Tianjin Medical Journal ›› 2024, Vol. 52 ›› Issue (6): 653-657.doi: 10.11958/20231362
• Applied Research • Previous Articles Next Articles
GU Cheng( ), SHEN Xinyu, SUN Jinghua, YAN Saike, WANG Haiping()
), SHEN Xinyu, SUN Jinghua, YAN Saike, WANG Haiping()
Received:2023-09-07
Revised:2023-12-05
Published:2024-06-15
Online:2024-06-06
Contact:
△E-mail: GU Cheng, SHEN Xinyu, SUN Jinghua, YAN Saike, WANG Haiping. The evaluation value of dynamic MRI imaging technology for LARS after anorectal preservation surgery in low rectal cancer[J]. Tianjin Medical Journal, 2024, 52(6): 653-657.
CLC Number:
| 序列 | TR/TE/ms | 层厚/层距/mm | 扫描视野/mm | 矩阵 | 激励次数 |
|---|---|---|---|---|---|
| T2WI矢状位 | 7 500/96 | 5/0.5 | 280×280 | 320×320 | 1 |
| T1WI轴位 | 450/8.6 | 6/0.6 | 420×420 | 384×384 | 2 |
| HR-MRI T2WI轴位 | 5 600/104 | 3/0.3 | 200×200 | 384×384 | 2 |
| T2WI冠状位 | 3 500/82 | 4/0.4 | 300×225 | 448×336 | 1 |
| 提肛相T2WI矢状位 | 2 410 /132 | 5.5/0.5 | 220×220 | 256×256 | 1 |
| 力排相T2WI矢状位 | 2 410 /132 | 5.5/0.5 | 220×220 | 256×256 | 1 |
| 提肛相T2WI轴位 | 2 450/131 | 4/0.4 | 250×250 | 320×320 | 1 |
| 力排相T2WI轴位 | 2 450/131 | 4/0.4 | 250×250 | 320×320 | 1 |
Tab.1 Sequence parameters of conventional and dynamic MRI examinations
| 序列 | TR/TE/ms | 层厚/层距/mm | 扫描视野/mm | 矩阵 | 激励次数 |
|---|---|---|---|---|---|
| T2WI矢状位 | 7 500/96 | 5/0.5 | 280×280 | 320×320 | 1 |
| T1WI轴位 | 450/8.6 | 6/0.6 | 420×420 | 384×384 | 2 |
| HR-MRI T2WI轴位 | 5 600/104 | 3/0.3 | 200×200 | 384×384 | 2 |
| T2WI冠状位 | 3 500/82 | 4/0.4 | 300×225 | 448×336 | 1 |
| 提肛相T2WI矢状位 | 2 410 /132 | 5.5/0.5 | 220×220 | 256×256 | 1 |
| 力排相T2WI矢状位 | 2 410 /132 | 5.5/0.5 | 220×220 | 256×256 | 1 |
| 提肛相T2WI轴位 | 2 450/131 | 4/0.4 | 250×250 | 320×320 | 1 |
| 力排相T2WI轴位 | 2 450/131 | 4/0.4 | 250×250 | 320×320 | 1 |
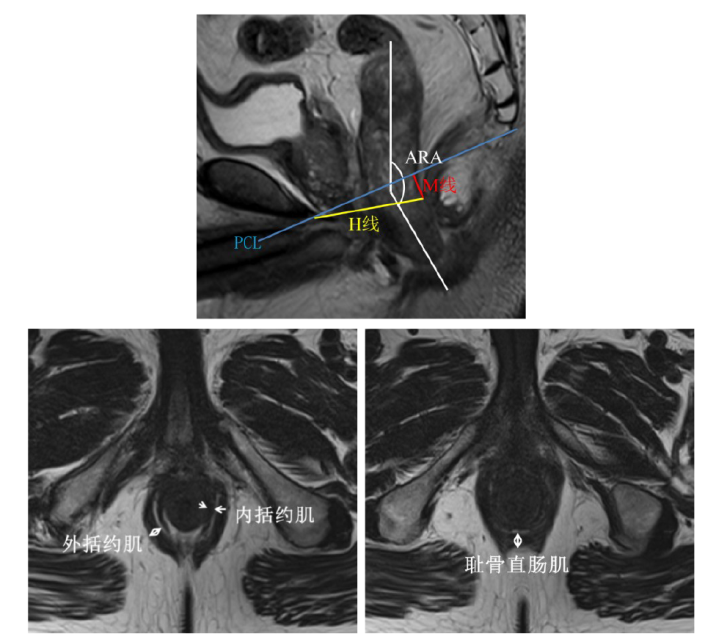
Fig.1 Measurement of MRI image indices
| 时相 | ARA/° | H线/mm | M线/mm | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 术前 | 术后 | t | 术前 | 术后 | t | 术前 | 术后 | t | ||||||||||
| 静息相 | 107.94±11.44 | 117.38±13.38 | 5.416** | 57.19±7.69 | 54.70±7.53 | 1.703 | 11.18±5.10 | 11.75±7.73 | 0.434 | |||||||||
| 提肛相 | 91.59±14.19a | 98.70±13.03a | 2.796** | 53.29±7.03a | 51.99±7.75 | 0.840 | 6.02±6.20a | 5.03±8.59a | 0.594 | |||||||||
| 力排相 | 116.14±12.73ab | 122.10±13.33b | 2.874** | 59.80±8.14b | 58.38±10.13b | 0.695 | 17.68±7.14ab | 19.38±10.91ab | 0.876 | |||||||||
