Tianjin Medical Journal ›› 2026, Vol. 54 ›› Issue (4): 369-373.doi: 10.11958/20251913
• Clinical Research • Previous Articles Next Articles
YAO Guohua1( ), LIU Jie1, ZHANG Wen1, MA Cuian1△(), WEI Botao1, GAO Na2
), LIU Jie1, ZHANG Wen1, MA Cuian1△(), WEI Botao1, GAO Na2
Received:2025-05-09
Revised:2025-11-21
Published:2026-04-15
Online:2026-04-14
Contact:
△E-mail:YAO Guohua, LIU Jie, ZHANG Wen, MA Cuian, WEI Botao, GAO Na. The construction of a prediction model for severe pneumonia caused by mycoplasma pneumoniae mixed with adenovirus infection in children based on BP neural network[J]. Tianjin Medical Journal, 2026, 54(4): 369-373.
CLC Number:
| 组别 | n | 男性 | 年龄/岁 | 出生体质量/kg | 发热持续天数/d | 最高体温/℃ | HGB/(g/L) | WBC/(×109/L) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非重症组 | 58 | 27(46.6) | 4.0(3.0,7.0) | 3.2(3.0,3.6) | 6.0(4.2,7.0) | 39.5(39.4,40.0) | 123(114.0,131.0) | 8.2(6.2,11.7) | |||||||||||||||||||
| 重症组 | 80 | 37(46.2) | 4.5(3.0,6.2) | 3.3(3.0,3.6) | 10.0(7.0,12.0) | 40.0(39.6,40.2) | 122(118.8,129.2) | 9.1(6.8,12.0) | |||||||||||||||||||
| U或χ2 | 0.000 | 2 328.500 | 2 223.500 | 1 034.500** | 1 568.500** | 2 334.000 | 2 095.500 | ||||||||||||||||||||
| 组别 | N/% | L/% | M/% | PLT/(×109/L) | CRP/(mg/L) | 白蛋白/(g/L) | ALT/(U/L) | ||||||||||||||||||||
| 非重症组 | 55.6(38.2,66.3) | 34.0(23.5,45.9) | 8.0(6.1,10.8) | 269(238.0,329.5) | 11.2(3.1,23.2) | 42.8(41.2,45.5) | 11.5(10.0,15.0) | ||||||||||||||||||||
| 重症组 | 64.5(56.9,74.2) | 24.2(19.5,32.4) | 7.2(5.0,9.2) | 271(217.8,356.0) | 14.2(3.3,33.1) | 41.4(39.4,43.4) | 12.0(10.0,16.0) | ||||||||||||||||||||
| U或χ2 | 1 540.000** | 2 960.000** | 2 762.000 | 2 326.500 | 2 033.000 | 2 994.000** | 2 135.000 | ||||||||||||||||||||
| 组别 | γ-GT/(U/L) | PCT/(μg/L) | AST/(U/L) | BUN/(mmol/L) | Cre/(μmol/L) | CK/(U/L) | CK-MB/(U/L) | ||||||||||||||||||||
| 非重症组 | 10.0(8.0,13.0) | 0.1(0.1,0.5) | 30.5(25.0,39.0) | 2.7(2.3,3.5) | 28.0(25.0,33.0) | 81.5(58.8,108.8) | 2.0(0.2,5.8) | ||||||||||||||||||||
| 重症组 | 10.5(8.0,13.0) | 0.2(0.1,0.5) | 35.0(27.8,46.2) | 2.9(2.5,3.4) | 29.0(24.0,33.0) | 83.0(62.2,132.0) | 2.5(0.0,5.2) | ||||||||||||||||||||
