Tianjin Medical Journal ›› 2024, Vol. 52 ›› Issue (7): 755-761.doi: 10.11958/20231546
• Clinical Research • Previous Articles Next Articles
LIU Chunwei1( ), YANG Fan2, HU Yuecheng1, ZHANG Jingxia1, CONG Hongliang1, LI Ximing1,∆()
), YANG Fan2, HU Yuecheng1, ZHANG Jingxia1, CONG Hongliang1, LI Ximing1,∆()
Received:2023-10-11
Revised:2023-11-10
Published:2024-07-15
Online:2024-07-11
Contact:
∆E-mail:liximing2816@163.com
LIU Chunwei, YANG Fan, HU Yuecheng, ZHANG Jingxia, CONG Hongliang, LI Ximing. Analysis of electrocardiographic features and in-hospital mortality in acute total left main artery occlusion and subtotal occlusion[J]. Tianjin Medical Journal, 2024, 52(7): 755-761.
CLC Number:
| 组别 | n | avR导联 ST段抬高 | avR+V1导联 ST段抬高 | Ⅰ、avL、V2—V5 导联ST段抬高 | avR+avL导联 ST段抬高 | QRS时限/ms | 左前分支 传导阻滞 | 完全性右束支 传导阻滞 | 左前分支+右束支 传导阻滞 |
|---|---|---|---|---|---|---|---|---|---|
| 次全闭塞组 | 99 | 59(59.6) | 30(30.3) | 7(7.1) | 3(3.0) | 94±13 | 13(13.1) | 1(1.0) | 0(0) |
| 完全闭塞组 | 94 | 12(12.8) | 5(5.3) | 51(54.3) | 26(27.7) | 117±23 | 32(34.0) | 5(5.3) | 18(19.1) |
| χ2或t | 45.473** | 20.273** | 51.069** | 22.908** | 8.375** | 11.792** | 2.972 | 20.907** | |
| 敏感度 | 0.13 | 0.05 | 0.54 | 0.28 | 0.34 | 0.05 | 0.19 | ||
| 特异度 | 0.40 | 0.70 | 0.93 | 0.97 | 0.87 | 0.99 | 1.00 |
Tab.1 Comparison of ECG features between LM total occlusion and subocclusion
| 组别 | n | avR导联 ST段抬高 | avR+V1导联 ST段抬高 | Ⅰ、avL、V2—V5 导联ST段抬高 | avR+avL导联 ST段抬高 | QRS时限/ms | 左前分支 传导阻滞 | 完全性右束支 传导阻滞 | 左前分支+右束支 传导阻滞 |
|---|---|---|---|---|---|---|---|---|---|
| 次全闭塞组 | 99 | 59(59.6) | 30(30.3) | 7(7.1) | 3(3.0) | 94±13 | 13(13.1) | 1(1.0) | 0(0) |
| 完全闭塞组 | 94 | 12(12.8) | 5(5.3) | 51(54.3) | 26(27.7) | 117±23 | 32(34.0) | 5(5.3) | 18(19.1) |
| χ2或t | 45.473** | 20.273** | 51.069** | 22.908** | 8.375** | 11.792** | 2.972 | 20.907** | |
| 敏感度 | 0.13 | 0.05 | 0.54 | 0.28 | 0.34 | 0.05 | 0.19 | ||
| 特异度 | 0.40 | 0.70 | 0.93 | 0.97 | 0.87 | 0.99 | 1.00 |
| 组别 | n | 年龄/岁 | 男性 | 高血压 | 糖尿病 | 吸烟史 | eGFR/[mL/(min·1.73 m2)] | LDL-C/(mmol/L) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 次全闭塞组 | 99 | 64.5±9.8 | 77(77.8) | 55(55.6) | 27(27.2) | 71(71.7) | 56.8±20.4 | 3.26±0.79 | ||||||||
| 完全闭塞组 | 94 | 60.8±13.0 | 80(85.1) | 55(58.5) | 29(30.9) | 73(77.7) | 58.4±21.1 | 3.28±0.87 | ||||||||
| t或χ2 | 2.258* | 1.707 | 0.129 | 0.016 | 0.899 | 0.528 | 0.184 | |||||||||
| 组别 | 发病时间/h | 休克 | IABP植入 | 机械通气 | 左主干病变部位 | 院内死亡 | ||||||||||
| 开口 | 左主干体部 | 分叉 | ||||||||||||||
| 次全闭塞组 | 4.4±2.8 | 17(17.1) | 71(71.7) | 19(19.2) | 10(10.1) | 41(41.4) | 48(48.5) | 14(14.1) | ||||||||
