Tianjin Medical Journal ›› 2026, Vol. 54 ›› Issue (5): 522-527.doi: 10.11958/20252631
• Clinical Research • Previous Articles Next Articles
YU Bo1( ), PU Xiaolin1, LIU Naiting1, LI Yabin2, WU Zhiru3
), PU Xiaolin1, LIU Naiting1, LI Yabin2, WU Zhiru3
Received:2025-08-04
Revised:2026-02-04
Published:2026-05-15
Online:2026-05-13
YU Bo, PU Xiaolin, LIU Naiting, LI Yabin, WU Zhiru. Analysis of risk factors for delayed bleeding in patients with gastrointestinal mucosal tumors after EMR[J]. Tianjin Medical Journal, 2026, 54(5): 522-527.
CLC Number:
| 组别 | n | 年龄/岁 | 男性 | 合并基础病 | 肿瘤直径/cm | 肿瘤部位 | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 高血压 | 糖尿病 | 冠心病 | 胃窦 | 胃体 | 贲门胃底 | 结肠 | 直肠 | ||||||||||||||||||||||
| 未出血组 | 320 | 61.78±8.18 | 161(50.3) | 37(11.6) | 21(6.6) | 25(7.8) | 4.26±1.24 | 36(11.2) | 122(38.1) | 51(38.1) | 69(21.6) | 42(13.1) | |||||||||||||||||
| 出血组 | 160 | 66.78±8.43 | 81(50.6) | 34(21.2) | 11(6.9) | 13(8.1) | 4.82±1.23 | 18(11.3) | 61(38.1) | 26(16.3) | 35(21.9) | 20(12.5) | |||||||||||||||||
| t或χ2 | 6.248** | 0.004 | 7.942** | 0.017 | 0.014 | 4.646** | 0.044 | ||||||||||||||||||||||
| 组别 | 肿瘤良恶性 | 术前 PT/s | 术前 APTT/s | 术前PLT/ (×109/L) | 抗凝药物 停药时间/d | 术前活检 次数/次 | 切除 面积/cm2 | 术中出血 | |||||||||||||||||||||
| 良性 | 恶性 | ||||||||||||||||||||||||||||
| 未出血组 | 256(80.0) | 64(20.0) | 12.11±1.02 | 29.98±2.39 | 215.36±44.53 | 4.74±1.30 | 2.00(1.00,3.00) | 4.26±1.43 | 50(15.6) | ||||||||||||||||||||
| 出血组 | 128(80.0) | 32(20.0) | 12.37±1.15 | 30.20±2.47 | 216.32±49.53 | 5.30±1.72 | 3.00(2.00,4.00) | 4.91±1.65 | 72(45.0) | ||||||||||||||||||||
| t、χ2或Z | 0.000 | 2.547* | 0.948 | 0.213 | 3.968** | 5.779** | 4.474** | 48.554** | |||||||||||||||||||||
| 组别 | 术中 使用钛夹 | 钛夹使用 数量/枚 | 钛夹类型 | 术中使用 肾上腺素 | 术后应用 抗凝药 | 术后抗凝药物 持续时间/d | |||||||||||||||||||||||
| 金属 | 可吸收 | ||||||||||||||||||||||||||||
| 未出血组 | 84(26.2) | 2.12±0.73 | 50(15.6) | 270(84.4) | 97(30.3) | 199(62.2) | 5.03±1.29 | ||||||||||||||||||||||
| 出血组 | 42(26.3) | 2.18±0.79 | 28(17.5) | 132(82.5) | 49(30.6) | 28(93.7) | 5.34±1.99 | ||||||||||||||||||||||
| t或χ2 | 0.000 | 0.775 | 0.276 | 0.005 | 85.455** | 2.052** | |||||||||||||||||||||||
Tab.1 Comparison of general data between the bleeding group and the non-bleeding group
