |||
| OSA合并OHS组 | 50.60±10.24ab | 31.86±12.42ab | |||
| F | 59.296** | 23.261** | |||
Tab.2 Comparison of arterial blood gases between the three groups of patients
| 组别 | n | pH值 | p(O2)(mmHg) | ||
|---|---|---|---|---|---|
| 单纯OSA组 | 109 | 7.41±0.02 | 75.43±9.24 | ||
| OSA合并ORSH组 | 46 | 7.41±0.02 | 73.20±7.82 | ||
| OSA合并OHS组 | 30 | 7.39±0.03 | 68.90±8.51a | ||
| F | 5.477 | 6.567** | |||
| 组别 | p(CO2)(mmHg) | HCO3-(mmol/L) | |||
| 单纯OSA组 | 39.86±2.89 | 24.53±1.87 | |||
| OSA合并ORSH组 | 41.57±2.34a | 25.60±1.67a | |||
| OSA合并OHS组 | 50.60±10.24ab | 31.86±12.42ab | |||
| F | 59.296** | 23.261** | |||
| 组别 | n | FVC% | FEV1% |
|---|---|---|---|
| 单纯OSA组 | 109 | 95.9±14.5 | 93.8±13.9 |
| OSA合并ORSH组 | 46 | 93.4±13.2 | 91.5±13.8 |
| OSA合并OHS组 | 30 | 80.3±18.4ab | 79.7±21.0ab |
| F | 12.915** | 10.085** |
Tab.3 Comparison of lung function between the three groups of patients
| 组别 | n | FVC% | FEV1% |
|---|---|---|---|
| 单纯OSA组 | 109 | 95.9±14.5 | 93.8±13.9 |
| OSA合并ORSH组 | 46 | 93.4±13.2 | 91.5±13.8 |
| OSA合并OHS组 | 30 | 80.3±18.4ab | 79.7±21.0ab |
| F | 12.915** | 10.085** |
| 组别 | n | ESS(分) | ODI(次/h) | AHI(次/h) | MAI(次/h) | AI(次/h) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单纯OSA组 | 109 | 8.0(3.0,14.0) | 55.7(25.9,77.0) | 64.7(26.4,82.8) | 31.6(15.6,54.3) | 24.4(3.7,64.8) | ||||||||||
| OSA合并ORSH组 | 46 | 9.0(5.0,14.0) | 70.3(60.0,93.0)a | 77.6(64.9,91.0)a | 43.9(30.2,62.5)a | 54.3(21.2,75.2)a | ||||||||||
| OSA合并OHS组 | 30 | 14.0(7.0,19.0)a | 82.4(55.0,91.9)a | 82.8(71.8,96.8)a | 56.0(28.6,69.7)a | 61.3(18.0,79.8)a | ||||||||||
| χ2 | 7.299* | 20.876** | 17.498** | 11.893* | 10.594* | |||||||||||
| 组别 | MAT(s) | LAT(s) | HI(次/h) | MHT(s) | LHT(s) | |||||||||||
| 单纯OSA组 | 18.0(14.5,24.6) | 36.5(23.5,57.5) | 17.4(8.2,30.8) | 20.7(18.2,25.1) | 52.0(36.8,67.0) | |||||||||||
| OSA合并ORSH组 | 23.5(19.9,28.2)a | 63.0(49.9,88.8)a | 18.6(5.6,48.0) | 20.6(17.0,24.8) | 48.5(39.9,64.4) | |||||||||||
| OSA合并OHS组 | 21.8(18.1,27.8)a | 71.5(45.8,89.1)a | 15.3(4.4,41.4) | 20.9(18.6,23.2) | 53.5(37.3,65.6) | |||||||||||
| χ2 | 17.640** | 37.419** | 0.184 | 0.442 | 0.265 | |||||||||||
| 组别 | minSpO2 | meanSpO2 | T90(%) | CPAP | BI-PAP | |||||||||||
| 单纯OSA组 | 0.75(0.61,0.83) | 0.93(0.91,0.95) | 9.4(1.2,35.2) | 97(88.9) | 5(4.5) | |||||||||||
| OSA合并ORSH组 | 0.60(0.49,0.68)a | 0.91(0.88,0.93)a | 29.6(19.3,45.6)a | 41(89.2) | 5(10.8)a | |||||||||||
| OSA合并OHS组 | 0.50(0.40,0.66)a | 0.89(0.85,0.90)a | 52.3(30.2,66.3)a | 20(66.7)ab | 10(33.3)ab | |||||||||||
| χ2 | 45.816** | 34.382** | 35.501** | 10.088** | 20.162** | |||||||||||
