Tianjin Medical Journal ›› 2025, Vol. 53 ›› Issue (12): 1270-1275.doi: 10.11958/20252583
• Clinical Research • Previous Articles Next Articles
XU Yong( ), SUN Jie(), HU Zongju
), SUN Jie(), HU Zongju
Received:2025-07-25
Revised:2025-09-10
Published:2025-12-15
Online:2025-12-08
Contact:
△E-mail:XU Yong, SUN Jie, HU Zongju. Analysis of influencing factors and construction of prediction model in patients with severe acute pancreatitis complicated with acute acalculous cholecystitis[J]. Tianjin Medical Journal, 2025, 53(12): 1270-1275.
CLC Number:
| 组别 | n | 年龄/岁 | 男性 | 吸烟 | 饮酒 | BMI/(kg/m2) | 禁食水时间/d | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非AAC组 | 156 | 52.35±7.38 | 108(69.23) | 53(33.97) | 70(44.87) | 23.18±1.94 | 7.63±2.08 | ||||||
| AAC组 | 64 | 54.17±8.83 | 41(64.06) | 24(37.50) | 21(32.81) | 22.69±2.07 | 10.25±2.87 | ||||||
| χ2或t | 1.459 | 0.555 | 0.248 | 2.721 | 1.644 | 6.621** | |||||||
| 组别 | SAP病因 | 基础疾病 | 脓毒症 | ||||||||||
| 高脂血症性 | 酒精性 | 特发性 | 其他 | 高血压 | 糖尿病 | ||||||||
| 非AAC组 | 56(35.90) | 60(38.46) | 23(14.74) | 17(10.90) | 58(37.18) | 24(15.38) | 23(14.74) | ||||||
| AAC组 | 26(40.63) | 15(23.44) | 10(15.63) | 13(20.31) | 30(46.88) | 16(25.00) | 18(28.13) | ||||||
| χ2 | 6.250 | 1.778 | 2.821 | 5.359* | |||||||||
Tab.1 Comparison of general clinical data between the 2 groups of patients
| 组别 | n | 年龄/岁 | 男性 | 吸烟 | 饮酒 | BMI/(kg/m2) | 禁食水时间/d | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 非AAC组 | 156 | 52.35±7.38 | 108(69.23) | 53(33.97) | 70(44.87) | 23.18±1.94 | 7.63±2.08 | ||||||
| AAC组 | 64 | 54.17±8.83 | 41(64.06) | 24(37.50) | 21(32.81) | 22.69±2.07 | 10.25±2.87 | ||||||
| χ2或t | 1.459 | 0.555 | 0.248 | 2.721 | 1.644 | 6.621** | |||||||
| 组别 | SAP病因 | 基础疾病 | 脓毒症 | ||||||||||
| 高脂血症性 | 酒精性 | 特发性 | 其他 | 高血压 | 糖尿病 | ||||||||
| 非AAC组 | 56(35.90) | 60(38.46) | 23(14.74) | 17(10.90) | 58(37.18) | 24(15.38) | 23(14.74) | ||||||
| AAC组 | 26(40.63) | 15(23.44) | 10(15.63) | 13(20.31) | 30(46.88) | 16(25.00) | 18(28.13) | ||||||
| χ2 | 6.250 | 1.778 | 2.821 | 5.359* | |||||||||
| 组别 | PLT/(×109/L) | PCT/(μg/L) | ALT/(U/L) | AST/(U/L) | TBil/(μmol/L) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 非AAC组 | 197.40±39.00 | 0.66±0.19 | 50.81±9.97 | 46.49±10.87 | 26.39±8.87 | ||||||
| AAC组 | 208.86±47.29 | 0.70±0.20 | 52.75±10.48 | 48.76±11.64 | 32.65±10.48 | ||||||
