Tianjin Medical Journal ›› 2025, Vol. 53 ›› Issue (7): 751-755.doi: 10.11958/20250560
• Clinical Research • Previous Articles Next Articles
CHEN Ying1( ), GUO Changying1, ZHANG Jing1, LI Juan1, CHEN Fengyi2
), GUO Changying1, ZHANG Jing1, LI Juan1, CHEN Fengyi2
Received:2025-02-14
Revised:2025-04-21
Published:2025-07-15
Online:2025-07-21
CHEN Ying, GUO Changying, ZHANG Jing, LI Juan, CHEN Fengyi. The risk of right heart failure after heart transplantation based on preoperative pulmonary artery pressure assessment[J]. Tianjin Medical Journal, 2025, 53(7): 751-755.
CLC Number:
| 组别 | n | 性别(男/女) | 年龄/岁 | BMI/(kg/m2) | NYHA心功能分级(Ⅲ级/Ⅳ级) | 吸烟史 |
|---|---|---|---|---|---|---|
| 训练集 | 126 | 90/36 | 49.52±9.02 | 22.37±1.41 | 88/38 | 82(65.1) |
| 验证集 | 58 | 44/14 | 48.64±8.75 | 22.15±1.36 | 40/18 | 32(55.2) |
| χ2或t | 0.394 | 0.621 | 0.994 | 0.344 | 1.654 |
Tab.1 Comparison of basic data between training set and verification set
| 组别 | n | 性别(男/女) | 年龄/岁 | BMI/(kg/m2) | NYHA心功能分级(Ⅲ级/Ⅳ级) | 吸烟史 |
|---|---|---|---|---|---|---|
| 训练集 | 126 | 90/36 | 49.52±9.02 | 22.37±1.41 | 88/38 | 82(65.1) |
| 验证集 | 58 | 44/14 | 48.64±8.75 | 22.15±1.36 | 40/18 | 32(55.2) |
| χ2或t | 0.394 | 0.621 | 0.994 | 0.344 | 1.654 |
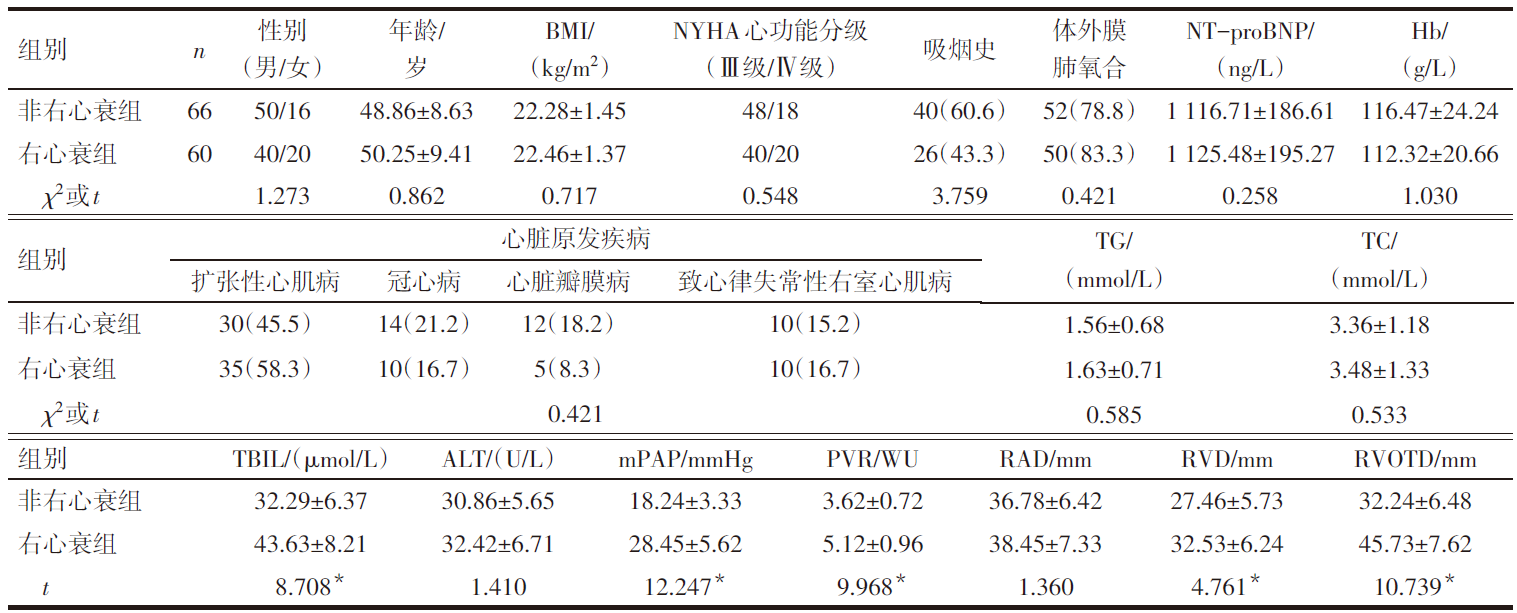 |
Tab.2 Comparison of clinical characteristics between the right heart failure group and the non-failure group
| |
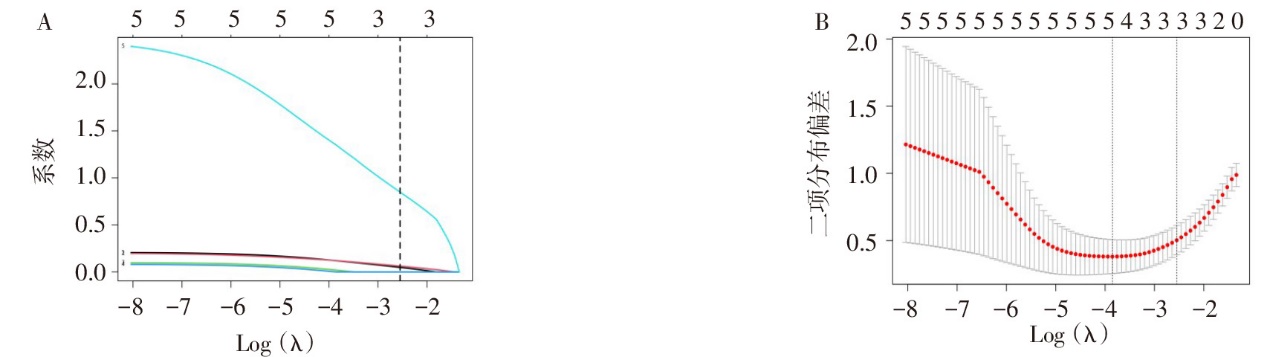
Fig.1 Selection process for Lasso regression
| 变量 | β | SE | Wald χ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| TBIL | 0.974 | 0.348 | 7.834 | 0.005 | 2.649 | 1.339~5.239 |
| mPAP | 1.126 | 0.332 | 11.503 | <0.001 | 3.082 | 1.608~5.910 |
| PVR | 1.154 | 0.315 | 13.421 | <0.001 | 3.171 | 1.710~5.879 |
| RVOTD | 0.986 | 0.346 | 8.121 | 0.004 | 2.681 | 1.361~5.281 |