| F | 33.162** | 30.532** | 6.451** | 4.918** | 66.691** | 21.425** | ||||||||||||
| 时相 | 耻骨直肠肌厚度/mm | 内括约肌厚度/mm | 外括约肌厚度/mm | |||||||||||||||
| 术前 | 术后 | t | 术前 | 术后 | t | 术前 | 术后 | t | ||||||||||
| 静息相 | 7.12±1.22 | 5.34±1.70 | 5.508** | 3.07±0.65 | 2.66±0.75 | 2.840** | 4.84±0.97 | 3.59±1.26 | 5.005** | |||||||||
| 提肛相 | 8.43±1.39a | 6.10±1.71 | 7.010** | 3.30±0.57 | 2.93±0.73 | 2.523* | 5.71±1.11a | 3.94±1.26 | 6.879** | |||||||||
| 力排相 | 6.59±1.33b | 5.46±1.44 | 3.922** | 2.70±0.55ab | 2.64±0.71 | 0.510 | 4.57±1.01b | 3.61±1.12 | 4.124** | |||||||||
| F | 17.948** | 2.207 | 8.958** | 1.646 | 11.748** | 0.907 | ||||||||||||
Tab.2 Preoperative/postoperative MRI indicators at three phases
| 时相 | ARA/° | H线/mm | M线/mm | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 术前 | 术后 | t | 术前 | 术后 | t | 术前 | 术后 | t | ||||||||||
| 静息相 | 107.94±11.44 | 117.38±13.38 | 5.416** | 57.19±7.69 | 54.70±7.53 | 1.703 | 11.18±5.10 | 11.75±7.73 | 0.434 | |||||||||
| 提肛相 | 91.59±14.19a | 98.70±13.03a | 2.796** | 53.29±7.03a | 51.99±7.75 | 0.840 | 6.02±6.20a | 5.03±8.59a | 0.594 | |||||||||
| 力排相 | 116.14±12.73ab | 122.10±13.33b | 2.874** | 59.80±8.14b | 58.38±10.13b | 0.695 | 17.68±7.14ab | 19.38±10.91ab | 0.876 | |||||||||
| F | 33.162** | 30.532** | 6.451** | 4.918** | 66.691** | 21.425** | ||||||||||||
| 时相 | 耻骨直肠肌厚度/mm | 内括约肌厚度/mm | 外括约肌厚度/mm | |||||||||||||||
| 术前 | 术后 | t | 术前 | 术后 | t | 术前 | 术后 | t | ||||||||||
| 静息相 | 7.12±1.22 | 5.34±1.70 | 5.508** | 3.07±0.65 | 2.66±0.75 | 2.840** | 4.84±0.97 | 3.59±1.26 | 5.005** | |||||||||
| 提肛相 | 8.43±1.39a | 6.10±1.71 | 7.010** | 3.30±0.57 | 2.93±0.73 | 2.523* | 5.71±1.11a | 3.94±1.26 | 6.879** | |||||||||
| 力排相 | 6.59±1.33b | 5.46±1.44 | 3.922** | 2.70±0.55ab | 2.64±0.71 | 0.510 | 4.57±1.01b | 3.61±1.12 | 4.124** | |||||||||
| F | 17.948** | 2.207 | 8.958** | 1.646 | 11.748** | 0.907 | ||||||||||||
| 组别 | n | ARA/° | H线/mm | M线/mm | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 静息相 | 提肛相 | 力排相 | 静息相 | 提肛相 | 力排相 | 静息相 | 提肛相 | 力排相 | |||||||||||
| 轻度组 | 24 | 112.76±9.31 | 94.45±7.89 | 121.74±11.91 | 54.50±7.52 | 51.40±7.32 | 58.75±10.66 | 10.68±7.96 | 4.02±6.26 | 19.81±10.27 | |||||||||
| 重度组 | 11 | 127.45±15.71 | 107.97±17.22 | 122.90±16.63 | 55.15±7.91 | 53.30±8.85 | 57.56±9.27 | 14.10±6.96 | 7.24±12.36 | 18.44±12.69 | |||||||||
| t | 2.877* | 2.487* | 0.236 | 0.234 | 0.669 | 0.319 | 1.225 | 1.029 | 0.342 | ||||||||||