Tab.4 Comparison of PSG indexes between the three groups of patients
| 组别 | n | ESS(分) | ODI(次/h) | AHI(次/h) | MAI(次/h) | AI(次/h) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单纯OSA组 | 109 | 8.0(3.0,14.0) | 55.7(25.9,77.0) | 64.7(26.4,82.8) | 31.6(15.6,54.3) | 24.4(3.7,64.8) | ||||||||||
| OSA合并ORSH组 | 46 | 9.0(5.0,14.0) | 70.3(60.0,93.0)a | 77.6(64.9,91.0)a | 43.9(30.2,62.5)a | 54.3(21.2,75.2)a | ||||||||||
| OSA合并OHS组 | 30 | 14.0(7.0,19.0)a | 82.4(55.0,91.9)a | 82.8(71.8,96.8)a | 56.0(28.6,69.7)a | 61.3(18.0,79.8)a | ||||||||||
| χ2 | 7.299* | 20.876** | 17.498** | 11.893* | 10.594* | |||||||||||
| 组别 | MAT(s) | LAT(s) | HI(次/h) | MHT(s) | LHT(s) | |||||||||||
| 单纯OSA组 | 18.0(14.5,24.6) | 36.5(23.5,57.5) | 17.4(8.2,30.8) | 20.7(18.2,25.1) | 52.0(36.8,67.0) | |||||||||||
| OSA合并ORSH组 | 23.5(19.9,28.2)a | 63.0(49.9,88.8)a | 18.6(5.6,48.0) | 20.6(17.0,24.8) | 48.5(39.9,64.4) | |||||||||||
| OSA合并OHS组 | 21.8(18.1,27.8)a | 71.5(45.8,89.1)a | 15.3(4.4,41.4) | 20.9(18.6,23.2) | 53.5(37.3,65.6) | |||||||||||
| χ2 | 17.640** | 37.419** | 0.184 | 0.442 | 0.265 | |||||||||||
| 组别 | minSpO2 | meanSpO2 | T90(%) | CPAP | BI-PAP | |||||||||||
| 单纯OSA组 | 0.75(0.61,0.83) | 0.93(0.91,0.95) | 9.4(1.2,35.2) | 97(88.9) | 5(4.5) | |||||||||||
| OSA合并ORSH组 | 0.60(0.49,0.68)a | 0.91(0.88,0.93)a | 29.6(19.3,45.6)a | 41(89.2) | 5(10.8)a | |||||||||||
| OSA合并OHS组 | 0.50(0.40,0.66)a | 0.89(0.85,0.90)a | 52.3(30.2,66.3)a | 20(66.7)ab | 10(33.3)ab | |||||||||||
| χ2 | 45.816** | 34.382** | 35.501** | 10.088** | 20.162** | |||||||||||
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| AHI | 0.013 | 0.008 | 2.508 | 0.113 | 1.013(0.997,1.030) |
| LAT | 0.028 | 0.009 | 10.572 | 0.001 | 1.029(1.011,1.046) |
| meanSpO2 | -0.001 | 0.063 | 0.000 | 0.984 | 0.999(0.883,1.129) |
| HCO3- | 0.267 | 0.119 | 5.065 | 0.024 | 1.306(1.035,1.648) |
| 常量 | -9.897 | 7.230 | 1.874 | 0.171 | - |
Tab.5 Multiple-factor Logistic regression analysis of factors affecting ORSH in patients with OSA
| 变量 | β | SE | Wald χ2 | P | OR(95%CI) |
|---|---|---|---|---|---|
| AHI | 0.013 | 0.008 | 2.508 | 0.113 | 1.013(0.997,1.030) |
| LAT | 0.028 | 0.009 | 10.572 | 0.001 | 1.029(1.011,1.046) |
| meanSpO2 | -0.001 | 0.063 | 0.000 | 0.984 | 0.999(0.883,1.129) |
| HCO3- | 0.267 | 0.119 | 5.065 | 0.024 | 1.306(1.035,1.648) |
| 常量 | -9.897 | 7.230 | 1.874 | 0.171 | - |
| 指标 | AUC | AUC 95%CI | 截断值 | SE | P | 敏感度 | 特异度 |
|---|---|---|---|---|---|---|---|
| LAT | 0.759 | 0.679~0.839 | 48.250 s | 0.041 | <0.001 | 0.804 | 0.633 |
| HCO3- | 0.666 | 0.575~0.758 | 24.950 mmol/L | 0.047 | 0.001 | 0.674 | 0.615 |