| 常数项 | -3.210 | 0.850 | 14.256 | <0.001 | 0.040 |
Tab.3 Multivariate Logistic regression analysis of right heart failure after heart transplantation
| 变量 | β | SE | Wald χ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| TBIL | 0.974 | 0.348 | 7.834 | 0.005 | 2.649 | 1.339~5.239 |
| mPAP | 1.126 | 0.332 | 11.503 | <0.001 | 3.082 | 1.608~5.910 |
| PVR | 1.154 | 0.315 | 13.421 | <0.001 | 3.171 | 1.710~5.879 |
| RVOTD | 0.986 | 0.346 | 8.121 | 0.004 | 2.681 | 1.361~5.281 |
| 常数项 | -3.210 | 0.850 | 14.256 | <0.001 | 0.040 |
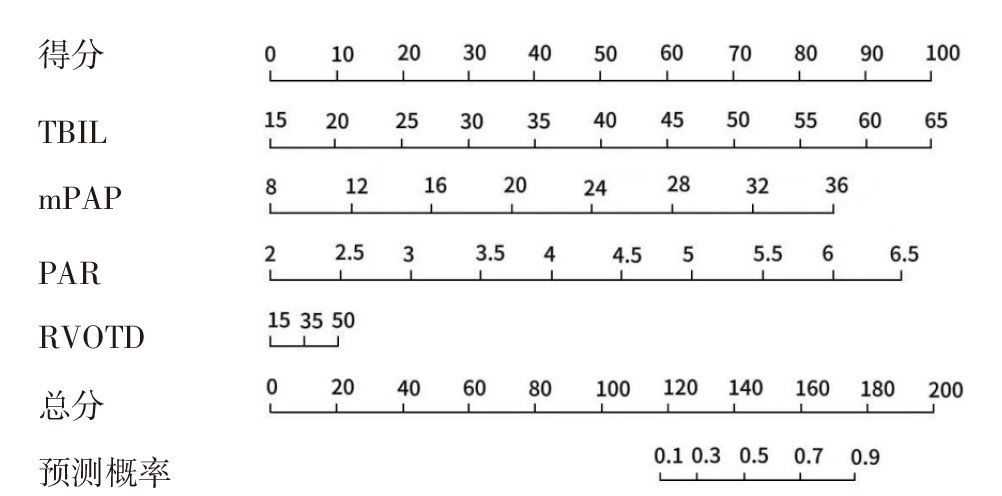
Fig.2 Nomogram for risk prediction of right heart failure after heart transplantation
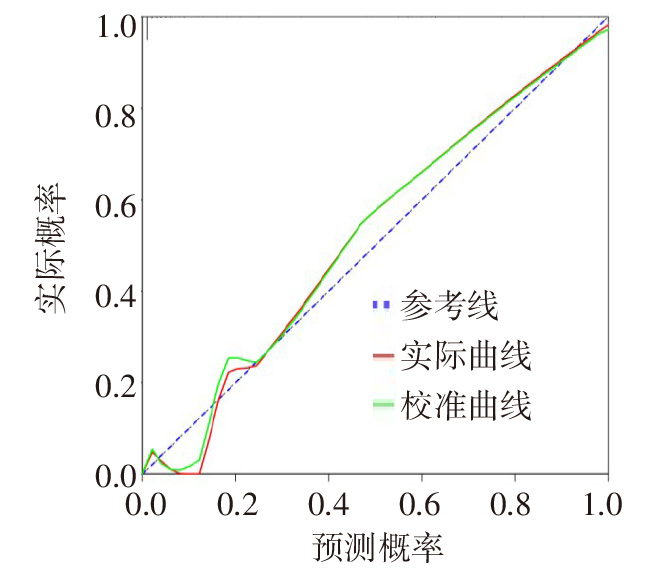
Fig.3 Calibration curve of the nomogram model
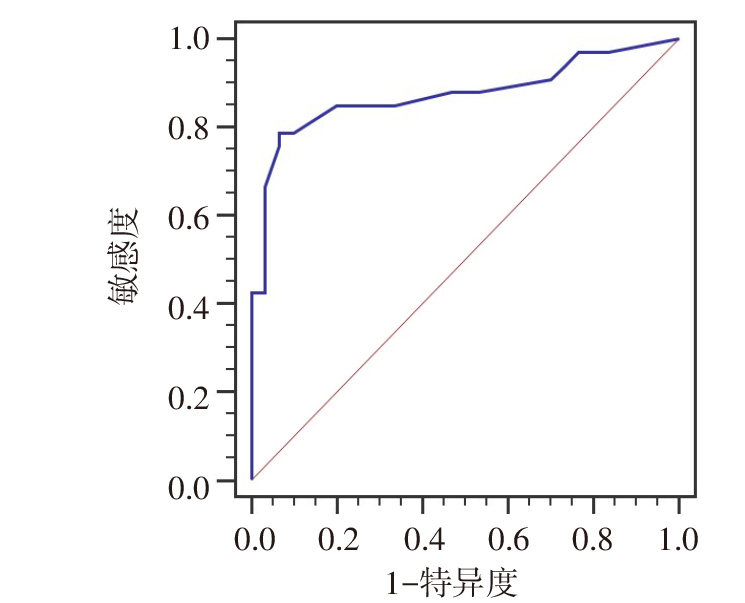
Fig.4 ROC curve of the nomogram model for predicting right heart failure
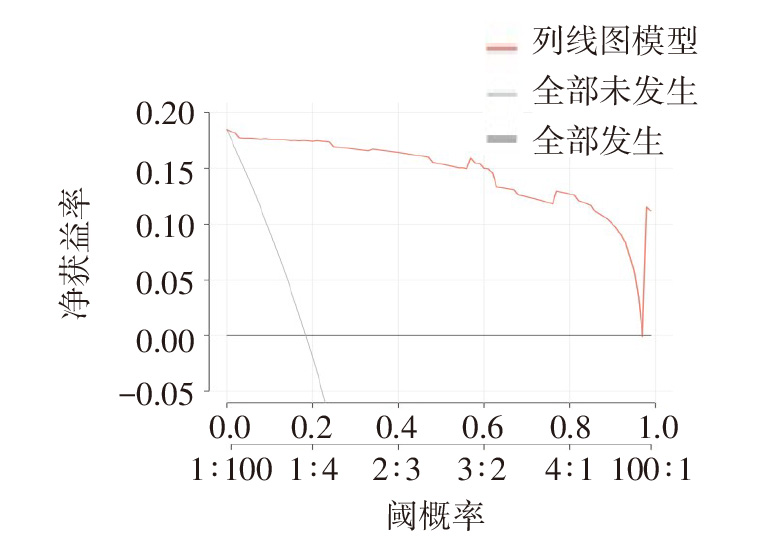
Fig.5 The decision curve analysis of nomogram model
| [1] | WU M Y, ALI KHAWAJA R D, VARGAS D. Heart transplantation:indications,surgical techniques,and complications[J]. Radiol Clin North Am, 2023, 61(5):847-859. doi:10.1016/j.rcl.2023.04.011. |
| [2] | CRESPO-LEIRO M G, COSTANZO M R, GUSTAFSSON F, et al. Heart transplantation:focus on donor recovery strategies,left ventricular assist devices,and novel therapies[J]. Eur Heart J, 2022, 43(23):2237-2246. doi:10.1093/eurheartj/ehac204. |
| [3] | HSICH E, SINGH T P, CHERIKH W S, et al. The international thoracic organ transplant registry of the international society for heart and lung transplantation:Thirty-ninth adult heart transplantation report-2022;focus on transplant for restrictive heart disease[J]. J Heart Lung Transplant, 2022, 41(10):1366-1375. doi:10.1016/j.healun.2022.07.018. |