| t | 1.714 | 1.721 | 1.292 | 1.384 | 4.512** | ||||||
| 组别 | n | AMY/(U/L) | LIP/(U/L) | SIRI | CAR | WMR | |||||
| 非AAC组 | 156 | 535.75±101.39 | 413.86±87.29 | 5.06(3.98,6.62) | 3.68(2.67,4.81) | 1.19±0.23 | |||||
| AAC组 | 64 | 517.81±123.66 | 433.87±90.43 | 7.44(4.73,10.38) | 4.33(3.69,5.41) | 1.28±0.30 | |||||
| t或Z | 1.027 | 1.529 | 4.028** | 2.997** | 2.269* | ||||||
Tab.2 Comparison of laboratory indexes between the 2 groups of patients
| 组别 | PLT/(×109/L) | PCT/(μg/L) | ALT/(U/L) | AST/(U/L) | TBil/(μmol/L) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 非AAC组 | 197.40±39.00 | 0.66±0.19 | 50.81±9.97 | 46.49±10.87 | 26.39±8.87 | ||||||
| AAC组 | 208.86±47.29 | 0.70±0.20 | 52.75±10.48 | 48.76±11.64 | 32.65±10.48 | ||||||
| t | 1.714 | 1.721 | 1.292 | 1.384 | 4.512** | ||||||
| 组别 | n | AMY/(U/L) | LIP/(U/L) | SIRI | CAR | WMR | |||||
| 非AAC组 | 156 | 535.75±101.39 | 413.86±87.29 | 5.06(3.98,6.62) | 3.68(2.67,4.81) | 1.19±0.23 | |||||
| AAC组 | 64 | 517.81±123.66 | 433.87±90.43 | 7.44(4.73,10.38) | 4.33(3.69,5.41) | 1.28±0.30 | |||||
| t或Z | 1.027 | 1.529 | 4.028** | 2.997** | 2.269* | ||||||
| 变量 | β | SE | Wald χ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| 禁食水时间 | 0.444 | 0.089 | 25.005 | <0.001 | 1.559 | 1.310~1.855 |
| 脓毒症 | 0.559 | 0.467 | 1.430 | 0.232 | 1.748 | 0.700~4.366 |
| SIRI | 0.217 | 0.060 | 12.998 | <0.001 | 1.242 | 1.104~1.398 |
| CAR | 0.278 | 0.124 | 5.038 | 0.025 | 1.321 | 1.036~1.684 |
| WMR | 1.869 | 0.807 | 5.364 | 0.021 | 6.480 | 1.333~31.508 |
| TBil | 0.053 | 0.021 | 6.430 | 0.011 | 1.054 | 1.012~1.098 |
| 常数项 | -11.364 | 1.751 | 42.100 | <0.001 | 0.000 |
Tab.3 Multivariate Logistic regression analysis of AAC in patients with SAP
| 变量 | β | SE | Wald χ2 | P | OR | OR 95%CI |
|---|---|---|---|---|---|---|
| 禁食水时间 | 0.444 | 0.089 | 25.005 | <0.001 | 1.559 | 1.310~1.855 |
| 脓毒症 | 0.559 | 0.467 | 1.430 | 0.232 | 1.748 | 0.700~4.366 |
| SIRI | 0.217 | 0.060 | 12.998 | <0.001 | 1.242 | 1.104~1.398 |
| CAR | 0.278 | 0.124 | 5.038 | 0.025 | 1.321 | 1.036~1.684 |
| WMR | 1.869 | 0.807 | 5.364 | 0.021 | 6.480 | 1.333~31.508 |
| TBil | 0.053 | 0.021 | 6.430 | 0.011 | 1.054 | 1.012~1.098 |
| 常数项 | -11.364 | 1.751 | 42.100 | <0.001 | 0.000 |
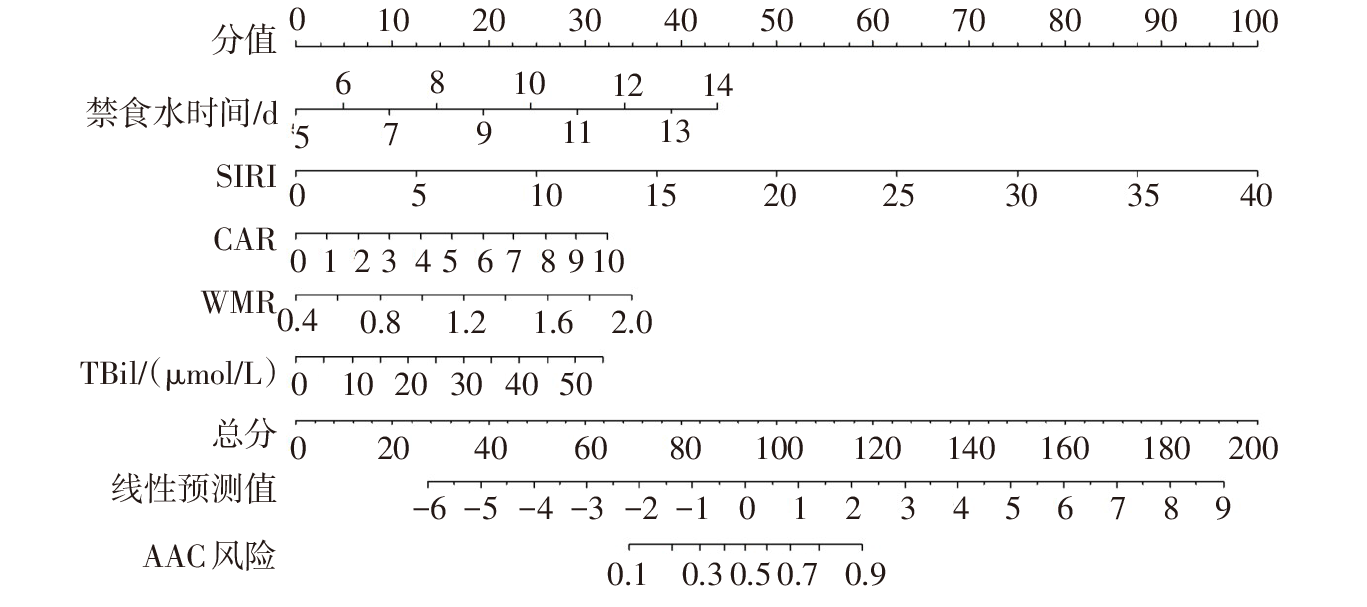
Fig.1 The nomogram of the prediction model for AAC in patients with SAP