| 组别 | 耻骨直肠肌厚度/mm | 内括约肌厚度/mm | 外括约肌厚度/mm | ||||||||||||||||
| 静息相 | 提肛相 | 力排相 | 静息相 | 提肛相 | 力排相 | 静息相 | 提肛相 | 力排相 | |||||||||||
| 轻度组 | 5.20±1.68 | 6.12±1.63 | 5.38±1.42 | 2.85±0.81 | 2.95±0.85 | 2.64±0.71 | 3.68±1.42 | 4.06±1.41 | 3.54±1.19 | ||||||||||
| 重度组 | 5.65±1.79 | 6.05±1.94 | 5.65±1.54 | 2.25±0.38 | 2.87±0.40 | 2.65±0.74 | 3.39±0.85 | 3.67±0.84 | 3.75±0.99 | ||||||||||
| t | 0.736 | 0.098 | 0.510 | 2.343* | 0.286 | 0.065 | 0.621 | 1.008 | 0.516 | ||||||||||
Tab.3 Comparison of postoperative three phases of MRI indicators between mild and severe LARS patients
| 组别 | n | ARA/° | H线/mm | M线/mm | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 静息相 | 提肛相 | 力排相 | 静息相 | 提肛相 | 力排相 | 静息相 | 提肛相 | 力排相 | |||||||||||
| 轻度组 | 24 | 112.76±9.31 | 94.45±7.89 | 121.74±11.91 | 54.50±7.52 | 51.40±7.32 | 58.75±10.66 | 10.68±7.96 | 4.02±6.26 | 19.81±10.27 | |||||||||
| 重度组 | 11 | 127.45±15.71 | 107.97±17.22 | 122.90±16.63 | 55.15±7.91 | 53.30±8.85 | 57.56±9.27 | 14.10±6.96 | 7.24±12.36 | 18.44±12.69 | |||||||||
| t | 2.877* | 2.487* | 0.236 | 0.234 | 0.669 | 0.319 | 1.225 | 1.029 | 0.342 | ||||||||||
| 组别 | 耻骨直肠肌厚度/mm | 内括约肌厚度/mm | 外括约肌厚度/mm | ||||||||||||||||
| 静息相 | 提肛相 | 力排相 | 静息相 | 提肛相 | 力排相 | 静息相 | 提肛相 | 力排相 | |||||||||||
| 轻度组 | 5.20±1.68 | 6.12±1.63 | 5.38±1.42 | 2.85±0.81 | 2.95±0.85 | 2.64±0.71 | 3.68±1.42 | 4.06±1.41 | 3.54±1.19 | ||||||||||
| 重度组 | 5.65±1.79 | 6.05±1.94 | 5.65±1.54 | 2.25±0.38 | 2.87±0.40 | 2.65±0.74 | 3.39±0.85 | 3.67±0.84 | 3.75±0.99 | ||||||||||
| t | 0.736 | 0.098 | 0.510 | 2.343* | 0.286 | 0.065 | 0.621 | 1.008 | 0.516 | ||||||||||
| [1] | 姚宏伟, 李心翔, 崔龙, 等. 中国结直肠癌手术病例登记数据库2022年度报告:一项全国性登记研究[J]. 中国实用外科杂志, 2023, 43(1):93-99. |
| YAO H W, LI X X, CUI L, et al. Annual report of Chinese Colorectal Cancer Surgery Database in 2022:a nationwide registry study[J]. Chinese Journal of Practical Surgery, 2023, 43(1):93-99. doi:10.19538/j.cjps.issn1005-2208.2023.01.13. | |
| [2] | LIAO J, QIN H, WANG Z, et al. Mesorectal reconstruction with pedicled greater omental transplantation to relieve low anterior resection syndrome following total intersphincteric resection in patients with ultra-low rectal cancer[J]. BMC Surg, 2023, 23(1):236. doi:10.1186/s12893-023-02140-1. |
| [3] | 吴晓华, 牛志新, 何峰, 等. 320例老年直肠癌保肛术后低位前切除综合征的危险因素分析[J]. 临床消化病杂志, 2023, 35(4):316-319. |