| U或χ2 | 2 123.500 | 2 047.500 | 1 755.500* | 2 129.500 | 2 320.500 | 2 209.500 | 2 439.500 | ||||||||||||||||||||
| 组别 | LDH/(U/L) | La/(mmol/L) | IL-6/(ng/L) | 大片炎症实变 | 住院天数/d | ||||||||||||||||||||||
| 非重症组 | 344.5(293.2,444.5) | 2.6(2.2,3.5) | 18.3(8.9,29.7) | 27(46.6) | 4.0(4.0,6.0) | ||||||||||||||||||||||
| 重症组 | 439.5(315.8,575.5) | 2.6(2.2,3.3) | 33.7(17.8,53.6) | 57(71.2) | 8.0(6.0,10.2) | ||||||||||||||||||||||
| U或χ2 | 1 628.000** | 2 430.500 | 1 453.000** | 7.610** | 481.500** | ||||||||||||||||||||||
Tab.1 Comparison of clinical data between the two groups of children
| 组别 | n | 男性 | 年龄/岁 | 出生体质量/kg | 发热持续天数/d | 最高体温/℃ | HGB/(g/L) | WBC/(×109/L) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非重症组 | 58 | 27(46.6) | 4.0(3.0,7.0) | 3.2(3.0,3.6) | 6.0(4.2,7.0) | 39.5(39.4,40.0) | 123(114.0,131.0) | 8.2(6.2,11.7) | |||||||||||||||||||
| 重症组 | 80 | 37(46.2) | 4.5(3.0,6.2) | 3.3(3.0,3.6) | 10.0(7.0,12.0) | 40.0(39.6,40.2) | 122(118.8,129.2) | 9.1(6.8,12.0) | |||||||||||||||||||
| U或χ2 | 0.000 | 2 328.500 | 2 223.500 | 1 034.500** | 1 568.500** | 2 334.000 | 2 095.500 | ||||||||||||||||||||
| 组别 | N/% | L/% | M/% | PLT/(×109/L) | CRP/(mg/L) | 白蛋白/(g/L) | ALT/(U/L) | ||||||||||||||||||||
| 非重症组 | 55.6(38.2,66.3) | 34.0(23.5,45.9) | 8.0(6.1,10.8) | 269(238.0,329.5) | 11.2(3.1,23.2) | 42.8(41.2,45.5) | 11.5(10.0,15.0) | ||||||||||||||||||||
| 重症组 | 64.5(56.9,74.2) | 24.2(19.5,32.4) | 7.2(5.0,9.2) | 271(217.8,356.0) | 14.2(3.3,33.1) | 41.4(39.4,43.4) | 12.0(10.0,16.0) | ||||||||||||||||||||
| U或χ2 | 1 540.000** | 2 960.000** | 2 762.000 | 2 326.500 | 2 033.000 | 2 994.000** | 2 135.000 | ||||||||||||||||||||
| 组别 | γ-GT/(U/L) | PCT/(μg/L) | AST/(U/L) | BUN/(mmol/L) | Cre/(μmol/L) | CK/(U/L) | CK-MB/(U/L) | ||||||||||||||||||||
| 非重症组 | 10.0(8.0,13.0) | 0.1(0.1,0.5) | 30.5(25.0,39.0) | 2.7(2.3,3.5) | 28.0(25.0,33.0) | 81.5(58.8,108.8) | 2.0(0.2,5.8) | ||||||||||||||||||||
| 重症组 | 10.5(8.0,13.0) | 0.2(0.1,0.5) | 35.0(27.8,46.2) | 2.9(2.5,3.4) | 29.0(24.0,33.0) | 83.0(62.2,132.0) | 2.5(0.0,5.2) | ||||||||||||||||||||