| 完全闭塞组 | 4.5±2.0 | 61(64.9) | 88(93.6) | 40(42.6) | 0(0) | 61(64.9) | 33(35.1) | 44(46.8) | ||||||||
| t或χ2 | 0.478 | 45.600** | 15.934** | 12.398** | 16.581** | 24.478** | ||||||||||
Tab.2 Comparison of clinical features between LM total occlusion and subocclusion
| 组别 | n | 年龄/岁 | 男性 | 高血压 | 糖尿病 | 吸烟史 | eGFR/[mL/(min·1.73 m2)] | LDL-C/(mmol/L) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 次全闭塞组 | 99 | 64.5±9.8 | 77(77.8) | 55(55.6) | 27(27.2) | 71(71.7) | 56.8±20.4 | 3.26±0.79 | ||||||||
| 完全闭塞组 | 94 | 60.8±13.0 | 80(85.1) | 55(58.5) | 29(30.9) | 73(77.7) | 58.4±21.1 | 3.28±0.87 | ||||||||
| t或χ2 | 2.258* | 1.707 | 0.129 | 0.016 | 0.899 | 0.528 | 0.184 | |||||||||
| 组别 | 发病时间/h | 休克 | IABP植入 | 机械通气 | 左主干病变部位 | 院内死亡 | ||||||||||
| 开口 | 左主干体部 | 分叉 | ||||||||||||||
| 次全闭塞组 | 4.4±2.8 | 17(17.1) | 71(71.7) | 19(19.2) | 10(10.1) | 41(41.4) | 48(48.5) | 14(14.1) | ||||||||
| 完全闭塞组 | 4.5±2.0 | 61(64.9) | 88(93.6) | 40(42.6) | 0(0) | 61(64.9) | 33(35.1) | 44(46.8) | ||||||||
| t或χ2 | 0.478 | 45.600** | 15.934** | 12.398** | 16.581** | 24.478** | ||||||||||
| 组别 | n | 年龄/岁 | 男性 | 高血压 | 糖尿病 | 吸烟史 | eGFR/ [mL/(min·1.73 m2)] | LDL-C/ (mmol/L) | 休克 | 发病 时间/h | 侧支 循环 | IABP 植入 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 存活组 | 50 | 58.9±13.9 | 43(86.0) | 2(54.0) | 13(26.0) | 38(76.0) | 58.8±22.3 | 3.36±0.84 | 20(40.0) | 3.7±2.1 | 29(58.0) | 46(92.0) | ||||||||||||||||||||
| 死亡组 | 44 | 62.9±11.8 | 37(84.1) | 28(63.6) | 16(36.4) | 35(79.5) | 52.0±18.7 | 3.18±0.90 | 41(93.2) | 4.3±3.3 | 9(20.5) | 42(95.5) | ||||||||||||||||||||
| t或χ2 | 1.513 | 0.067 | 0.895 | 1.178 | 0.170 | 1.587 | 1.067 | 29.056** | 0.937 | 14.756** | 0.467 | |||||||||||||||||||||
| 组别 | 机械 通气 | 血栓 抽吸 | 右冠状动脉 严重狭窄 | 右冠状动脉同期PCI | 左主干病变部位 | avR导联(包括avR+ V1导联)ST段抬高 | Ⅰ、avL、V2—V5 导联ST段抬高 | avR+avL导 联ST段抬高 | ||||||||||||||||||||||||
| 开口 | 左主干体部 | 分叉 | ||||||||||||||||||||||||||||||
| 存活组 | 17(34.0) | 14(28.0) | 13(26.0) | 3(6.0) | 0(0) | 31(62.0) | 19(38.0) | 14(28.0) | 17(34.0) | 19(38.0) | ||||||||||||||||||||||
| 死亡组 | 23(52.3) | 13(29.5) | 8(18.2) | 1(2.3) | 0(0) | 30(68.2) | 14(31.8) | 3(6.8) | 34(77.3) | 7(15.9) | ||||||||||||||||||||||
| χ2 | 3.197 | 0.027 | 0.825 | 0.798 | 0.393 | 7.088** | 17.658** | 5.708* | ||||||||||||||||||||||||
| 组别 | QRS时限/ms | 左前分支 传导阻滞 | 完全性右束支 传导阻滞 | 左前分支+右束支 传导阻滞 | 发病年度 | |||||||||||||||||||||||||||
| 2001—2006 | 2007—2012 | 2013—2018 | 2019—2023 | |||||||||||||||||||||||||||||
| 存活组 | 111±23 | 18(36.0) | 2(4.0) | 6(12.0) | 10(20.0) | 11(22.0) | 15(30.0) | 14(28.0) | ||||||||||||||||||||||||
| 死亡组 | 122±23 | 14(31.8) | 3(6.8) | 12(27.3) | 9(20.5) | 12(27.3) | 13(29.5) | 10(22.7) | ||||||||||||||||||||||||
