Tianjin Medical Journal ›› 2025, Vol. 53 ›› Issue (11): 1158-1164.doi: 10.11958/20252455
• Clinical Research • Previous Articles Next Articles
WU Menglin( ), MA Fang, YANG Yafei
), MA Fang, YANG Yafei
Received:2025-07-10
Revised:2025-08-13
Published:2025-11-15
Online:2025-11-19
WU Menglin, MA Fang, YANG Yafei. Diagnostic efficacy of ultrasonic artificial intelligence combined with BRAF V600E gene testing in differentiating benign-malignant and invasive thyroid nodules[J]. Tianjin Medical Journal, 2025, 53(11): 1158-1164.
CLC Number:
| 组别 | n | 性别(男/女) | 年龄/岁 | 辐射接触史 |
|---|---|---|---|---|
| 良性组 | 150 | 52/98 | 46.00(36.00,59.00) | 2(1.33) |
| 恶性组 | 150 | 57/93 | 49.00(39.00,60.00) | 7(4.67) |
| χ2或Z | 0.360 | 1.278 | 1.833 | |
| 组别 | 碘暴露史 | 甲状腺疾病史 | 甲状腺疾病家族史 | |
| 良性组 | 3(2.00) | 23(15.33) | 18(12.00) | |
| 恶性组 | 9(6.00) | 32(21.33) | 21(14.00) | |
| χ2 | 3.125 | 1.803 | 0.265 | |
Tab.1 Comparison of general clinical characteristics between the benign group and the malignant group
| 组别 | n | 性别(男/女) | 年龄/岁 | 辐射接触史 |
|---|---|---|---|---|
| 良性组 | 150 | 52/98 | 46.00(36.00,59.00) | 2(1.33) |
| 恶性组 | 150 | 57/93 | 49.00(39.00,60.00) | 7(4.67) |
| χ2或Z | 0.360 | 1.278 | 1.833 | |
| 组别 | 碘暴露史 | 甲状腺疾病史 | 甲状腺疾病家族史 | |
| 良性组 | 3(2.00) | 23(15.33) | 18(12.00) | |
| 恶性组 | 9(6.00) | 32(21.33) | 21(14.00) | |
| χ2 | 3.125 | 1.803 | 0.265 | |
| 组别 | n | 性别(男/女) | 年龄/岁 | 辐射接触史 |
|---|---|---|---|---|
| 未侵袭组 | 84 | 27/57 | 47.50(38.25,58.75) | 2(2.38) |
| 侵袭组 | 66 | 30/36 | 50.50(39.00,61.00) | 5(7.58) |
| χ2或Z | 2.780 | 0.922 | 1.226 | |
| 组别 | 碘暴露史 | 甲状腺疾病史 | 甲状腺疾病家族史 | |
| 未侵袭组 | 3(3.57) | 14(16.67) | 11(13.10) | |
| 侵袭组 | 6(9.09) | 18(27.27) | 10(15.15) | |
| χ2 | 1.138 | 2.477 | 0.130 | |
Tab.2 Comparison of general clinical characteristics between the non-invasive group and the invasive group
| 组别 | n | 性别(男/女) | 年龄/岁 | 辐射接触史 |
|---|---|---|---|---|
| 未侵袭组 | 84 | 27/57 | 47.50(38.25,58.75) | 2(2.38) |
| 侵袭组 | 66 | 30/36 | 50.50(39.00,61.00) | 5(7.58) |
| χ2或Z | 2.780 | 0.922 | 1.226 | |
| 组别 | 碘暴露史 | 甲状腺疾病史 | 甲状腺疾病家族史 | |
| 未侵袭组 | 3(3.57) | 14(16.67) | 11(13.10) | |
| 侵袭组 | 6(9.09) | 18(27.27) | 10(15.15) | |
| χ2 | 1.138 | 2.477 | 0.130 | |
| 组别 | 结节数量 | 结节位置 | 最大直径 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单发 | 多发 | 左叶 | 右叶 | 峡部 | 混合 | ≤1 cm | >1 cm | ||||||||||
| 良性组 | 90(60.00) | 60(40.00) | 60(40.00) | 58(38.67) | 8(5.33) | 24(16.00) | 97(64.67) | 53(35.33) | |||||||||