| 组别 | n | 年龄/岁 | 男性 | 合并基础病 | 肿瘤直径/cm | 肿瘤部位 | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 高血压 | 糖尿病 | 冠心病 | 胃窦 | 胃体 | 贲门胃底 | 结肠 | 直肠 | ||||||||||||||||||||||
| 未出血组 | 320 | 61.78±8.18 | 161(50.3) | 37(11.6) | 21(6.6) | 25(7.8) | 4.26±1.24 | 36(11.2) | 122(38.1) | 51(38.1) | 69(21.6) | 42(13.1) | |||||||||||||||||
| 出血组 | 160 | 66.78±8.43 | 81(50.6) | 34(21.2) | 11(6.9) | 13(8.1) | 4.82±1.23 | 18(11.3) | 61(38.1) | 26(16.3) | 35(21.9) | 20(12.5) | |||||||||||||||||
| t或χ2 | 6.248** | 0.004 | 7.942** | 0.017 | 0.014 | 4.646** | 0.044 | ||||||||||||||||||||||
| 组别 | 肿瘤良恶性 | 术前 PT/s | 术前 APTT/s | 术前PLT/ (×109/L) | 抗凝药物 停药时间/d | 术前活检 次数/次 | 切除 面积/cm2 | 术中出血 | |||||||||||||||||||||
| 良性 | 恶性 | ||||||||||||||||||||||||||||
| 未出血组 | 256(80.0) | 64(20.0) | 12.11±1.02 | 29.98±2.39 | 215.36±44.53 | 4.74±1.30 | 2.00(1.00,3.00) | 4.26±1.43 | 50(15.6) | ||||||||||||||||||||
| 出血组 | 128(80.0) | 32(20.0) | 12.37±1.15 | 30.20±2.47 | 216.32±49.53 | 5.30±1.72 | 3.00(2.00,4.00) | 4.91±1.65 | 72(45.0) | ||||||||||||||||||||
| t、χ2或Z | 0.000 | 2.547* | 0.948 | 0.213 | 3.968** | 5.779** | 4.474** | 48.554** | |||||||||||||||||||||
| 组别 | 术中 使用钛夹 | 钛夹使用 数量/枚 | 钛夹类型 | 术中使用 肾上腺素 | 术后应用 抗凝药 | 术后抗凝药物 持续时间/d | |||||||||||||||||||||||
| 金属 | 可吸收 | ||||||||||||||||||||||||||||
| 未出血组 | 84(26.2) | 2.12±0.73 | 50(15.6) | 270(84.4) | 97(30.3) | 199(62.2) | 5.03±1.29 | ||||||||||||||||||||||
| 出血组 | 42(26.3) | 2.18±0.79 | 28(17.5) | 132(82.5) | 49(30.6) | 28(93.7) | 5.34±1.99 | ||||||||||||||||||||||
| t或χ2 | 0.000 | 0.775 | 0.276 | 0.005 | 85.455** | 2.052** | |||||||||||||||||||||||
| 变量 | β | SE | Wald χ2 | P | OR | OR95%CI |
|---|---|---|---|---|---|---|
| 年龄 | 0.080 | 0.014 | 31.645 | <0.001 | 1.084 | 1.057~1.114 |
| 术前活检次数 | 0.464 | 0.107 | 25.253 | <0.001 | 1.709 | 1.387~2.107 |
| 术中出血 | 1.645 | 0.246 | 44.802 | <0.001 | 5.179 | 3.199~8.382 |
| 常数项 | -7.677 | 0.994 | 59.696 | <0.001 | 0.000 | - |
Tab.2 Influencing factors of delayed bleeding in patients with gastrointestinal mucosal tumors at 30d after EMR
| 变量 | β | SE | Wald χ2 | P | OR | OR95%CI |
|---|---|---|---|---|---|---|
| 年龄 | 0.080 | 0.014 | 31.645 | <0.001 | 1.084 | 1.057~1.114 |