| U或χ2 | 2 123.500 | 2 047.500 | 1 755.500* | 2 129.500 | 2 320.500 | 2 209.500 | 2 439.500 | ||||||||||||||||||||
| 组别 | LDH/(U/L) | La/(mmol/L) | IL-6/(ng/L) | 大片炎症实变 | 住院天数/d | ||||||||||||||||||||||
| 非重症组 | 344.5(293.2,444.5) | 2.6(2.2,3.5) | 18.3(8.9,29.7) | 27(46.6) | 4.0(4.0,6.0) | ||||||||||||||||||||||
| 重症组 | 439.5(315.8,575.5) | 2.6(2.2,3.3) | 33.7(17.8,53.6) | 57(71.2) | 8.0(6.0,10.2) | ||||||||||||||||||||||
| U或χ2 | 1 628.000** | 2 430.500 | 1 453.000** | 7.610** | 481.500** | ||||||||||||||||||||||
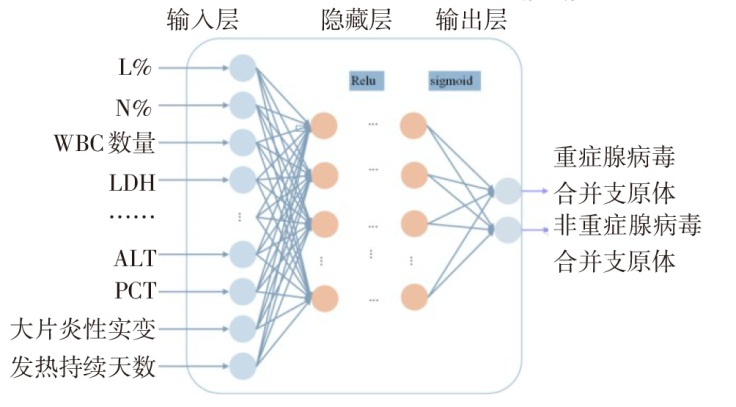
Fig.1 Structural diagram of the prediction model for severe pneumonia in children with MP mixed ADV established by BP neural network
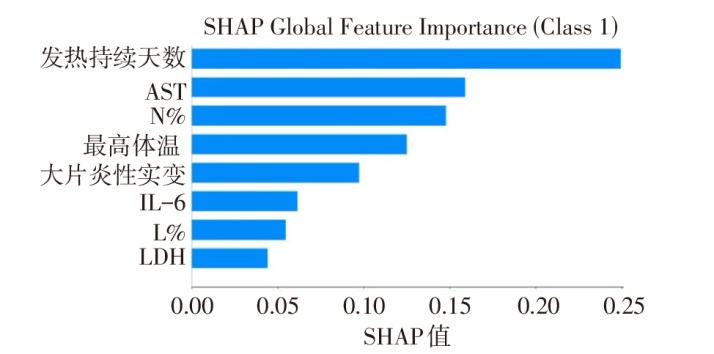
Fig.2 Bar chart of SHAP values for key predictors
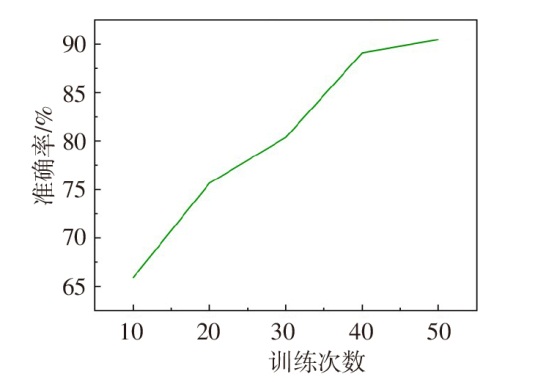
Fig.3 Accuracy change curve
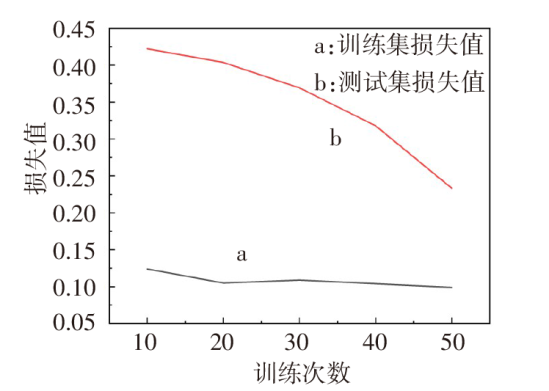
Fig.4 Loss change curve
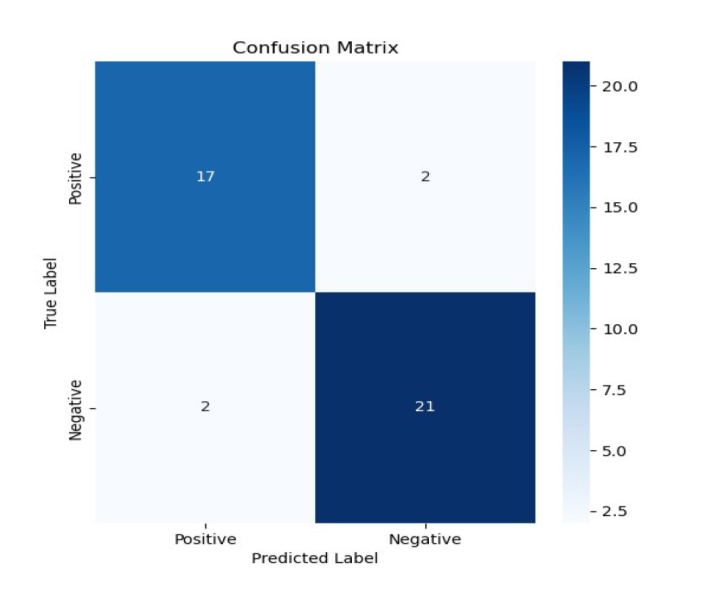
Fig.5 Confusion matrix
| [1] | PERIN J, MULICK A, YEUNG D, et al. Global,regional,and national causes of under-5 mortality in 2000-19:an updated systematic analysis with implications for the Sustainable Development Goals[J]. Lancet Child Adolesc Health, 2022, 6(2):106-115. doi:10.1016/S2352-4642(21)00311-4. |
| [2] | NAIR G B, NIEDERMAN M S. Updates on community acquired pneumonia management in the ICU[J]. Pharmacol Ther, 2021, 217:107663. doi:10.1016/j.pharmthera.2020.107663. |
| [3] | CHEN B, GAO L Y, CHU Q J, et al. The epidemic characteristics of Mycoplasma pneumoniae infection among children in Anhui,China,2015-2023[J]. Microbiol Spectr, 2024, 12(10):e0065124. doi:10.1128/spectrum.00651-24. |
| [4] | LIU M, XU Q, LI T, et al. Prevalence of human infection with respiratory adenovirus in China:A systematic review and meta-analysis[J]. PLoS Negl Trop Dis, 2023, 17(2):e0011151. doi:10.1371/journal.pntd.0011151. |
| [5] | 黄娇甜, 卢秀兰, 祝益民, 等. 儿童重症腺病毒肺炎的临床特征及混合感染的高危因素分析[J]. 中国小儿急救医学, 2021, 28(9):756-762. |
| HUANG J T, LU X L, ZHU Y M, et al. Risk factors for mixed infections and clinical characteristics in children with severe adenovirus pneumonia[J]. Chinese Pediatric Emergency Medicine, 2021, 28(9):756-762. doi:10.3760/cma.j.issn.1673-4912.2021.09.003. | |