| 恶性组 | 102(68.00) | 48(32.00) | 54(36.00) | 63(42.00) | 15(10.00) | 18(12.00) | 51(40.00) | 99(66.00) | |||||||||
| χ2 | 2.083 | 3.510 | 28.218** | ||||||||||||||
| 组别 | 结节结构 | 回声类型 | 钙化类型 | 边界 | |||||||||||||
| 囊性 | 实性 | 无回声 | 极低回声/ 低回声 | 等回声/ 高回声 | 混合回声 | 无 | 微钙化 | 粗钙化 | 清晰 | 模糊 | |||||||
| 良性组 | 105(70.00) | 45(30.00) | 24(16.00) | 45(30.00) | 72(48.00) | 9(6.00) | 90(60.00) | 14(9.33) | 46(30.67) | 120(80.00) | 30(20.00) | ||||||
| 恶性组 | 7(4.67) | 143(95.33) | 3(2.00) | 126(84.00) | 15(10.00) | 6(4.00) | 32(21.33) | 103(68.67) | 15(10.00) | 33(22.00) | 117(78.00) | ||||||
| χ2 | 136.835** | 92.647** | 111.029** | 100.960** | |||||||||||||
| 组别 | 形态 | 纵横比 | 血流分布 | 血流丰富度 | |||||||||||||
| 规则 | 不规则 | ≤1 | >1 | 周边 | 内部/混合 | Ⅰ—Ⅱ级 | Ⅲ—Ⅴ级 | ||||||||||
| 良性组 | 103(68.67) | 47(31.33) | 134(89.33) | 16(10.67) | 82(54.67) | 68(45.33) | 115(76.67) | 35(23.33) | |||||||||
| 恶性组 | 50(33.33) | 100(66.67) | 49(32.67) | 101(67.33) | 20(13.33) | 130(86.67) | 53(35.33) | 97(64.67) | |||||||||
| χ2 | 37.468** | 101.233** | 57.100** | 52.002** | |||||||||||||
Tab.3 Comparison of ultrasound AI features between the two groups
| 组别 | 结节数量 | 结节位置 | 最大直径 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单发 | 多发 | 左叶 | 右叶 | 峡部 | 混合 | ≤1 cm | >1 cm | ||||||||||
| 良性组 | 90(60.00) | 60(40.00) | 60(40.00) | 58(38.67) | 8(5.33) | 24(16.00) | 97(64.67) | 53(35.33) | |||||||||
| 恶性组 | 102(68.00) | 48(32.00) | 54(36.00) | 63(42.00) | 15(10.00) | 18(12.00) | 51(40.00) | 99(66.00) | |||||||||
| χ2 | 2.083 | 3.510 | 28.218** | ||||||||||||||
| 组别 | 结节结构 | 回声类型 | 钙化类型 | 边界 | |||||||||||||
| 囊性 | 实性 | 无回声 | 极低回声/ 低回声 | 等回声/ 高回声 | 混合回声 | 无 | 微钙化 | 粗钙化 | 清晰 | 模糊 | |||||||
| 良性组 | 105(70.00) | 45(30.00) | 24(16.00) | 45(30.00) | 72(48.00) | 9(6.00) | 90(60.00) | 14(9.33) | 46(30.67) | 120(80.00) | 30(20.00) | ||||||
| 恶性组 | 7(4.67) | 143(95.33) | 3(2.00) | 126(84.00) | 15(10.00) | 6(4.00) | 32(21.33) | 103(68.67) | 15(10.00) | 33(22.00) | 117(78.00) | ||||||
| χ2 | 136.835** | 92.647** | 111.029** | 100.960** | |||||||||||||
| 组别 | 形态 | 纵横比 | 血流分布 | 血流丰富度 | |||||||||||||
| 规则 | 不规则 | ≤1 | >1 | 周边 | 内部/混合 | Ⅰ—Ⅱ级 | Ⅲ—Ⅴ级 | ||||||||||
| 良性组 | 103(68.67) | 47(31.33) | 134(89.33) | 16(10.67) | 82(54.67) | 68(45.33) | 115(76.67) | 35(23.33) | |||||||||
| 恶性组 | 50(33.33) | 100(66.67) | 49(32.67) | 101(67.33) | 20(13.33) | 130(86.67) | 53(35.33) | 97(64.67) | |||||||||
| χ2 | 37.468** | 101.233** | 57.100** | 52.002** | |||||||||||||
| 组别 | n | 结节数量 | 结节位置 | 最大直径 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单发 | 多发 | 左叶 | 右叶 | 峡部 | 混合 | ≤1 cm | >1 cm | |||||||||||||||||