| LAT和HCO3-联合 | 0.784 | 0.712~0.856 | -2.176 | 0.037 | <0.001 | 0.913 | 0.541 |
Tab.6 The predictive efficiency of LAT and HCO3- levels analyzed by ROC for OSA patients combined with ORSH
| 指标 | AUC | AUC 95%CI | 截断值 | SE | P | 敏感度 | 特异度 |
|---|---|---|---|---|---|---|---|
| LAT | 0.759 | 0.679~0.839 | 48.250 s | 0.041 | <0.001 | 0.804 | 0.633 |
| HCO3- | 0.666 | 0.575~0.758 | 24.950 mmol/L | 0.047 | 0.001 | 0.674 | 0.615 |
| LAT和HCO3-联合 | 0.784 | 0.712~0.856 | -2.176 | 0.037 | <0.001 | 0.913 | 0.541 |
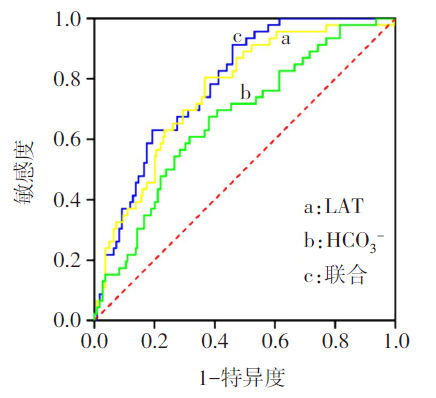
Fig.1 ROC curves of LAT and HCO3- levels for predicting OSA combined with ORSH
| [1] | 罗金梅, 肖毅. 肥胖低通气综合征:需要早期诊断和正确的治疗[J]. 中华结核与呼吸杂志, 2016, 39(8):585-587. |
| LUO J M, XIAO Y. Obesity hypopnea syndrome:Early diagnosis and correct treatment[J]. Chin J Tuberc Respir Dis, 2016, 39(8):585-587. doi: 10.3760/cma.j.issn.1001-0939.2016.08.006. | |
| [2] | PIPER A J, GRUNSTEIN R R. Big breathing:The complex interaction of obesity,hypoventilation,weight loss,and respiratory function[J]. J Appl Physiol(1985), 2010, 108(1):199-205. doi: 10.1152/japplphysiol.00713.2009. |
| [3] | PIPER A J, GRUNSTEIN R R. Obesity hypoventilation syndrome:mechanisms and management[J]. Am J Respir Crit Care Med, 2011, 183(3):292-298. doi: 10.1164/rccm.201008-1280CI. |
| [4] | RANDERATH W, VERBRAECKEN J, ANDREAS S, et al. Definition,discrimination,diagnosis and treatment of central breathing disturbances during sleep[J]. Eur Respir J, 2017, 49(1):1600959. doi: 10.1183/13993003.00959-2016. |
| [5] | CASTRO-AÑÓN O, PÉREZ DE LLANO L A, DE LA FUENTE SÁNCHEZ S, et al. Obesity-hypoventilation syndrome:Increased risk of death over sleep apnea syndrome[J]. PLoS One, 2015, 10(2):e0117808. doi: 10.1371/journal.pone.0117808. |
| [6] | JENNUM P, IBSEN R, KJELLBERG J. Morbidity prior to a diagnosis of sleep-disordered breathing:A controlled national study[J]. J Clin Sleep Med, 2013, 9(2):103-108. doi: 10.5664/jcsm.2398. |
| [7] | 中华医学会呼吸病学分会睡眠呼吸障碍学组. 阻塞性睡眠呼吸暂停低通气综合征诊治指南(2011年修订版)[J]. 中华结核与呼吸杂志, 2012, 35(1):9-12. |
| Sleep disorders group,respiratory branch, Chinese Medical Association. Guidelines for the diagnosis and treatment of obstructive sleep apnea hypopnea syndrome(2011 revision)[J]. Chin J Tuberc Respir Dis, 2012, 35(1):9-12. doi: 10.3760/cma.j.issn.1001-0939.2012.01.007. | |
| [8] | KUSHIDA C A, CHEDIAK A, BERRY R B, et al. Clinical guidelines for the manual titration of positive airway pressure in patients with obstructive sleep apnea[J]. J Clin Sleep Med, 2008, 4(2):157-171. |