| t或χ2 | 2.280* | 0.182 | 0.369 | 3.526 | 0.525 | |||||||||||||||||||||||||||
Tab.3 Comparison of clinical features between the survival group and the death group of patients with left main complete occlusion
| 组别 | n | 年龄/岁 | 男性 | 高血压 | 糖尿病 | 吸烟史 | eGFR/ [mL/(min·1.73 m2)] | LDL-C/ (mmol/L) | 休克 | 发病 时间/h | 侧支 循环 | IABP 植入 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 存活组 | 50 | 58.9±13.9 | 43(86.0) | 2(54.0) | 13(26.0) | 38(76.0) | 58.8±22.3 | 3.36±0.84 | 20(40.0) | 3.7±2.1 | 29(58.0) | 46(92.0) | ||||||||||||||||||||
| 死亡组 | 44 | 62.9±11.8 | 37(84.1) | 28(63.6) | 16(36.4) | 35(79.5) | 52.0±18.7 | 3.18±0.90 | 41(93.2) | 4.3±3.3 | 9(20.5) | 42(95.5) | ||||||||||||||||||||
| t或χ2 | 1.513 | 0.067 | 0.895 | 1.178 | 0.170 | 1.587 | 1.067 | 29.056** | 0.937 | 14.756** | 0.467 | |||||||||||||||||||||
| 组别 | 机械 通气 | 血栓 抽吸 | 右冠状动脉 严重狭窄 | 右冠状动脉同期PCI | 左主干病变部位 | avR导联(包括avR+ V1导联)ST段抬高 | Ⅰ、avL、V2—V5 导联ST段抬高 | avR+avL导 联ST段抬高 | ||||||||||||||||||||||||
| 开口 | 左主干体部 | 分叉 | ||||||||||||||||||||||||||||||
| 存活组 | 17(34.0) | 14(28.0) | 13(26.0) | 3(6.0) | 0(0) | 31(62.0) | 19(38.0) | 14(28.0) | 17(34.0) | 19(38.0) | ||||||||||||||||||||||
| 死亡组 | 23(52.3) | 13(29.5) | 8(18.2) | 1(2.3) | 0(0) | 30(68.2) | 14(31.8) | 3(6.8) | 34(77.3) | 7(15.9) | ||||||||||||||||||||||
| χ2 | 3.197 | 0.027 | 0.825 | 0.798 | 0.393 | 7.088** | 17.658** | 5.708* | ||||||||||||||||||||||||
| 组别 | QRS时限/ms | 左前分支 传导阻滞 | 完全性右束支 传导阻滞 | 左前分支+右束支 传导阻滞 | 发病年度 | |||||||||||||||||||||||||||
| 2001—2006 | 2007—2012 | 2013—2018 | 2019—2023 | |||||||||||||||||||||||||||||
| 存活组 | 111±23 | 18(36.0) | 2(4.0) | 6(12.0) | 10(20.0) | 11(22.0) | 15(30.0) | 14(28.0) | ||||||||||||||||||||||||
| 死亡组 | 122±23 | 14(31.8) | 3(6.8) | 12(27.3) | 9(20.5) | 12(27.3) | 13(29.5) | 10(22.7) | ||||||||||||||||||||||||
| t或χ2 | 2.280* | 0.182 | 0.369 | 3.526 | 0.525 | |||||||||||||||||||||||||||
| 组别 | n | 年龄/岁 | 男性 | 高血压 | 糖尿病 | 吸烟史 | eGFR/[mL/(min·1.73 m2)] | LDL-C/(mmol/L) | 休克 | 发病时间/h | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 存活组 | 85 | 63.9±10.0 | 65(76.5) | 46(54.1) | 23(27.1) | 61(71.8) | 56.7±20.9 | 3.31±0.78 | 6(7.1) | 4.1±2.7 | ||||||||||||||||||||
| 死亡组 | 14 | 68.4±7.9 | 12(85.7) | 9(64.3) | 4(28.6) | 10(71.4) | 56.9±18.1 | 2.94±0.80 | 11(78.6) | 5.0±3.6 | ||||||||||||||||||||
| χ2或t | 1.601 | 0.594 | 0.503 | 0.014 | 0.001 | 0.027 | 1.654 | 43.220** | 1.110 | |||||||||||||||||||||
| 组别 | 侧支循环 | IABP植入 | 机械通气 | 血栓抽吸 | 左主干病变部位 | avR导联(包括avR+ V1)ST段抬高 | Ⅰ、avL、V2—V5 导联ST段抬高 | |||||||||||||||||||||||
| 开口 | 左主干体部 | 分叉 | ||||||||||||||||||||||||||||