| [6] | LI F, ZHANG Y, SHI P, et al. Mycoplasma pneumoniae and adenovirus coinfection cause pediatric severe community-acquired pneumonia[J]. Microbiol Spectr, 2022, 10(2):e0002622. doi:10.1128/spectrum.00026-22. |
| [7] | NAJAFABADI A H Z, RAMSPEK C L, DEKKER F W, et al. TRIPOD statement:a preliminary pre-post analysis of reporting and methods of prediction models[J]. BMJ Open, 2020, 10(9):e041537. doi:10.1136/bmjopen-2020-041537. |
| [8] | ZHOU Y, WANG J, CHEN W, et al. Impact of viral coinfection and macrolide-resistant mycoplasma infection in children with refractory Mycoplasma pneumoniae pneumonia[J]. BMC Infect Dis, 2020, 20(1):633. doi:10.1186/s12879-020-05356-1. |
| [9] | 中华人民共和国国家卫生健康委员会国家中医药管理局. 儿童腺病毒肺炎诊疗规范(2019年版)[J]. 中华临床感染病杂志, 2019, 12(3):161-166. |
| National Health Commission of the People's Republic of China,State Administration of Traditional Chinese Medicine. Guideline for diagnosis and treatment of adenovirus pneumonia in children (2019 version)[J]. Chinese Journal of Clinical Infectious Diseases, 2019, 12(3):161-166. doi:10.3760/cma.j.issn.1674-2397.2019.03.001. | |
| [10] | 中华人民共和国国家卫生健康委员会. 儿童肺炎支原体肺炎诊疗指南(2023年版)[J]. 国际流行病学传染病学杂志, 2023, 50(2):79-85. |
| National Health Commission of the People's Republic of China. Guidelines for the diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children(2023 edition)[J]. International Journal of Epidemiology and Infectious Disease, 2023, 50(2):79-85. doi:10.3760/cma.j.cn331340-20230217-00023. | |
| [11] | 中华人民共和国国家健康委员会, 国家中医药局, 儿童社区获得性肺炎诊疗规范(2019年版)[J]. 中华临床感染病杂志, 2019, 12(1):6-13. |
| National Health Commission of the People's Republic of China,National Administration of Traditional Chinese Medicine. Guideline for diagnosis and treatment of community-acquired pneumonia in Children (2019 version)[J]. Chinese Journal of Clinical Infectious Diseases, 2019, 12(1):6-13. doi:10.3760/cma.j.issn.1674-2397.2019.01.002. | |
| [12] | LÓPEZ-MARTÍNEZ F, NÚÑEZ-VALDEZ E R, CRESPO R G, et al. An artificial neural network approach for predicting hypertension using NHANES data[J]. Sci Rep, 2020, 10(1):10620. doi:10.1038/s41598-020-67640-z. |