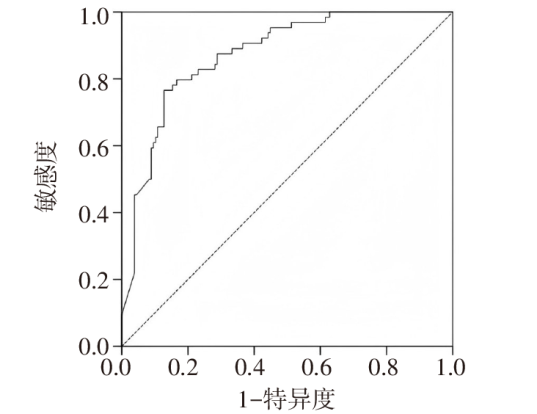
Fig.2 ROC curve of the nomogram prediction model for AAC in patients with SAP
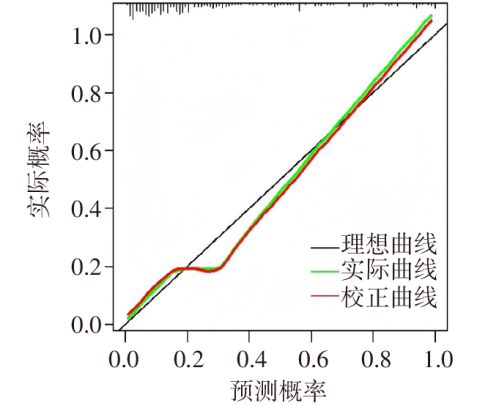
Fig.3 The calibration curve of the nomogram prediction model for AAC in patients with SAP
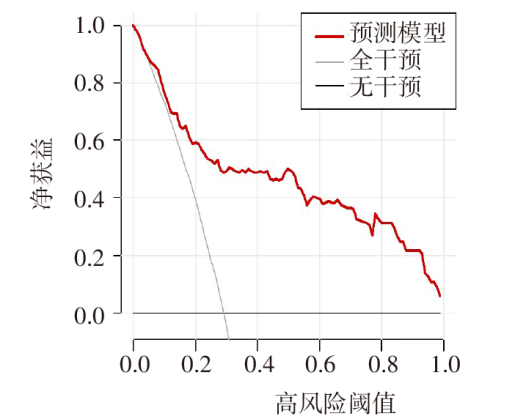
Fig.4 The DCA curve of the nomogram prediction model for AAC in patients with SAP
| [1] | HAMESCH K, HOLLENBACH M, GUILABERT L, et al. Practical management of severe acute pancreatitis[J]. Eur J Intern Med, 2025, 133:1-13. doi:10.1016/j.ejim.2024.10.030. |
| [2] | RODRIGUES T, BOIKE J R. Biliary strictures:etiologies and medical management[J]. Semin Intervent Radiol, 2021, 38(3):255-262. doi:10.1055/s-0041-1731086. |
| [3] | MORIKAWA T, AKADA M, SHIMIZU K, et al. Current status and therapeutic strategy of acute acalculous cholecystitis:Japanese nationwide survey in the era of the Tokyo guidelines[J]. J Hepatobiliary Pancreat Sci, 2024, 31(3):162-172. doi:10.1002/jhbp.1401. |
| [4] | 李启元, 罗岩, 孙备. 急性胰腺炎并发胆道系统疾病的诊治进展[J]. 中华外科杂志, 2025, 63(1):76-80. |
| LI Q Y, LUO Y, SUN B. Progress in the diagnosis and treatment of acute pancreatitis complicated by biliary tract diseases[J]. Chin J Surg, 2025, 63(1):76-80. doi:10.3760/cma.j.cn112139-20240708-00330. | |
| [5] | MOSSAAB G, BEN KHLIFA M, KARIM N, et al. Acute acalculous cholecystitis in hospitalized patients in intensive care unit:study of 5 cases[J]. Heliyon, 2022, 8(11):e11524. doi:10.1016/j.heliyon.2022.e11524. |
| [6] | ISLAM M M, SATICI M O, EROGLU S E. Unraveling the clinical significance and prognostic value of the neutrophil-to-lymphocyte ratio,platelet-to-lymphocyte ratio,systemic immune-inflammation index,systemic inflammation response index,and delta neutrophil index:an extensive literature review[J]. Turk J Emerg Med, 2024, 24(1):8-19. doi:10.4103/tjem.tjem_198_23. |
| [7] | LIU J, CHEN X, YANG M, et al. C-reactive protein to albumin ratio as a prognostic tool for predicting intravenous immunoglobulin resistance in children with Kawasaki disease:a systematic review of cohort studies[J]. Pediatr Rheumatol Online J, 2024, 22(1):42. doi:10.1186/s12969-024-00980-6. |
| [8] | WANG Y, MIAO Y, WAN Q. Association of white blood cell count to mean platelet volume ratio with type 2 diabetic peripheral neuropathy in a Chinese population:a cross-sectional study[J]. BMC Endocr Disord, 2024, 24(1):129. doi:10.1186/s12902-024-01644-y. |