| WU X H, NIU Z X, HE F, et al. Analysis of high risk factors of low anterior resection syndrome after anus-preserving surgery for elderly rectal cancer[J]. Chinese Journal of Clinical Gastroenterology, 2023, 35(4):316-319. doi:10.3870/lcxh.j.issn.1005-541X.2023.04.15. | |
| [4] | 陈锦垣, 王樱花, 李燕玲, 等. 静动态MRI测量肛提肌裂孔面积预测女性盆底功能障碍的价值研究[J]. 中国实用医药, 2023, 18(8):81-85. |
| CHEN J Y, WANG Y H, LI Y L, et al. A study on the value of static and dynamic MRI to measure levator hiatus area to predict female pelvic floor dysfunction[J]. China Practical Medicine, 2023, 18(8):81-85. doi:10.14163/j.cnki.11-5547/r.2023.08.024. | |
| [5] | SUN R, DAI Z, ZHANG Y, et al. The incidence and risk factors of low anterior resection syndrome (LARS) after sphincter-preserving surgery of rectal cancer: a systematic review and meta-analysis[J]. Support Care Cancer, 2021, 29(12):7249-7258. doi:10.1007/s00520-021-06326-2. |
| [6] | 闫晶晶, 牟绍玉, 谭人福, 等. 直肠癌低位前切除综合征评分表中文版的实证研究[J]. 解放军护理杂志, 2015, 32(4):12-15. |
| YAN J J, MOU S Y, TAN R F, et al. Empirical research of the Chinese Version of Low Anterior Resection Syndrome Score(LARS)[J]. Nursing Journal of Chinese People's Liberation Army, 2015, 32(4):12-15. doi:10.3969/j.issn.1008-9993.2015.04.003. | |
| [7] | 乔新华, 王砚丽, 张凤联. 直肠癌保肛术后低位前切除综合征研究进展[J]. 肿瘤预防与治疗, 2023, 36(1):68-74. |
| QIAO X H, WANG Y L, ZHANG F L. Low anterior resection syndrome of rectal cancer patients after anus-preserving surgery[J]. Journal of Cancer Control and Treatment, 2023, 36(1):68-74. doi:10.3969/j.issn.1674-0904.2023.01.011. | |
| [8] | MOON J, EHLEBRACHT A, CWINTAL M, et al. Low anterior resection syndrome in a reference North American population:prevalence,predictors,and association with quality of life[J]. Journal of the American College of Surgeons, 2021, 233(5):S58. doi:10.1016/j.jamcollsurg.2021.07.099. |
| [9] | 李洲, 马勇, 方仕旭, 等. 全直肠系膜切除术后低位前切除综合征的发生率及相关危险因素分析[J]. 肿瘤预防与治疗, 2022, 35(2):169-174. |
| LI Z, MA Y, FANG S X, et al. Incidence of low anterior resection syndrome after total mesorectal excision and its risk factors[J]. Journal of Cancer Control and Treatment, 2022, 35(2):169-174. doi:10.3969/j.issn.1674-0904.2022.02.011. | |
| [10] | 郭帆, 韩斌, 黄琳凯, 等. 腹腔镜直肠癌保肛根治术后低位前切除综合征的发生及影响因素分析[J]. 华中科技大学学报(医学版), 2021, 50(2):194-200. |
| GUO F, HAN B, HUANG L K, et al. Occurrence and influencing factors of low anterior resection syndrome after laparoscopic anus preserving radical resection of rectal cancer[J]. Acta Medicinae Universitatis Scientiae et Technologiae Huazhong, 2021, 50(2):194-200. doi:10.3870/j.issn.1672-0741.2021.02.011. | |