| 未侵袭组 | 84 | 62(73.81) | 22(26.19) | 32(38.10) | 33(39.29) | 7(8.33) | 12(14.29) | 35(41.67) | 49(58.33) | |||||||||||||||
| 侵袭组 | 66 | 40(60.61) | 26(39.39) | 22(33.33) | 30(45.45) | 8(12.12) | 6(9.09) | 16(24.24) | 50(75.76) | |||||||||||||||
| χ2 | 2.961 | 1.929 | 5.001* | |||||||||||||||||||||
| 组别 | 结节结构 | 回声类型 | 钙化类型 | 边界 | ||||||||||||||||||||
| 囊性 | 实性 | 无回声 | 极低回声/低回声 | 等回声/ 高回声 | 混合回声 | 无 | 微钙化 | 粗钙化 | 清晰 | 模糊 | ||||||||||||||
| 未侵袭组 | 7(8.33) | 77(91.67) | 3(3.57) | 64(76.19) | 13(15.48) | 4(4.76) | 26(30.95) | 45(53.57) | 13(15.48) | 29(34.52) | 55(65.48) | |||||||||||||
| 侵袭组 | 0 | 66(100.00) | 0 | 62(93.94) | 2(3.03) | 2(3.03) | 6(9.09) | 58(87.88) | 2(3.03) | 4(6.06) | 62(93.94) | |||||||||||||
| χ2 | 4.048* | 11.719** | 20.340** | 17.449** | ||||||||||||||||||||
| 组别 | 形态 | 纵横比 | 血流分布 | 血流丰富度 | ||||||||||||||||||||
| 规则 | 不规则 | ≤1 | >1 | 周边 | 内部/混合 | Ⅰ—Ⅱ级 | Ⅲ—Ⅴ级 | |||||||||||||||||
| 未侵袭组 | 38(45.24) | 46(54.76) | 29(34.52) | 55(65.48) | 16(19.05) | 68(80.95) | 45(53.57) | 39(46.43) | ||||||||||||||||
| 侵袭组 | 12(18.18) | 54(81.82) | 20(30.30) | 46(69.70) | 4(6.06) | 62(93.94) | 8(12.12) | 58(87.88) | ||||||||||||||||
| χ2 | 12.175** | 0.299 | 5.395* | 27.792** | ||||||||||||||||||||
Tab.4 Comparison of ultrasound AI characteristics between the non-invasive group and the invasive group of thyroid nodules
| 组别 | n | 结节数量 | 结节位置 | 最大直径 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 单发 | 多发 | 左叶 | 右叶 | 峡部 | 混合 | ≤1 cm | >1 cm | |||||||||||||||||
| 未侵袭组 | 84 | 62(73.81) | 22(26.19) | 32(38.10) | 33(39.29) | 7(8.33) | 12(14.29) | 35(41.67) | 49(58.33) | |||||||||||||||
| 侵袭组 | 66 | 40(60.61) | 26(39.39) | 22(33.33) | 30(45.45) | 8(12.12) | 6(9.09) | 16(24.24) | 50(75.76) | |||||||||||||||
| χ2 | 2.961 | 1.929 | 5.001* | |||||||||||||||||||||
| 组别 | 结节结构 | 回声类型 | 钙化类型 | 边界 | ||||||||||||||||||||
| 囊性 | 实性 | 无回声 | 极低回声/低回声 | 等回声/ 高回声 | 混合回声 | 无 | 微钙化 | 粗钙化 | 清晰 | 模糊 | ||||||||||||||
| 未侵袭组 | 7(8.33) | 77(91.67) | 3(3.57) | 64(76.19) | 13(15.48) | 4(4.76) | 26(30.95) | 45(53.57) | 13(15.48) | 29(34.52) | 55(65.48) | |||||||||||||
| 侵袭组 | 0 | 66(100.00) | 0 | 62(93.94) | 2(3.03) | 2(3.03) | 6(9.09) | 58(87.88) | 2(3.03) | 4(6.06) | 62(93.94) | |||||||||||||
| χ2 | 4.048* | 11.719** | 20.340** | 17.449** | ||||||||||||||||||||
| 组别 | 形态 | 纵横比 | 血流分布 | 血流丰富度 | ||||||||||||||||||||
| 规则 | 不规则 | ≤1 | >1 | 周边 | 内部/混合 | Ⅰ—Ⅱ级 | Ⅲ—Ⅴ级 | |||||||||||||||||