| [9] | 中华医学会外科学分会胰腺外科学组. 中国急性胰腺炎诊治指南(2021)[J]. 中华外科杂志, 2021, 59(7):578-587. |
| Study Group of Pancreatic Surgery in China Society of Surgery of Chinese Medical Association. Chinese guidelines for the management of acute pancreatitis(2021)[J]. Chin J Surg, 2021, 59(7):578-587. doi:10.3760/cma.j.cn112139-20210416-00172. | |
| [10] | YOKOE M, HATA J, TAKADA T, et al. Tokyo Guidelines 2018:diagnostic criteria and severity grading of acute cholecystitis (with videos)[J]. J Hepatobiliary Pancreat Sci, 2018, 25(1):41-54. doi:10.1002/jhbp.515. |
| [11] | HUANG S S, LIN K W, LIU K L, et al. Diagnostic performance of ultrasound in acute cholecystitis:a systematic review and meta-analysis[J]. World J Emerg Surg, 2023, 18(1):54. doi:10.1186/s13017-023-00524-5. |
| [12] | 刘振, 张旭, 张保平, 等. 内镜下逆行胰胆管造影术后非结石性急性胆囊炎风险因素分析[J]. 中国实用外科杂志, 2024, 44(10):1165-1170. |
| LIU Z, ZHANG X, ZHANG B P, et al. Study on risk factors of post-endoscopic retrograde cholangiopancreatography acalculous acute cholecystitis[J]. Chin J Pract Surg, 2024, 44(10):1165-1170. doi:10.19538/j.cjps.issn1005-2208.2024.10.17. | |
| [13] | UWATOKO R, KANI N, MAKINO S, et al. Shiga toxin-producing Escherichia coli-associated hemolytic uremic syndrome with recurrent acute cholecystitis:a case report[J]. CEN Case Rep, 2024, 13(3):215-219. doi:10.1007/s13730-023-00831-5. |
| [14] | 李启元, 罗岩, 陈华, 等. 重症急性胰腺炎并发胆道系统疾病的临床特征及危险因素分析[J]. 中华外科杂志, 2025, 63(8):712-719. |
| LI Q Y, LUO Y, CHEN H, et al. Analysis of clinical features and risk factors for severe acute pancreatitis complicated with biliary system diseases[J]. Chin J Surg, 2025, 63(8):712-719. doi:10.3760/cma.j.cn112139-20250217-00080. | |
| [15] | GALLAHER J R, CHARLES A. Acute cholecystitis:a review[J]. JAMA, 2022, 327(10):965-975. doi:10.1001/jama.2022.2350. |
| [16] | 赵经委, 侯煜铖, 杨自逸, 等. 肠道菌群在胆道良性疾病中致病作用的全基因组孟德尔随机化研究[J]. 中华外科杂志, 2024, 62(3):216-222. |
| ZHAO J W, HOU Y C, YANG Z Y, et al. Genome-wide Mendelian randomization study of the pathogenic role of gut microbiota in benign biliary tract diseases[J]. Chin J Surg, 2024, 62(3):216-222. doi:10.3760/cma.j.cn112139-20230714-00008. | |