| 存活组 | 0(0) | 59(69.4) | 13(15.3) | 10(11.8) | 7(8.2) | 37(43.5) | 41(48.2) | 77(90.6) | 5(5.9) | |||||||||||||||||||||
| 死亡组 | 0(0) | 12(85.7) | 6(42.9) | 3(21.4) | 3(21.4) | 4(28.6) | 7(50.0) | 12(85.7) | 2(14.3) | |||||||||||||||||||||
| χ2或t | 1.575 | 5.888* | 0.984 | 2.728 | 0.314 | 1.292 | ||||||||||||||||||||||||
| 组别 | avR+avL导联ST段抬高 | QRS时限/ms | 左前分支 传导阻滞 | 完全性右束支传导阻滞 | 左前分支+右束支传导阻滞 | 发病年度 | ||||||||||||||||||||||||
| 2001—2006 | 2007—2012 | 2013—2018 | 2019—2023 | |||||||||||||||||||||||||||
| 存活组 | 3(3.5) | 93±13 | 10(11.8) | 0(0) | 0(0) | 10(11.8) | 26(30.6) | 29(34.1) | 20(23.5) | |||||||||||||||||||||
| 死亡组 | 0(0) | 100±14 | 3(21.4) | 1(7.1) | 0(0) | 2(14.3) | 4(28.6) | 5(35.7) | 3(21.4) | |||||||||||||||||||||
| χ2或t | 0.510 | 1.867 | 0.984 | 6.133* | 0.111 | |||||||||||||||||||||||||
Tab.4 Comparison of clinical features between the survival group and the death group of patients with left main subtotal occlusion
| 组别 | n | 年龄/岁 | 男性 | 高血压 | 糖尿病 | 吸烟史 | eGFR/[mL/(min·1.73 m2)] | LDL-C/(mmol/L) | 休克 | 发病时间/h | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 存活组 | 85 | 63.9±10.0 | 65(76.5) | 46(54.1) | 23(27.1) | 61(71.8) | 56.7±20.9 | 3.31±0.78 | 6(7.1) | 4.1±2.7 | ||||||||||||||||||||
| 死亡组 | 14 | 68.4±7.9 | 12(85.7) | 9(64.3) | 4(28.6) | 10(71.4) | 56.9±18.1 | 2.94±0.80 | 11(78.6) | 5.0±3.6 | ||||||||||||||||||||
| χ2或t | 1.601 | 0.594 | 0.503 | 0.014 | 0.001 | 0.027 | 1.654 | 43.220** | 1.110 | |||||||||||||||||||||
| 组别 | 侧支循环 | IABP植入 | 机械通气 | 血栓抽吸 | 左主干病变部位 | avR导联(包括avR+ V1)ST段抬高 | Ⅰ、avL、V2—V5 导联ST段抬高 | |||||||||||||||||||||||
| 开口 | 左主干体部 | 分叉 | ||||||||||||||||||||||||||||
| 存活组 | 0(0) | 59(69.4) | 13(15.3) | 10(11.8) | 7(8.2) | 37(43.5) | 41(48.2) | 77(90.6) | 5(5.9) | |||||||||||||||||||||
| 死亡组 | 0(0) | 12(85.7) | 6(42.9) | 3(21.4) | 3(21.4) | 4(28.6) | 7(50.0) | 12(85.7) | 2(14.3) | |||||||||||||||||||||
| χ2或t | 1.575 | 5.888* | 0.984 | 2.728 | 0.314 | 1.292 | ||||||||||||||||||||||||
| 组别 | avR+avL导联ST段抬高 | QRS时限/ms | 左前分支 传导阻滞 | 完全性右束支传导阻滞 | 左前分支+右束支传导阻滞 | 发病年度 | ||||||||||||||||||||||||
| 2001—2006 | 2007—2012 | 2013—2018 | 2019—2023 | |||||||||||||||||||||||||||
| 存活组 | 3(3.5) | 93±13 | 10(11.8) | 0(0) | 0(0) | 10(11.8) | 26(30.6) | 29(34.1) | 20(23.5) | |||||||||||||||||||||
| 死亡组 | 0(0) | 100±14 | 3(21.4) | 1(7.1) | 0(0) | 2(14.3) | 4(28.6) | 5(35.7) | 3(21.4) | |||||||||||||||||||||
| χ2或t | 0.510 | 1.867 | 0.984 | 6.133* | 0.111 | |||||||||||||||||||||||||
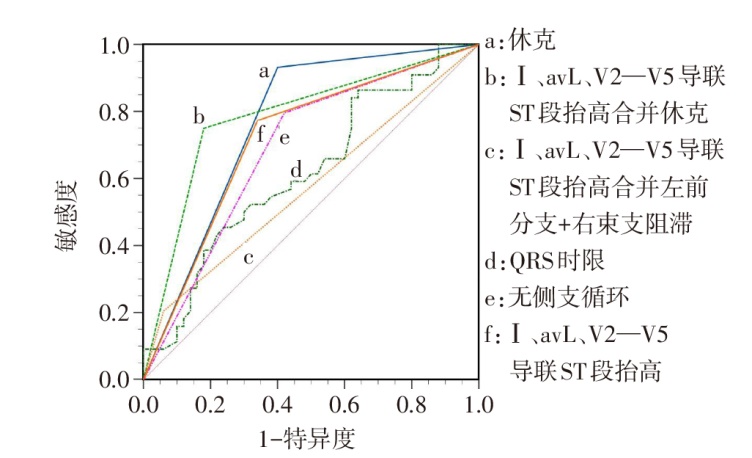
Fig.1 ROC curve of ECG index for predicting hospital death with left main complete occlusion