| [4] | KANWAR M K, EVERETT K D, GULATI G, et al. Epidemiology and management of right ventricular-predominant heart failure and shock in the cardiac intensive care unit[J]. Eur Heart J Acute Cardiovasc Care, 2022, 11(7):584-594. doi:10.1093/ehjacc/zuac063. |
| [5] | BELLETTINI M, FREA S, PIDELLO S, et al. Pretransplant right ventricular dysfunction is associated with increased mortality after heart transplantation:a hard inheritance to overcome[J]. J Card Fail, 2022, 28(2):259-269. doi:10.1016/j.cardfail.2021.08.018. |
| [6] | 武才鑫, 闫彦, 邓瑗琳, 等. 心脏磁共振评估结缔组织病伴重度肺动脉高压的价值[J]. 天津医药, 2024, 52(7):691-695. |
| WU C X, YAN Y, DENG Y L, et al. Value of cardiac magnetic resonance imaging in evaluating connective tissue disease with severe pulmonary hypertension[J]. Tianjin Med J, 2024, 52(7):691-695. doi:10.11958/20231770. | |
| [7] | HUMBERT M, KOVACS G, HOEPER M M, et al. ESC/ERS scientific document group. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension[J]. Eur Heart J, 2022, 43(38):3618-3731. doi:10.1093/eurheartj/ehac237. |
| [8] | OLSSON K M, CORTE T J, KAMP J C, et al. Pulmonary hypertension associated with lung disease:new insights into pathomechanisms,diagnosis,and management[J]. Lancet Respir Med, 2023, 11(9):820-835. doi:10.1016/S2213-2600(23)00259-X. |
| [9] | CRAGER S E, HUMPHREYS C. Right ventricular failure and pulmonary hypertension[J]. Emerg Med Clin North Am, 2022, 40(3):519-537. doi:10.1016/j.emc.2022.05.006. |
| [10] | 马萌雪, 马萍, 徐清斌, 等. 急性心肌梗死并发心力衰竭的风险预测模型构建及验证[J]. 天津医药, 2023, 51(11):1221-1226. |
| MA M X, MA P, XU Q B, et al. Construction and verification of risk prediction model of acute myocardial infarction complicated with heart failure[J]. Tianjin Med J, 2023, 51(11):1221-1226. doi:10.11958/20230055. | |