| 术前活检次数 | 0.464 | 0.107 | 25.253 | <0.001 | 1.709 | 1.387~2.107 |
| 术中出血 | 1.645 | 0.246 | 44.802 | <0.001 | 5.179 | 3.199~8.382 |
| 常数项 | -7.677 | 0.994 | 59.696 | <0.001 | 0.000 | - |
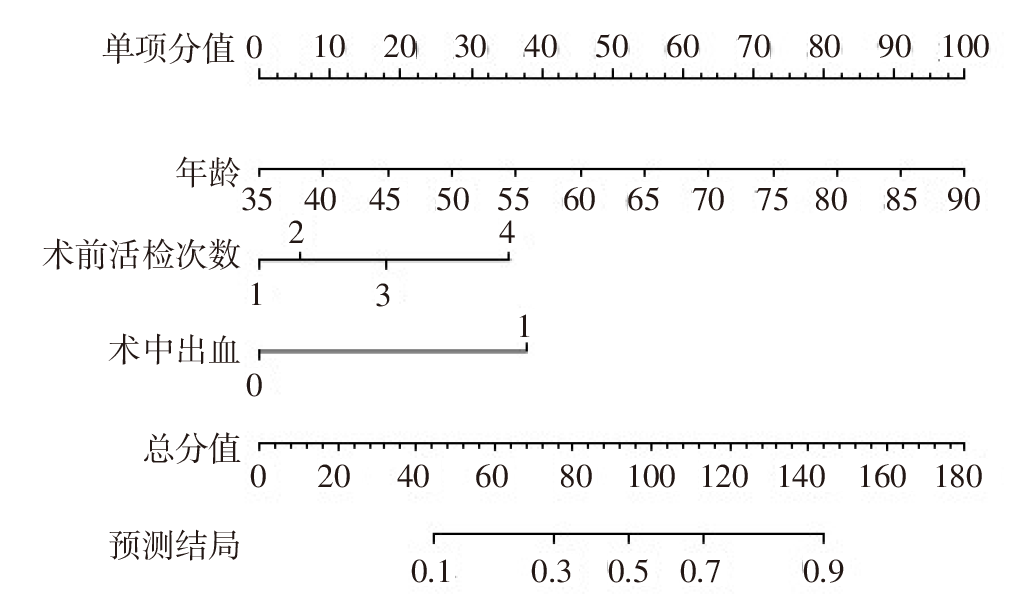
Fig.1 Nomogram to predict the risk of delayed bleeding in patients with gastrointestinal mucosal tumors after EMR
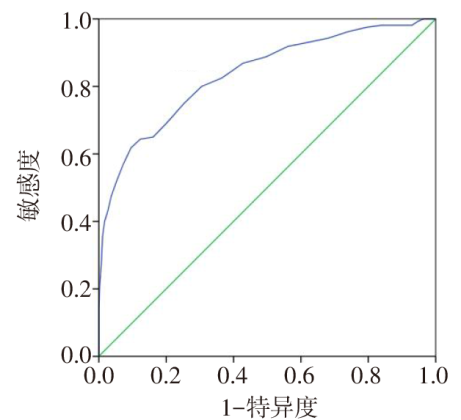
Fig.2 ROC curves of nomogram model for predicting delayed bleeding in patients with gastrointestinal mucosal tumors after EMR
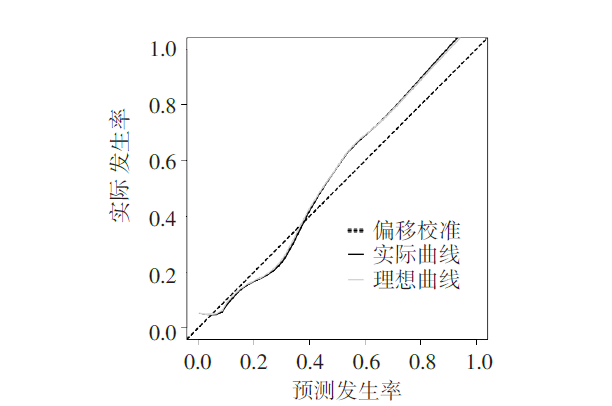
Fig.3 Calibration curves of the nomogram model for predicting delayed bleeding in patients with gastrointestinal mucosal tumors after EMR
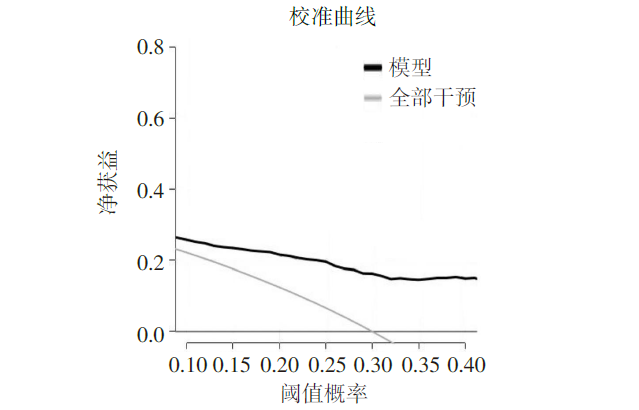
Fig.4 Clinical decision curves of the nomogram model for predicting delayed bleeding in patients with gastrointestinal mucosal tumors after EMR
| [1] | ISAKOV V. Machine learning in colorectal polyp surveillance:a paradigm shift in post-endoscopic mucosal resection follow-up[J]. World J Gastroenterol, 2025, 31(19):1-9. doi:10.3748/wjg.v31.i19.106628. |
| [2] | SHI Y H, LIU J L, CHENG C C, et al. Construction and validation of machine learning-based predictive model for colorectal polyp recurrence one year after endoscopic mucosal resection[J]. World J Gastroenterol, 2025, 31(11):1023-1025. doi:10.3748/wjg.v31.i11.102387. |
| [3] | ZHOU C, ZHANG F, WE Y. Efficacy of endoscopic mucosal resection versus endoscopic submucosal dissection for rectal neuroendocrine tumors ≤10 mm:a systematic review and meta-analysis[J]. Ann Saudi Med, 2023, 43(3):179-195. doi:10.5144/0256-4947.2023.179. |
| [4] | HAYASHI K, HAYASHI S, PASSERA R, et al. Endoscopic resection versus laparoscopic resection for gastric submucosal tumors:a systematic review and meta-analysis of safety and efficacy[J]. Asian J Endosc Surg, 2025, 18(1):e70104. doi:10.1111/ases.70104. |
| [5] | TURAN A S, MOONS L M G, SCHREUDER R M, et al. Clip placement to prevent delayed bleeding after colonic endoscopic mucosal resection(CLIPPER):study protocol for a randomized controlled trial[J]. Trials, 2021, 22(1):63. doi:10.1186/s13063-020-04996-7. |
| [6] | 梁文英, 陈淑华, 彭岚. 结肠息肉内镜下黏膜切除术后迟发性出血预测模型构建与验证[J]. 当代护士, 2025, 32(21):98-102. |