| 指标 | AUC(95% CI) | SE | 敏感度 | 特异度 |
|---|---|---|---|---|
| 休克 | 0.766(0.667~0.847) | 0.040 | 0.93 | 0.60 |
| Ⅰ、avL、V2—V5导联ST段抬高合并休克 | 0.785(0.688~0.863) | 0.043 | 0.75 | 0.82 |
| Ⅰ、avL、V2—V5导联ST段抬高合并左前分支+右束支阻滞 | 0.572(0.466~0.674) | 0.035 | 0.21 | 0.94 |
| QRS时限 | 0.619(0.513~0.717) | 0.059 | 0.86 | 0.36 |
| 无侧支循环 | 0.688(0.584~0.779) | 0.047 | 0.80 | 0.58 |
| Ⅰ、avL、V2—V5导联ST段抬高 | 0.716(0.614~0.805) | 0.047 | 0.77 | 0.66 |
Tab.5 Value of electrocardiogram characteristics in predicting hospital death with complete occlusion of left main trunk
| 指标 | AUC(95% CI) | SE | 敏感度 | 特异度 |
|---|---|---|---|---|
| 休克 | 0.766(0.667~0.847) | 0.040 | 0.93 | 0.60 |
| Ⅰ、avL、V2—V5导联ST段抬高合并休克 | 0.785(0.688~0.863) | 0.043 | 0.75 | 0.82 |
| Ⅰ、avL、V2—V5导联ST段抬高合并左前分支+右束支阻滞 | 0.572(0.466~0.674) | 0.035 | 0.21 | 0.94 |
| QRS时限 | 0.619(0.513~0.717) | 0.059 | 0.86 | 0.36 |
| 无侧支循环 | 0.688(0.584~0.779) | 0.047 | 0.80 | 0.58 |
| Ⅰ、avL、V2—V5导联ST段抬高 | 0.716(0.614~0.805) | 0.047 | 0.77 | 0.66 |
| 不同心电图特点 | n | 前降支供血区 | 前降支+回旋支供血区 | 回旋支供血区 | 无侧支循环 |
|---|---|---|---|---|---|
| avR导联(包含avR+V1导联)ST段抬高 | 17 | 1(5.9) | 14(82.4) | 0(0) | 2(11.8) |
| avR+avL导联ST段抬高 | 26 | 18(69.2) | 4(15.4) | 1(3.8) | 3(11.5) |
| Ⅰ、avL、V2—V5导联ST段抬高 | 51 | 0(0) | 0(0) | 0(0) | 51(100.0) |
| χ2 | 53.822** | 56.181** | 2.644 | 75.653** |
Tab.6 Comparison of collateral circulation blood supply areas between different ECG characteristics in left main complete occlusion
| 不同心电图特点 | n | 前降支供血区 | 前降支+回旋支供血区 | 回旋支供血区 | 无侧支循环 |
|---|---|---|---|---|---|
| avR导联(包含avR+V1导联)ST段抬高 | 17 | 1(5.9) | 14(82.4) | 0(0) | 2(11.8) |
| avR+avL导联ST段抬高 | 26 | 18(69.2) | 4(15.4) | 1(3.8) | 3(11.5) |
| Ⅰ、avL、V2—V5导联ST段抬高 | 51 | 0(0) | 0(0) | 0(0) | 51(100.0) |
| χ2 | 53.822** | 56.181** | 2.644 | 75.653** |
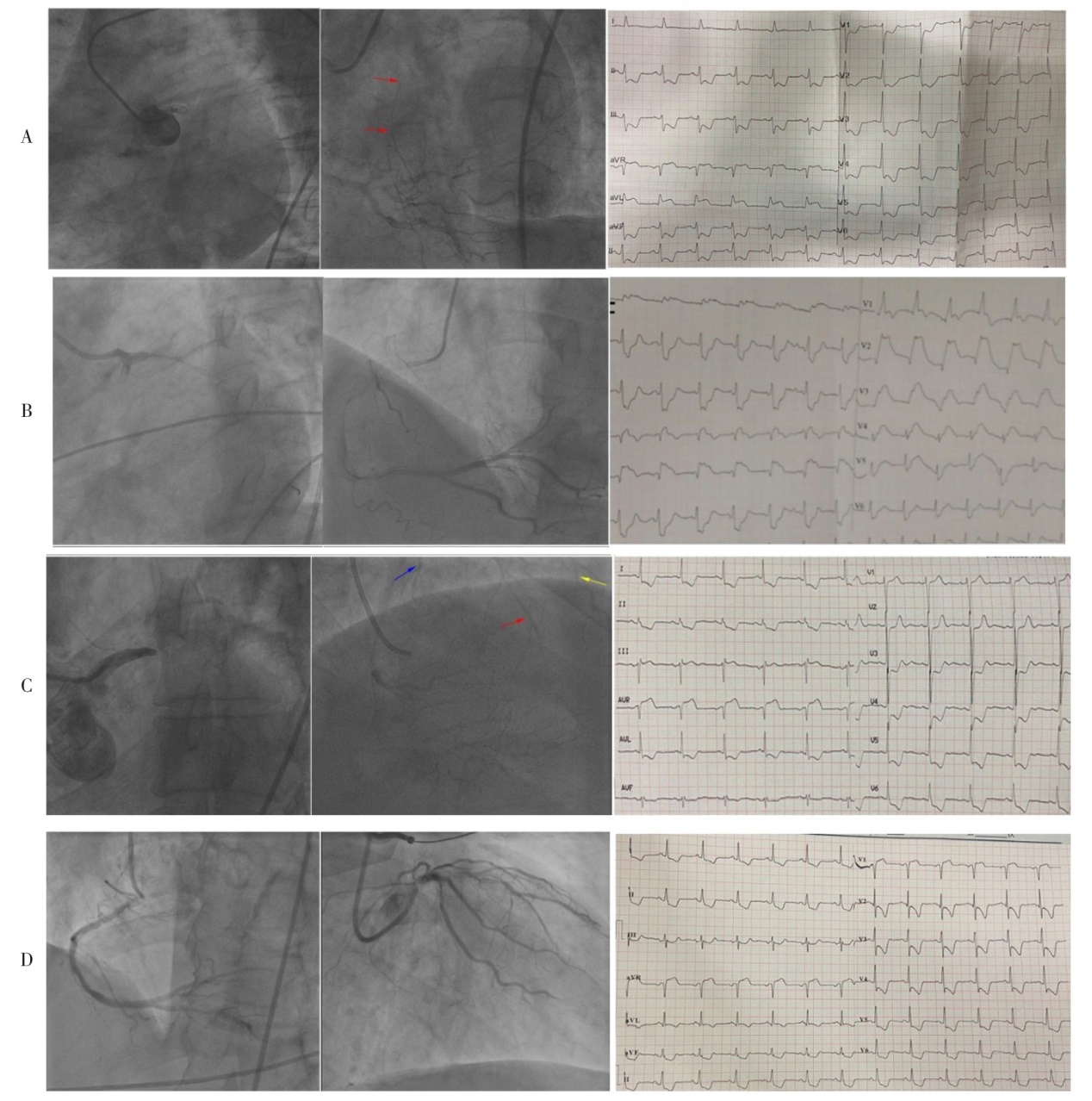
Fig.2 Corresponding collateral circulation in patients with different ECG manifestations in left main disease
| [1] | 何金山, 李学斌, 郭继鸿. 左主干闭塞的心电图表现[J]. 中华心血管病杂志, 2019, 47(9):756-758. |
| HE J S, LI X B, GUO J H. Electrocardiogram characteristics of patients with left main coronary artery occlusion[J]. Chinese Journal of Cardiology, 2019, 47(9):756-758. doi:16806/j.cnki.issn.1004-3934.2021.09.009. | |
| [2] | AHMED A, AGUIRRE F V, CHAMBERS J, et al. STEMI:considerations for left main culprit lesions[J]. Curr Cardiol Rep, 2022, 24(6):645-651. doi:10.1007/s11886-022-01685-6. |
| [3] | NIKUS K C. Electrocardiographic presentations of acute total occlusion of the left main coronary artery[J]. J Electrocardiol, 2012, 45(5):491-493. doi:10.1016/j.jelectrocard.2012.06.014. |