| 未侵袭组 | 38(45.24) | 46(54.76) | 29(34.52) | 55(65.48) | 16(19.05) | 68(80.95) | 45(53.57) | 39(46.43) | ||||||||||||||||
| 侵袭组 | 12(18.18) | 54(81.82) | 20(30.30) | 46(69.70) | 4(6.06) | 62(93.94) | 8(12.12) | 58(87.88) | ||||||||||||||||
| χ2 | 12.175** | 0.299 | 5.395* | 27.792** | ||||||||||||||||||||
| 超声AI | 术后病理 | 术后病理 | ||||
|---|---|---|---|---|---|---|
| 恶性 | 良性 | 合计 | 侵袭 | 未侵袭 | 合计 | |
| ≥0.5 | 135 | 29 | 164 | 56 | 14 | 70 |
| <0.5 | 15 | 121 | 136 | 10 | 70 | 80 |
| 合计 | 150 | 150 | 300 | 66 | 84 | 150 |
Tab.5 Comparion of ultrasound AI diagnosis and postoperative pathological conditions of thyroid nodules
| 超声AI | 术后病理 | 术后病理 | ||||
|---|---|---|---|---|---|---|
| 恶性 | 良性 | 合计 | 侵袭 | 未侵袭 | 合计 | |
| ≥0.5 | 135 | 29 | 164 | 56 | 14 | 70 |
| <0.5 | 15 | 121 | 136 | 10 | 70 | 80 |
| 合计 | 150 | 150 | 300 | 66 | 84 | 150 |
| BRAF V600E | 术后病理 | 术后病理 | ||||
|---|---|---|---|---|---|---|
| 恶性 | 良性 | 合计 | 侵袭 | 未侵袭 | 合计 | |
| 阳性 | 109 | 15 | 124 | 49 | 10 | 59 |
| 阴性 | 41 | 135 | 176 | 17 | 74 | 72 |
| 合计 | 150 | 150 | 300 | 66 | 84 | 150 |
Tab.6 Comparison of BRAF V600E gene diagnosis and postoperative pathological conditions of thyroid nodules
| BRAF V600E | 术后病理 | 术后病理 | ||||
|---|---|---|---|---|---|---|
| 恶性 | 良性 | 合计 | 侵袭 | 未侵袭 | 合计 | |
| 阳性 | 109 | 15 | 124 | 49 | 10 | 59 |
| 阴性 | 41 | 135 | 176 | 17 | 74 | 72 |
| 合计 | 150 | 150 | 300 | 66 | 84 | 150 |
| 指标 | AUC | 95%CI | 约登指数 |
|---|---|---|---|
| 超声AI | 0.853 | 0.807~0.900 | 0.707 |
| BRAF V600E基因 | 0.813 | 0.762~0.864 | 0.627 |
| 联合检测 | 0.941 | 0.917~0.966 | 0.727 |
Tab.7 Diagnostic efficacy of combined AI ultrasound and BRAF V600E testing for malignant thyroid nodules
| 指标 | AUC | 95%CI | 约登指数 |
|---|---|---|---|
| 超声AI | 0.853 | 0.807~0.900 | 0.707 |
| BRAF V600E基因 | 0.813 | 0.762~0.864 | 0.627 |
| 联合检测 | 0.941 | 0.917~0.966 | 0.727 |
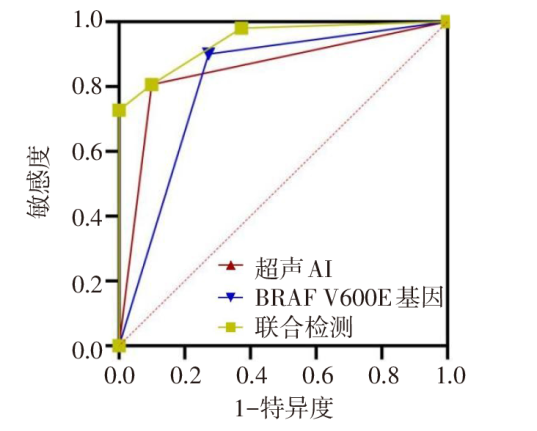
Fig.1 ROC curve of combined AI ultrasound and BRAF V600E testing for predicting malignant thyroid nodules
| 指标 | AUC | 95%CI | 约登指数 |
|---|---|---|---|
| 超声AI | 0.841 | 0.773~0.909 | 0.681 |
| BRAF V600E基因 | 0.812 | 0.737~0.886 | 0.623 |
| 联合检测 | 0.924 | 0.880~0.967 | 0.774 |
Tab.8 Diagnostic efficacy of combined AI ultrasound and BRAF V600E testing for invasive malignant thyroid nodules
| 指标 | AUC | 95%CI | 约登指数 |
|---|---|---|---|
| 超声AI | 0.841 | 0.773~0.909 | 0.681 |
| BRAF V600E基因 | 0.812 | 0.737~0.886 | 0.623 |
| 联合检测 | 0.924 | 0.880~0.967 | 0.774 |
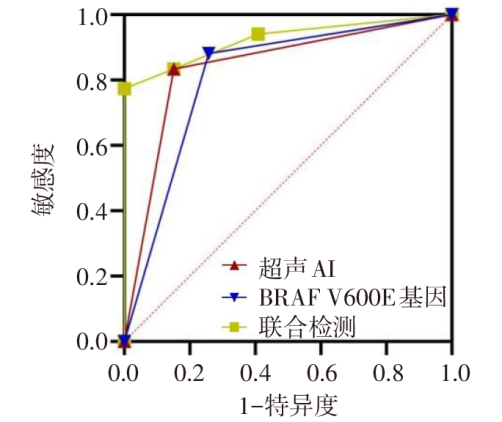