| LIANG W Y, CHEN S H, PENG L. Construction and validation of the predictive model for delayed bleeding in colonic polyps after endoscopic mucosal resection[J]. Modern Nurse, 2025, 32(21):98-102. doi:10.19793/j.cnki.1006-6411.2025.21.022. | |
| [7] | 周平红, 钟芸诗, 李全林, 等. 中国消化道黏膜下肿瘤内镜诊治专家共识(2023版)[J]. 中国实用外科杂志, 2023, 40(3):241-251. |
| ZHOU P H, ZHONG Y S, LI Q L, et al. Chinese consensus on endoscopic diagnosis and managment of gastrointestinal submucosal tumors(version 2023)[J]. Chin J Pract Surg, 2023, 40(3):241-251. doi:10.3760/cma.j.cn321463-20230310-00039. | |
| [8] | 杨桂凤, 虞敏亚, 杨雪兰. 个体化预测早期消化道肿瘤ESD术后迟发性出血风险的列线图模型的建立[J]. 中华现代护理杂志, 2021, 27(2):164-170. |
| YANG G F, YU M Y, YANG X L. Establishment of a Nomogram model for individualized prediction of the risk of delayed bleeding after endoscopic submucosal dissection for early gastrointestinal tumors[J]. Chinese Journal of Modern Nursing, 2021, 27(2):164-170. doi:10.3760/cma.j.cn115682-20200515-03365. | |
| [9] | KODAMA M. Editorial for delayed perforation after colorectal cold snare polypectomy with simultaneously performed endoscopic submucosal dissection:a case report and literature Review[J]. JMA J, 2025, 8(3):979-980. doi:10.31662/jmaj.2025-0262. |
| [10] | ALBOUYS J, MONTORI PINA S, BOUKECHICHE S, et al. Risk of delayed bleeding after colorectal endoscopic submucosal dissection: the limoges bleeding score[J]. Endoscopy, 2024, 56(2):110-118. doi:10.1055/a-2189-0807. |
| [11] | SUGIMOTO M, MURATA M, KAWAI T. Assessment of delayed bleeding after endoscopic submucosal dissection of early-stage gastrointestinal tumors in patients receiving direct oral anticoagulants[J]. World J Gastroenterol, 2023, 29(19):2916-2931. doi:10.3748/wjg.v29.i19.2916. |
| [12] | 刘荣泉, 季云, 张杰. 消化道早癌患者内镜黏膜下剥离术后迟发性出血的危险因素分析[J]. 中国现代医学杂志, 2023, 33(24):80-86. |
| LIU R Q, JI Y, ZHANG J. Risk factors for delayed bleeding after endoscopic submucosal dissection in patients with early cancer of the gastrointestinal tract[J]. Chin J Modern Med, 2023, 33(24):80-86. doi:10.3969/j.issn.1005-8982.2023.24.014. | |
| [13] | 杨真真, 贺馨, 潘晓林, 等. 消化道病变内镜黏膜下剥离术后创面处理的研究进展[J]. 中国实用内科杂志, 2023, 43(7):599-603. |