| [4] | THYGESEN K, ALPERT J S, JAFFE A S, et al. Fourth universal definition of myocardial infarction(2018)[J]. Eur Heart J, 2019, 40(3):237-269. doi:10.1093/eurheartj/ehy462. |
| [5] | 夏平. “8+2”心电图临床价值的研究进展[J]. 心血管病学进展, 2021, 42(9):800-803,808. |
| XIA P. Clinical value of"8 Plus 2"ECG[J]. Advances in Cardiovascular Diseases, 2021, 42(9):800-803,808. doi:10.16806/j.cnki.issn.1004-3934.2021.09.009. | |
| [6] | D'ANGELO C, ZAGNONI S, GALLO P, et al. Electrocardiographic changes in patients with acute myocardial infarction caused by left main trunk occlusion[J]. J Cardiovasc Med(Hagerstown), 2018, 19(8):439-445. doi:10.2459/JCM.0000000000000684. |
| [7] | YAMAJI H, IWASAKI K, KUSACHI S, et al. Prediction of acute left main coronary artery obstruction by 12-lead electrocardiography. ST segment elevation in lead aVR with less ST segment elevation in lead V(1)[J]. J Am Coll Cardiol, 2001, 38(5):1348-1354. doi:10.1016/s0735-1097(01)01563-7. |
| [8] | NIKUS K C, SCLAROVSKY S, HUHTALA H, et al. Electrocardiographic presentation of global ischemia in acute coronary syndrome predicts poor outcome[J]. Ann Med, 2012, 44(5):494-502. doi:10.3109/07853890.2011.585345. |
| [9] | WONG C K, GAO W, STEWART R A, et al. aVR ST elevation: an important but neglected sign in ST elevation acute myocardial infarction[J]. Eur Heart J, 2010, 31(15):1845-1853. doi:10.1093/eurheartj/ehq161. |
| [10] | GUTIÉRREZ-BARRIOS A, MIALDEA-SALMERÓN D, CAÑADAS-PRUAÑO D, et al. Electrocardiographic findings in true acute left main coronary total occlusion a subanalisys from ATOLMA registry[J]. J Electrocardiol, 2021, 68:48-52. doi:10.1016/j.jelectrocard.2021.07.017. |
| [11] | KURISU S, INOUE I, KAWAGOE T, et al. Electrocardiographic features in patients with acute myocardial infarction associated with left main coronary artery occlusion[J]. Heart, 2004, 90(9):1059-1060. doi:10.1136/hrt.2003.026799. |
| [12] | BIRNBAUM Y, HASDAI D, SCLAROVSKY S, et al. Acute myocardial infarction entailing ST-segment elevation in lead aVL:electrocardiographic differentiation among occlusion of the left anterior descending, first diagonal, and first obtuse marginal coronary arteries[J]. Am Heart J, 1996, 131(1):38-42. doi:10.1016/s0002-8703(96)90048-4. |
| [13] | IIDA T, TANIMURA F, TAKAHASHI K, et al. Electrocardiographic characteristics associated with in-hospital outcome in patients with left main acute coronary syndrome:for contriving a new risk stratification score[J]. Eur Heart J Acute Cardiovasc Care, 2018, 7(3):200-207. doi:10.1177/2048872616683524. |