Fig.2 ROC curve of combined AI ultrasound and BRAF V600E testing for predicting invasive malignant thyroid nodules
| [1] | 中国医师协会外科医师分会甲状腺外科专家工作组, 中国研究型医院学会甲状腺疾病专业委员会, 等. 超声引导下甲状腺结节和颈部淋巴结细针穿刺活检中国专家共识及操作指南(2025版)[J]. 中国实用外科杂志, 2025, 45(1):34-41. |
| Expert Working Group of Thyroid Association,College of Surgeons, Chinese Medical Doctor Association, Chinese Research Hospital Association Thyroid Disease Committee, et al. Chinese experts consensus and operational guidelines on ultrasound guided fine-needle aspiration biopsy of thyroid nodule and cervical lymph node(2025 edition)[J]. Chinese Journal of Practical Surgery, 2025, 45(1):34-41. doi:10.19538/j.cjps.issn1005-2208.2025.01.05. | |
| [2] | 杨桃, 全艳, 张加孟, 等. 甲状腺结节细针穿刺细胞学联合BRAF基因检测在甲状腺良恶性肿瘤鉴别诊断中的应用价值[J]. 天津医药, 2025, 53(9):972-976. |
| YANG T, QUAN Y, ZHANG J M, et al. Application value of thyroid nodule fine needle aspiration cytology combined with BRAF gene detection in the differential diagnosis of benign and malignant thyroid tumors[J]. Tianjin Med J, 2025, 53(9):972-976. doi:10.11958/20241258. | |
| [3] | 蔡文卿, 崔灿, 刘洁, 等. BRAFV600E基因突变检测在细针穿刺细胞学良性甲状腺结节中的应用价值[J]. 中国普通外科杂志, 2024, 33(11):1786-1793. |
| CAI W Q, CUI C, LIU J, et al. The application value of BRAFV600Egene mutation testing in fine-needle aspiration biopsy diagnosed benign thyroid nodules[J]. China Journal of General Surgery, 2024, 33(11):1786-1793. doi:10.7659/j.issn.1005-6947.2024.11.005. | |
| [4] | 刘凌晓, 董怡. 人工智能技术在甲状腺结节诊断及预测淋巴结转移中的应用[J]. 介入放射学杂志, 2021, 30(4):4. |
| LIU L X, DONG Y. Application of artificial inteligenee technology in diagnosing thyroid nodules and predicting lymphnode metastasis[J]. J Intervent Radiol, 2021, 30(4):4. doi:10.3969/j.issn.1008-794X.2021.04.001. | |
| [5] | MENDES J M, ELSHEIKH T M, DI MARCO J, et al. Are there specific cytologic features that can predict BRAFV600E mutational status of papillary thyroid carcinoma in fine-needle aspiration specimens?[J]. Diagn Cytopathol. 2024, 52(6):295-302. doi:10.1002/dc.25290. |
| [6] | DURANTE C, HEGEDüS L, CZARNIECKA A, et al. 2023 European Thyroid Association Clinical Practice Guidelines for thyroid nodule management[J]. Eur Thyroid J, 2023, 12(5):e230067. doi:10.1530/ETJ-23-0067. |
| [7] | 刘江云, 李利霞, 刘新羽. 超声AI、弹性应变率及TSH检测在甲状腺结节良恶性鉴别中的应用研究[J]. 临床和实验医学杂志, 2024, 23(22):2438-2442. |
| LIU J Y, LI L X, LIU X Y. Application of ultrasonic AI,elastic strain rate and TSH detection in differential diagnosis of benign and malignant thyroid nodules[J]. Journal of Clinical and Experimental Medicine, 2024, 23(22):2438-2442. doi:10.3969/j.issn.1671-4695.2024.22.023. | |