| [9] | BERRY R B, BUDHIRAJA R, GOTTLIEB D J, et al. Rules for scoring respiratory events in sleep:update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine[J]. J Clin Sleep Med, 2012, 8(5):597-619. doi: 10.5664/jcsm.2172. |
| [10] | WANG Y, WANG L, QU W. New national data show alarming increase in obesity and noncommunicable chronic diseases in China[J]. Eur J Clin Nutr, 2017, 71(1):149-150. doi: 10.1038/ejcn.2016.171. |
| [11] | GOYAL A, PAKHARE A, TIWARI I R, et al. Diagnosing obstructive sleep apnea patients with isolated nocturnal hypoventilation and defining obesity hypoventilation syndrome using new European Respiratory Society classification criteria:an Indian perspective[J]. Sleep Med, 2020, 66:85-91. doi: 10.1016/j.sleep.2019.08.009. |
| [12] | NOWBAR S, BURKART K M, GONZALES R, et al. Obesity-associated hypoventilation in hospitalized patients:Prevalence,effects,and outcome[J]. Am J Med, 2004, 116(1):1-7. doi: 10.1016/j.amjmed.2003.08.022. |
| [13] | SIVAM S, YEE B, WONG K, et al. Obesity hypoventilation syndrome:Early detection of nocturnal-only hypercapnia in an obese population[J]. J Clin Sleep Med, 2018, 14(9):1477-1484. doi: 10.5664/jcsm.7318. |
| [14] | PERGER E, ARON-WISNEWSKY J, ARNULF I, et al. Diagnostic approach to sleep disordered-breathing among patients with grade Ⅲ obesity[J]. Sleep Med, 2021, 82:18-22. doi: 10.1016/j.sleep.2021.03.024. |
| [15] | 李宁, 李庆云. 阻塞性睡眠呼吸暂停患者呼吸暂停与睡眠期二氧化碳的变化分析[C]// . 中国睡眠研究会第十一届全国学术年会论文集,济南, 2019:104. |
| LING N, LI Q Y. The analysis of changes of carbon dioxide and apnea during sleep in patients with obstructive sleep apnea[C]// . Proceedings of the 11th National Academic Annual Meeting of Sleep Research Association in China,Jinan, 2019:104. doi: 10.26914/c.cnkihy.2019.014436. | |
| [16] | JAIMCHARIYATAM N, DWEIK R A, KAW R, et al. Polysomnographic determinants of nocturnal hypercapnia in patients with sleep apnea[J]. J Clin Sleep Med, 2013, 9(3):209-215. doi: 10.5664/jcsm.2480. |
| [17] | AYAPPA I, BERGER K I, NORMAN R G, et al. Hypercapnia and ventilatory periodicity in obstructive sleep apnea syndrome[J]. Am J Respir Crit Care Med, 2002, 166(8):1112-1115. doi: 10.1164/rccm.200203-212OC. |
| [18] | BINGOL Z, PIHTILI A, CAGATAY P, et al. Clinical predictors of obesity hypoventilation syndrome in obese subjects with obstructive sleep apnea[J]. Respir Care, 2015, 60(5):666-672. doi: 10.4187/respcare.03733. |
| [19] | HART N, MANDAL S, MANUEL A, et al. Obesity hypoventilation syndrome:does the current definition need revisiting?[J]. Thorax, 2014, 69(1):83-84. doi: 10.1136/thoraxjnl-2013-204298. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||