| [11] | 吾拉尔·阿德力, 娜孜拉·努尔兰, 阿提开木·吾布力, 等. 建立动脉性肺动脉高压发展为右心衰的列线图预测模型[J]. 新疆医科大学学报, 2023, 46(4):453-459. |
| WULAER A D L, NAZILA N E L, ATIKAIMU W B L, et al. The nomogram prediction model of arterial pulmonary hypertension developing into right heart failure was established[J]. J Xinjiang Med Univ, 2023, 46(4):453-459. doi:10.3969/j.issn.1009-5551.2023.04.005. | |
| [12] | 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 右心衰竭诊断和治疗中国专家共识[J]. 中华心血管病杂志, 2012, 40(6):449-461. |
| Chinese Medical Association Cardiovascular Branch, Editorial Committee of Chinese Journal of Cardiology. China expert consensus on diagnosis and treatment of right heart failure[J]. Chin J Cardiol, 2012, 40(6):449-461. doi:10.3760/cma.j.issn.0253-3758.2012.06.001. | |
| [13] | KAVEEVORAYAN P, TOKAVANICH N, KITTIPIBUL V, et al. Primary isolated right ventricular failure after heart transplantation:prevalence,right ventricular characteristics,and outcomes[J]. Sci Rep, 2023, 13(1):394. doi:10.1038/s41598-023-27482-x. |
| [14] | AL-ADHAMI A, AVTAAR SINGH S S, DE S D, et al. Primary graft dysfunction after heart transplantation-unravelling the enigma[J]. Curr Probl Cardio, 2022, 47(8):100941. doi:10.1016/j.cpcardiol.2021.100941. |
| [15] | KĘDZIORA A, PIĄTEK J, HYMCZAK H, et al. Early postoperative hemodynamic instability after heart transplantation-incidence and metabolic indicators[J]. BMC Anesthesiol, 2021, 21(1):236. doi:10.1186/s12871-021-01455-x. |
| [16] | BRAHMBHATT D H, BLITZER D, BILLIA F, et al. Acute complication posttransplant:primary allograft dysfunction[J]. Curr Opin Organ Transplant, 2023, 28(5):376-383. doi:10.1097/MOT.0000000000001091. |
| [17] | 孙瑞雪, 周强, 周志明, 等. 心脏移植早期死亡的影响因素及预测模型构建[J]. 中华器官移植杂志, 2022, 43(12):723-729. |