| [8] | 中华医学超声杂志(电子版)编辑委员会浅表器官学组. 甲状腺结节超声诊断规范[J]. 中华医学超声杂志(电子版), 2017, 14(4):241-244. |
| Editorial Board of Chinese Journal of Medical Ultrasound(Electronic Edition),Superficial Organ Subgroup. Standardization for thyroid nodule ultrasound diagnosis[J]. Chin J Med Ultrasotmd(Electronic Edition), 2017, 14(4):241-244. doi:10.3877/cma.j.issn.1672-6448.2017.04.001. | |
| [9] | 广东省医学教育协会甲状腺专业委员会, 广东省基层医药学会细胞病理与分子诊断专业委员会. 甲状腺癌基因检测与临床应用广东专家共识(2020版)[J]. 中华普通外科学文献(电子版), 2020, 14(3):161-168. |
| Guangdong Medical Education Association Thyroid Specialized Committee, Guangdong Primary Healthcare Association Cellular Pathology and Molecular Diagnosis Specialized Committee. Guangdong expert consensus on gene testing and clinical application in thyroid cancer(Version 2020)[J]. Chin Arch Gen Surg(Electronic Edition), 2020, 14(3):161-168. doi:10.3877/cma.j.issn.1674-0793.2020.03.001. | |
| [10] | 杨蕊菲, 刘葆婧, 武曼, 等. 血浆ctDNA中HOXA7、SOX17甲基化联合影像学指标在肺癌早诊中的应用研究[J]. 重庆医科大学学报, 2025, 50(3):403-408. |
| YANG R F, LIU B J, WU M, et al. Application of radiological indicators combined with the methylation of HOXA7 and SOX17 in plasma circulating tumor DNA in the early diagnosis of lung cancer[J]. Journal of Chongqing Medical University, 2025, 50(3):403-408. doi:10.13406/j.cnki.cyxb.003715. | |
| [11] | 李晓宇, 刘利平, 辛雨薇, 等. 人工智能软件联合超声造影鉴别诊断甲状腺良、恶性结节[J]. 中国医学影像学杂志, 2023, 31(3):226-230. |
| LI X Y, LIU L P, XIN Y W, et al. Diagnosis of artificial intelligence software combined with contrast-enhanced ultrasound in differentiating benign from malignant thyroid nodules[J]. Chinese Journal of Medical Imaging, 2023, 31(3):226-230. doi:10.3969/j.issn.1005-5185.2023.03.007. | |
| [12] | 张萌, 金壮, 赵蕙琳, 等. 多模态超声联合临床特征建立对甲状腺结节良恶性诊断的预测模型[J]. 中国医学影像学杂志, 2024, 32(1):14-20. |
| ZHANG M, JIN Z, ZHAO H L, et al. Establishment of a predictive model for the diagnosis of benign and malignant thyroid nodulesvia multimodal ultrasound combined with thyroid hormone[J]. Chinese Journal of Medical Imaging, 2024, 32(1):14-20. doi:10.3969/j.issn.1005-5185.2024.01.003. | |
| [13] | FU J, LIN J, DAI Z, et al. Hypoxia-associated autophagy flux dysregulation in human cancers[J]. Cancer Lett, 2024, 590(5):216823. doi:10.1016/j.canlet.2024.216823. |
| [14] | 赵玲, 马步云. 甲状腺髓样癌和甲状腺乳头状癌的超声特征研究[J]. 现代肿瘤医学, 2023, 31(16):3010-3014. |