| YANG Z Z, HE X, PAN X L, et al. Research progress on wound management after endoscopic submucosal dissection of digestive tract diseases[J]. Chin J Pract Int Med, 2023, 43(7):599-603. doi:10.19538/j.nk2023070114. | |
| [14] | FERLITSCH M, HASSAN C, BISSCHOPS R, et al. Colorectal polypectomy and endoscopic mucosal resection: European Society of Gastrointestinal Endoscopy(ESGE)guideline - update 2024[J]. Endoscopy, 2024, 56(7):516-545. doi:10.1055/a-2304-3219. |
| [15] | 杨柳, 郑舒丹. ESD与EMR治疗早期结直肠癌、癌前病变的手术效果及并发症观察[J]. 河北医科大学学报, 2024, 45(2):159-164. |
| YANG L, ZHENG S D. Surgical effect and complications of ESD and EMR in the treatment of colorectal cancer and precancerous lesions[J]. J Hebei Med Univ, 2024, 45(2):159-164. doi:10.3969/j.issn.1007-3205.2024.02.007. | |
| [16] | LI W F, LAI B, LV L, et al. Complete closure utilizing titanium clips minimizes delayed postpolypectomy bleeding after colorectal endoscopic mucosal resection: a retrospective analysis[J]. Ther Adv Gastroenterol, 2025, 18:17562848251332836. doi:10.1177/17562848251332836. |
| [17] | 王睿, 赵海艳, 刘雪. 内镜黏膜下剥离术与内镜下黏膜切除术治疗早期食管癌的临床效果对比[J]. 实用癌症杂志, 2023, 38(6):930-932,945. |
| WANG R, ZHAO H Y, LIU X. Clinical comparison of endoscopic submucosal dissection and endoscopic mucosal resection in the treatment of early esophageal cancer[J]. Pract J Cancer, 2023, 38(6):930-932,945. doi:10.3969/j.issn.1001-5930.2023.06.016. | |
| [18] | 闫真, 孙亚梅, 高峰, 等. 结肠息肉内镜黏膜切除术后迟发性出血的危险因素分析[J]. 中国医药导报, 2023, 20(17):132-135. |
| YAN Z, SUN Y M, GAO F, et al. Analysis on risk factors of delayed bleeding after endoscopic mucosal resection of colon polyps[J]. China Medical Herald, 2023, 20(17):132-135. doi:10.20047/j.issn1673-7210.2023.17.30. | |
| [19] | 中华医学会消化内镜分会NOTES、外科学组,中国医师协会内镜医师分会消化内镜专业委员会,中华医学会外科学分会胃肠外科学组. 中国消化道黏膜下肿瘤内镜诊治专家共识(2023版)[J]. 中国实用外科杂志, 2023, 43(3):241-251. |
| NOTES and Endoscopic Surgery Group,Chinese Society of Digestive Endoscopology, Chinese Medical Association; Digestive Endoscopy Special Committee,Endoscopic Physicians Branch of Chinese Medical Doctor Association; Chinese Society of Gastrointestinal Surgery,Chinese Society of Surgery,Chinese Medical Association. Chinese consensus on endoscopic diagnosis and managment of gastrointestinal submucosal tumors(version 2023)[J]. Chin J Pract Surg, 2023, 43(3):241-251. doi:10.19538/j.cjps.issn1005-2208.2023.03.01. | |