| [14] | FIOL M, CARRILLO A, RODRíGUEZ A, et al. Electrocardiographic changes of ST-elevation myocardial infarction in patients with complete occlusion of the left main trunk without collateral circulation: differential diagnosis and clinical considerations[J]. J Electrocardiol, 2012, 45(5):487-490. doi:10.1016/j.jelectrocard.2012.05.001. |
| [15] | LIU C, YANG F, HU Y, et al. Combining electrocardiographic criteria for predicting acute total left main coronary artery occlusion[J]. Front Cardiovasc Med, 2022,9:936687. doi:10.3389/fcvm.2022.936687. |
| [16] | GONZÁLEZ-BRAVO D H, ESCABÍ-MENDOZA J. Electrocardiographic recognition of unprotected left main ST-segment elevation myocardial infarction:looking beyond aVR[J]. JACC Case Rep, 2021, 3(5):754-759. doi:10.1016/j.jaccas.2021.02.014. |
| [17] | HIRANO T, TSUCHIYA K, NISHIGAKI K, et al. Clinical features of emergency electrocardiography in patients with acute myocardial infarction caused by left main trunk obstruction[J]. Circ J, 2006, 70(5):525-529. doi:10.1253/circj.70.525. |
| [18] | WIDIMSKY P, ROHAC F, STASEK J, et al. Primary angioplasty in acute myocardial infarction with right bundle branch block:should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy?[J]. Eur Heart J, 2012, 33(1):86-95. doi:10.1093/eurheartj/ehr291. |
| [19] | VIS M M, BEIJK M A, GRUNDEKEN M J, et al. A systematic review and meta-analysis on primary percutaneous coronary intervention of an unprotected left main coronary artery culprit lesion in the setting of acute myocardial infarction[J]. JACC Cardiovasc Interv, 2013, 6(4):317-324. doi:10.1016/j.jcin.2012.10.020. |
| [20] | ZHOU H, HUANG Y S, ZHAO Y T, et al. Clinical and electrocardiographic features in acute total left main coronary artery occlusion without collateral circulation[J]. J Electrocardiol, 2023, 76:79-84. doi:10.1016/j.jelectrocard.2022.11.005. |
| [1] | YU Youjia, QIN Xia. Prognostic value of peripheral perfusion index combined with plasma volume in patients with septic shock [J]. Tianjin Medical Journal, 2026, 54(2): 169-172. |
| [2] | CAO Zhenzhen, YE Rui, LIU Jiayao, MENG Tong, SUN Rong, XU Lingyao. Application value of serum Hsp90α combined with β2-MG detection in early diagnosis and prognosis of colorectal cancer [J]. Tianjin Medical Journal, 2025, 53(7): 756-760. |
| [3] | XIANG Lili, WANG Qian, MENG Yanna, FU Jie, ZHANG Pu. Efficacy of lenalidomide combined with bortezomib and dexamethasone in the treatment of multiple myeloma [J]. Tianjin Medical Journal, 2025, 53(6): 665-669. |