| [11] | 李雪, 耿学斯, 程一乘, 等. CGRP、AchE在功能性排便障碍大鼠模型中的表达[J]. 天津医药, 2020, 48(12):1169-1174,1255. |
| LI X, GENG X S, CHENG Y C, et al. The expressions of CGRP and AchE in a rat model of functional defecation disorder[J]. Tianjin Medical Journal, 2020, 48(12):1169-1174,1255. doi:10.11958/20201095. | |
| [12] | THANARACTHANON P, SASIWIMONPHAN K, SUNTHORNRAM A, et al. Diagnostic performance of dynamic MR defecography in assessment of dyssynergic defecation[J]. Abdom Radiol(NY), 2023, 48(11):3458-3468. doi: 10.1007/s00261-023-04010-z. |
| [13] | 薛霞, 李宽, 马黎飞, 等. 基于3D高分辨肛门直肠测压研究针刺对脊髓损伤神经源性肠道的疗效[J]. 中国康复, 2020, 35(1):35-38. |
| XUE X, LI K, MA L F, et al. Clinical effect of acupuncture on neurogenic bowel dysfunction after spinal cord injury based on 3D high-resolution anorectal manometry[J]. Chinese Journal of Rehabilitation, 2020, 35(1):35-38. doi:10.3870/zgkf.2020.01.009. | |
| [14] | 杨华盛, 邓罡, 徐丽姝. 功能性便秘排便障碍患者三维高分辨直肠测压的应用[J]. 实用医学杂志, 2021, 37(11):1456-1460. |
| YANG H S, DENG G, XU L S. Application of 3D high-resolution anorectal manometry in functional constipation caused by defecation disorders[J]. The Journal of Practical Medicine, 2021, 37(11):1456-1460. doi:10.3969/j.issn.1006-5725.2021.11.017. | |
| [15] | FATHY A H, FAROUK R E, NOHA M, et al. Urodynamics/lower urinary tract dysfunction/female pelvic medicine:pelvic prolapse[J]. The Journal of Urology, 2022, 207(Supplement 5):e708. doi:10.1097/JU.0000000000002605.01. |
| [16] | ZHANG X, XIANG Y, YAO J, et al. Automatic segmentation of the female pelvic floor muscles on MRI for pelvic floor function assessment[J]. Quant Imaging Med Surg, 2023, 13(7):4181-4195. doi:10.21037/qims-22-1198. |
| [17] | 刘广辉. 高分辨率MRI联合动态MRI在盆底功能障碍性疾病中的诊断价值[J]. 中国民康医学, 2022, 34(16):130-133. |
| LIU G H. Diagnostic value of high resolution MRI combined with dynamic MRI in pelvic floor dysfunction disease[J]. Medical Journal of Chinese People's Health, 2022, 34(16):130-133. doi:10.3969/j.issn.1672-0369.2022.16.039. | |
| [18] | GUPTA A P, PANDYA P R, NGUYEN M L, et al. Use of dynamic MRI of the pelvic floor in the assessment of anterior compartment disorders[J]. Curr Urol Rep, 2018, 19(12):112. doi:10.1007/s11934-018-0862-4. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||