| [20] | 鲁传和, 许复成, 袁海波. 直立位金属钛夹夹闭方式对结直肠息肉EMR后迟发性出血的影响及相关因素分析[J]. 临床和实验医学杂志, 2024, 23(6):614-618. |
| LU C H, XU F C, YUAN H B. Effect of upright titanium clamping on delayed bleeding after EMR colorectal polyps and related factors[J]. Journal of Clinical and Experimental Medicine, 2024, 23(6):614-618. doi:10.3969/j.issn.1671-4695.2024.06.015. | |
| [21] | 王超, 徐顺利, 林国安, 等. 超薄刃厚MEEK皮片修复大面积深度烧伤创面疗效分析[J]. 河南外科学杂志, 2025, 31(5):30-33. |
| WANG C, XU S L, LIN G A, et al. Efficacy of ultrathin split-thickness MEEK flap in the repair of extensively deep burn wounds[J]. Henan J Surg, 2025, 31(5):30-33. doi:10.3969/j.issn.1007-8991.2025.05.010. | |
| [22] | 杨舒悦, 邵琳琳, 赵正, 等. 国产与进口止血夹预防≥10 mm结直肠息肉内镜切除术后迟发性出血的效果对比[J]. 中华消化内镜杂志, 2023, 40(4):270-275. |
| YANG S Y, SHAO L L, ZHAO Z, et al. Comparison of domestic and imported hemostatic clips in preventing delayed post-polypectomy bleeding after endoscopic resection of colorectal polyps larger than 10 mm[J]. Chinese Journal of Digestive Endoscopy, 2023, 40(4):270-275. doi:10.3760/cma.j.cn321463-20220413-00644. | |
| [23] | 申艳, 陈欣, 武涛, 等. 肝硬化患者门静脉血栓形成合并消化道出血的研究进展[J]. 临床肝胆病杂志, 2022, 38(8):1901-1905. |
| SHEN Y, CHEN X, WU T, et al. Research advances in the treatment of portal vein thrombosis and gastrointestinal bleeding in patients with liver cirrhosis[J]. Chin J Clin Hepatol, 2022, 38(8):1901-1905. doi:10.3969/j.issn.1001-5256.2022.08.036. | |
| [24] | 叶冠男, 张嘉怡, 周震, 等. 抗血栓治疗对大结肠息肉患者内镜下黏膜切除术后迟发性出血的影响[J]. 中国普通外科杂志, 2023, 32(9):1426-1432. |
| YE G N, ZHANG J Y, ZHOU Z, et al. Impact of antithrombotic therapy on delayed postoperative bleeding in patients with large colonic polyps undergoing endoscopic mucosal resection[J]. Chin J Gen Surg, 2023, 32(9):1426-1432. doi:10.7659/j.issn.1005-6947.2023.09.018. | |
| [25] | MIYAKAWA A, TAMARU Y, MIZUMOTO T, et al. Prophylactic clip closure after endoscopic submucosal dissection of large flat and sessile colorectal polyps:a multicentre randomised controlled trial(EPOC trial)[J]. Gut, 2025, 74(11):1814-1820. doi:10.1136/gutjnl-2024-334463. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||