| ZHAO L, MA B Y. Ultrasonographic features study of medullary thyroid carcinoma and papillaithyroid carcinoma[J]. Modern Oncology, 2023, 31(16):3010-3014. doi:10.3969/j.issn.1672-4992.2023.16.011. | |
| [15] | 侯婷婷, 夏燕妮, 张红伟. C-TIRADS联合cfDNA鉴别诊断甲状腺结节价值及临床效用评价[J]. 河北医药, 2023, 45(18):2736-2740. |
| HOU T T, XIA Y N, ZHANG H W. Evaluation of the value and clinical application of the Chinese thyroid imaging reports and data systems combined with circulating free DNA detection in the differential diagnosis of thyroid nodules[J]. Hebei Medical Journal, 2023, 45(18):2736-2740. doi:10.3969/j.issn.1002-7386.2023.18.003. | |
| [16] | 周芳, 张刚, 李欢, 等. 甲状腺乳头状癌超声图像特征及BRAF V600E突变与颈部淋巴结转移的关系[J]. 临床超声医学杂志, 2023, 25(4):289-293. |
| ZHOU F, ZHANG G, LI H, et al. Correlation of ultrasonographic characteristics,BRAF V600E gene mutation and cervical lymph node metastasis in papillary thyroid carcinoma[J]. J Clin Ultrasound in Med, 2023, 25(4):289-293. doi:10.3969/j.issn.1008-6978.2023.04.011. | |
| [17] | VIMALRAJ S. A concise review of VEGF,PDGF,FGF,Notch,angiopoietin,and HGF signalling in tumor angiogenesis with a focus on alternative approaches and future directions[J]. Int J Biol Macromol, 2022, 221(11):1428-1438. doi:10.1016/j.ijbiomac.2022.09.129. |
| [18] | ZOU M, AL-YAHYA S, AL-ALWAN M, et al. β-catenin attenuation leads to up-regulation of activating NKG2D ligands and tumor regression in BrafV600E-driven thyroid cancer cells[J]. Front Immunol, 2023, 14(7):1171816. doi:10.3389/fimmu.2023.1171816. |
| [19] | 常晨, 房国栋, 雷建园, 等. 免疫组化检测BRAF V600E突变在甲状腺乳头状癌中的应用[J]. 国际遗传学杂志, 2022, 45(6):441-447. |
| CHANG C, FANG G D, LEI J Y, et al. Immunohistochemical detection of BRAF V600E mutation in papillary thyroid cancer[J]. International Journal of Genetics, 2022, 45(6):441-447. doi:10.3760/cma.j.cn231536-20220801-00072. | |
| [20] | 吴宪吉, 肖思齐, 沈珂羽, 等. BRAF V600E突变与甲状腺乳头状癌临床病理特征关系的研究进展[J]. 中国实验诊断学, 2024, 28(2):219-223. |
| WU X J, XIAO S Q, SHEN K Y, et al. Research progress on the relationship between BRAF V600E mutation and clinicopathological features of papillary thyroid carcinoma[J]. Chinese Journal of Laboratory Diagnosis, 2024, 28(2):219-223. doi:10.3969/j.issn.1007-4287.2024.02.021. | |
| [21] | 赵思童, 胡晓东, 许怀瑾, 等. 桥本甲状腺炎超声与病理学诊断的一致性分析[J]. 解放军医学杂志, 2023, 48(5):530-536. |
| ZHAO S T, HU X D, XU H J, et al. Analysis of consistency between ultrasound and pathological diagnosis of Hashimoto thyroiditis[J]. Med J Chin PLA, 2023, 48(5):530-536. doi:10.11855/j.issn.0577-7402.2023.05.0530. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||