| [17] | JIN X, JIANG Y, TANG J. Ultrasound-guided percutaneous transhepatic gallbladder drainage improves the prognosis of patients with severe acute cholecystitis[J]. Evid Based Complement Alternat Med, 2022,2022:5045869. doi:10.1155/2022/5045869. |
| [18] | 董丹, 陈立娟, 俞荷花. 急性胰腺炎并发低血压的危险因素分析及预测模型建立[J]. 天津医药, 2025, 53(5):509-513. |
| DONG D, CHEN L J, YU H H. Analysis of risk factors and establishment of prediction model of acute pancreatitis complicated with hypotension[J]. Tianjin Med J, 2025, 53(5):509-513. doi:10.11958/20250456. | |
| [19] | 鲍布和, 张琪, 李海林, 等. 血常规比值参数在类风湿关节炎中的诊断价值[J]. 天津医药, 2023, 51(11):1271-1275. |
| BAO B H, ZHANG Q, LI H L, et al. Diagnostic value of blood cell count-derived ratio parameters in rheumatoid arthritis[J]. Tianjin Med J, 2023, 51(11):1271-1275. doi:10.11958/20230481. | |
| [20] | 徐家丹, 戴签, 王中新. 全身免疫炎症指数对中度重症和重症急性胰腺炎的预测价值[J]. 重庆医学, 2023, 52(14):2175-2179. |
| XU J D, DAI Q, WANG Z X. Predictive value of systemic immune inflammation index for moderate-severe and severe acute pancreatitis[J]. Chongqing Med, 2023, 52(14):2175-2179. doi:10.3969/j.issn.1671-8348.2023.14.017. | |
| [21] | FU Y, PANG L, DAI W, et al. Advances in the study of acute acalculous cholecystitis:a comprehensive review[J]. Dig Dis, 2022, 40(4):468-478. doi:10.1159/000520025. |
| [22] | CAKCAK İ E, KULA O. Predictive evaluation of SIRI,SII,PNI,and GPS in cholecystostomy application in patients with acute cholecystitis[J]. Ulus Travma Acil Cerrahi Derg, 2022, 28(7):940-946. doi:10.14744/tjtes.2022.90249. |
| [23] | 付玉茹, 孙振康, 刘成, 等. C反应蛋白/白蛋白比值与重症肺炎患者病情严重程度的关系及其对28 d死亡风险的预测价值[J]. 解放军医学杂志, 2025, 50(3):309-317. |
| FU Y R, SUN Z K, LIU C, et al. Relationship between C-reactive protein/albumin ratio and severity in patients with severe pneumonia and its predictive value for 28-day mortality risk[J]. Med J Chin PLA, 2025, 50(3):309-317. doi:10.11855/j.issn.0577-7402.0345.2024.1215. | |
| [24] | BOCCATONDA A, CAMPELLO E, TALLARICO V, et al. Splanchnic venous thrombosis in patients with acute cholecystitis:a case series and review of literature[J]. J Ultrasound, 2025, 28(3):551-561. doi:10.1007/s40477-025-01029-4. |
| [25] | ÖZDEMIR S, ALTUNOK I, ÖZKAN A, et al. Relationship between platelet indices in acute cholecystitis:a case-control study[J]. Rev Gastroenterol Mex(Engl Ed), 2024, 89(2):232-236. doi:10.1016/j.rgmxen.2023.04.012. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||