| [4] | HAO Yanyan, ZHANG Yu, BAI Yaowu, SHI Donghai. Effects of remimazolam regulating the Nrf2/GPX4 pathway on circulatory function in septic shock rats [J]. Tianjin Medical Journal, 2025, 53(4): 349-354. |
| [5] | ZHANG Yehang, NIU Xiangdong, GENG Yiming. Diagnostic value of serum sST2 and DcR3 combined with dynamic electrocardiogram in silent myocardial ischemia [J]. Tianjin Medical Journal, 2025, 53(4): 420-424. |
| [6] | LIU Huan, ZHANG Qi, YAN Qikun, CAO Lu. A single-center study of the relationship between QRS duration of first medical contact and clinical endpoint in acute ST-segment elevation myocardial infarction [J]. Tianjin Medical Journal, 2025, 53(1): 71-74. |
| [7] | DAI Yao, FANG Xiang, HUANG Kang, FENG Jie, LIU Min, WU Songbai. Clinical curative effect of HAT therapy on septic shock [J]. Tianjin Medical Journal, 2024, 52(8): 825-829. |
| [8] | REN Yan, CHEN Shanping, ZHOU Lihua, WANG Lingxiao, GUAN Lijuan, YANG Yongxue. The predictive value of laboratory frailty index for the risk of sepsis and septic shock in elderly CAP inpatients [J]. Tianjin Medical Journal, 2024, 52(4): 416-421. |
| [9] | YU Hong, YANG Chaodong, LIU dan. The relationship between ALT/ALP ratio, PLR and hepatic injury in elderly patients with septic shock [J]. Tianjin Medical Journal, 2024, 52(11): 1211-1215. |
| [10] | LU Yibei, JIN Dongxia, SONG Zhenchun, MA Haoyuan, LI Yan, HAO Tianxu, LI Ximing. Preliminary research on clinical application of a new flexible patch ECG [J]. Tianjin Medical Journal, 2024, 52(10): 1095-1099. |
| [11] | HU Danhui, LUO Huichen, LIU Haiying. The expression of miR-149-3p in heart tissue of newborn mice with congenital heart disease and its effect on differentiation of P19 cells [J]. Tianjin Medical Journal, 2023, 51(1): 45-49. |
| [12] | CHANG Qinghua, WANG Gaopin, LIU Renguang. The study of His bundle potential recorded beat by beat on body surface [J]. Tianjin Medical Journal, 2022, 50(4): 424-427. |
| [13] | GU Zi, TANG Yong, ZHOU Chengji, ZHENG Qiang. The role of palmitoylated NOD2 in animal model of hemorrhagic shock [J]. Tianjin Medical Journal, 2022, 50(10): 1050-1055. |
| [14] | LI Qing, LIU Xuan-chang, ZHU Fen, CAO Lei, JIANG Wen, LI Xiang-you△. Relationship between cardiac electrical remodeling and blood pressure control in patients with primary hypertension [J]. Tianjin Medical Journal, 2021, 49(9): 968-972. |
| [15] | WANG Qing-feng, WANG Xin-kang. Relationship between chest wall deformity with congenital pectus excavatum and abnormal electrocardiogram in children [J]. Tianjin Medical Journal, 2021, 49(8): 856-860. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||