| [13] | LUNDBERG S M, LEE S I. A unified approach to interpreting model predictions[C]. Advances in neural information processing systems, 2017,30. doi:10.48550/arXiv.1705.07874. |
| [14] | GAO J, XU L, XU B, et al. Human adenovirus coinfection aggravates the severity of Mycoplasma pneumoniae pneumonia in children[J]. BMC Infect Dis, 2020, 20(1):420. doi:10.1186/s12879-020-05152-x. |
| [15] | YI X, JIA W, LI W, et al. Diagnostic value of cytokines in severe childhood Mycoplasma pneumoniae pneumonia combined with Adenovirus infection[J]. Ital J Pediatr, 2024, 50(1):92. doi:10.1186/s13052-024-01661-6. |
| [16] | 史大伟, 刘玲, 赵萌萌, 等. 肺炎支原体肺炎患儿支气管肺泡灌洗液中肺炎支原体耐药基因和13种病原检测结果分析[J]. 中华实用儿科临床杂志, 2022, 37(12):893-896. |
| SHI D W, LIU L, ZHAO M M, et al. Analysis of drug resistance gene in Mycoplasma pneumoniae and 13 pathogens in bronchoalveolar lavage fluid of children with Mycoplasma pneumoniae pneumonia[J]. Chinese Journal of Applied Clinical Pediatrics, 2022, 37(12):893-896. doi:10.3760/cma.j.cn101070-20210716-00833. | |
| [17] | 王卫, 陈杰华, 谢淦, 等. 重症腺病毒肺炎后引起闭塞性细支气管炎的危险因素分析[J]. 中国小儿急救医学, 2022, 29(8):611-615. |
| WANG W, CHEN J H, XIE G, et al. Risk factors for postinfectious bronchiolitis obliterans after severe adenovirus pneumonia[J]. Chinese Pediatric Emergency Medicine, 2022, 29(8):611-615. doi:10.3760/cma.j.issn.1673-4912.2022.08.008. | |
| [18] | 冯志冠, 刘小兰, 陈杰华, 等. 重症肺炎相关性噬血细胞综合征30例临床分析[J]. 中华实用儿科临床杂志, 2021, 36(3):199-203. |
| FENG Z G, LIU X L, CHEN J H, et al. Clinical analysis of 30 cases of severe pneumonia-associated hemophagocytic lymphohistiocytosis[J]. Chinese Journal of Applied Clinical Pediatrics, 2021, 36(3):199-203. doi:10.3760/cma.j.cn101070-20191117-01142. | |
| [19] | ZHOU W, CHEN J, XI Z, et al. Characteristics of lung microbiota in children's refractory mycoplasma pneumoniae pneumonia coinfected with human adenovirus B[J]. Can J Infect Dis Med Microbiol, 2022, 2022:7065890. doi:10.1155/2022/7065890. |
| [20] | 李颖, 陈红卫, 胡若晖, 等. 儿童人腺病毒7型混合肺炎支原体感染肺炎36例临床特征分析[J]. 中华实用儿科临床杂志, 2022, 37(8):611-614. |