| SUN R X, ZHOU Q, ZHOU Z M, et al. Influencing factors of early death after heart transplantation and construction of prediction model[J]. Chin J Organ Transplantat, 2022, 43(12):723-729. doi:10.3760/cma.j.cn421203-20220816-00204. | |
| [18] | GUIGNABERT C, SAVALE L, BOUCLY A, et al. Serum and pulmonary expression profiles of the activin signaling system in pulmonary arterial hypertension[J]. Circulation, 2023, 147(24):1809-1822. doi:10.1161/CIRCULATIONAHA.122.061501. |
| [19] | ZHOU W, DU Z, TAO Y, et al. Effect of preoperative pulmonary artery pressure on the prognosis of end-stage heart failure patients after heart transplantation[J]. J Cardiothorac Surg, 2023, 18(1):154. doi:10.1186/s13019-023-02253-x. |
| [20] | AHMED A, KANIA K, ABDUL RAHIM H, et al. Adrenomedullin peptides and precursor levels in relation to haemodynamics and prognosis after heart transplantation[J]. ESC Heart Fail, 2023, 10(4):2427-2437. doi:10.1002/ehf2.14399. |
| [21] | 常开丽, 刘演龙, 李昇铃, 等. 先天性心脏病相关性肺动脉高压[J]. 实用心脑肺血管病杂志, 2024, 32(1):1-8. |
| CHANG K L, LIU Y L, LI S L, et al. Congenital heart disease-related pulmonary hypertension[J]. Pract J Cardiac Cereb Pneum Vasc Disdoi, 2024, 32(1):1-8. doi:10.12114/j.issn.1008-5971.2024.00.018. | |
| [22] | LEE JY, ZAWADZKI R S, KIDAMBI S, et al. Evaluating predicted heart mass in adolescent heart transplantation[J]. J Heart Lung Transplant, 2022, 41(12):1790-1797. doi:10.1016/j.healun.2022.08.027. |
| [23] | YANAGAWA R, IWADOH K, AKABANE M, et al. LightGBM outperforms other machine learning techniques in predicting graft failure after liver transplantation:creation of a predictive model through large-scale analysis[J]. Clin Transplant, 2024, 38(4):15316. doi:10.1161/JAHA.122.028766. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||