| LI Y, CHEN H W, HU R H, et al. Clinical analysis of 36 children with pneumonia caused by coinfection of human adenovirus type 7 and Mycoplasma pneumoniae[J]. Chinese Journal of Applied Clinical Pediatrics, 2022, 37(8):611-614. doi:10.3760/cma.j.cn101070-20210218-00191. | |
| [21] | 王玉亮, 王峰, 耿洁. 细胞因子与细胞因子风暴[J]. 天津医药, 2020, 48(6):494-499. |
| WANG Y L, WANG F, GENG J. Cytokine and cytokine storm[J]. Tianjin Med J, 2020, 48(6):494-499. doi:10.11958/20200323. | |
| [22] | 赖小雪, 邹映雪. 儿童腺病毒肺炎免疫学发病机制研究进展[J]. 国际儿科学杂志, 2022, 49(5):343-347. |
| LAI X X, ZOU Y X. Progress on immunological pathogenesis of adenovirus pneumonia in children[J]. International Journal of Pediatrics, 2022, 49(5):343-347. doi:10.3760/cma.j.issn.1673-4408.2022.05.013. | |
| [23] | HUANG J, YANG X, ZHUO Z, et al. Clinical characteristics of plastic bronchitis in children:a retrospective analysis of 43 cases[J]. Respir Res, 2022, 23(1):51. doi:10.1186/s12931-022-01975-1. |
| [24] | 中华医学会儿科学分会呼吸学组, 中华儿科杂志编辑委员会, 中国医药教育协会儿科专业委员会. 儿童社区获得性肺炎管理指南(2024修订)[J]. 中华儿科杂志, 2024, 62(10):920-930. |
| The Subspecialty Group of Respiratory the Society of Pediatrics Chinese Medical Association,The Editorial Board Chinese Journal of Pediatrics,China Medicine Education Association Committee on Pediatrics. Guidelines for the management of community-acquired pneumonia in children (2024 revision)[J]. Chinese Journal of Pediatrics, 2024, 62(10):920-930. doi:10.3760/cma.j.cn112140-20240728-00523. | |
| [25] | WEI J, WU S, JIN X, et al. Association of Mycoplasma pneumoniae coinfection with adenovirus pneumonia severity in children[J]. Allergol Immunopathol (Madr), 2022, 50(1):31-36. doi:10.15586/aei.v50i1.476. |
| [26] | 刘满姣, 钱星星, 皮胜男, 等. 腺病毒合并肺炎支原体感染患儿临床特征分析[J]. 国际医药卫生导报, 2024, 30(24):4115-4119. |
| LIU M J, QIAN X X, PI S N, et al. Analysis of clinical characteristics in children infected with adenovirus and Mycoplasma pneumoniae[J]. International Medicine and Health Guidance News, 2024, 30(24):4115-4119. doi:10.3760/cma.j.issn.1007-1245.2024.24.011. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||